Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (3): 521-529. doi: 10.19723/j.issn.1671-167X.2023.03.019
Previous Articles Next Articles
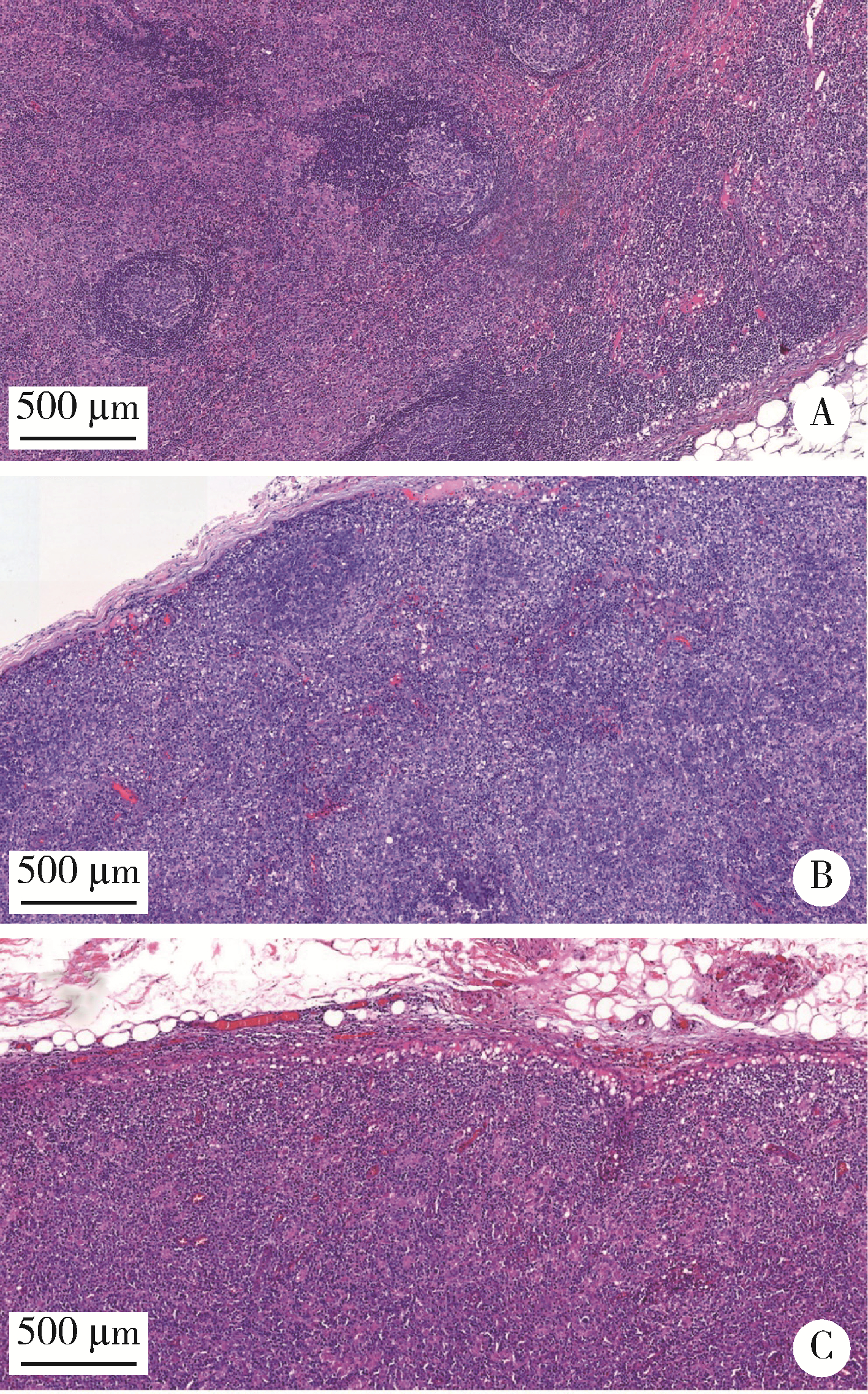
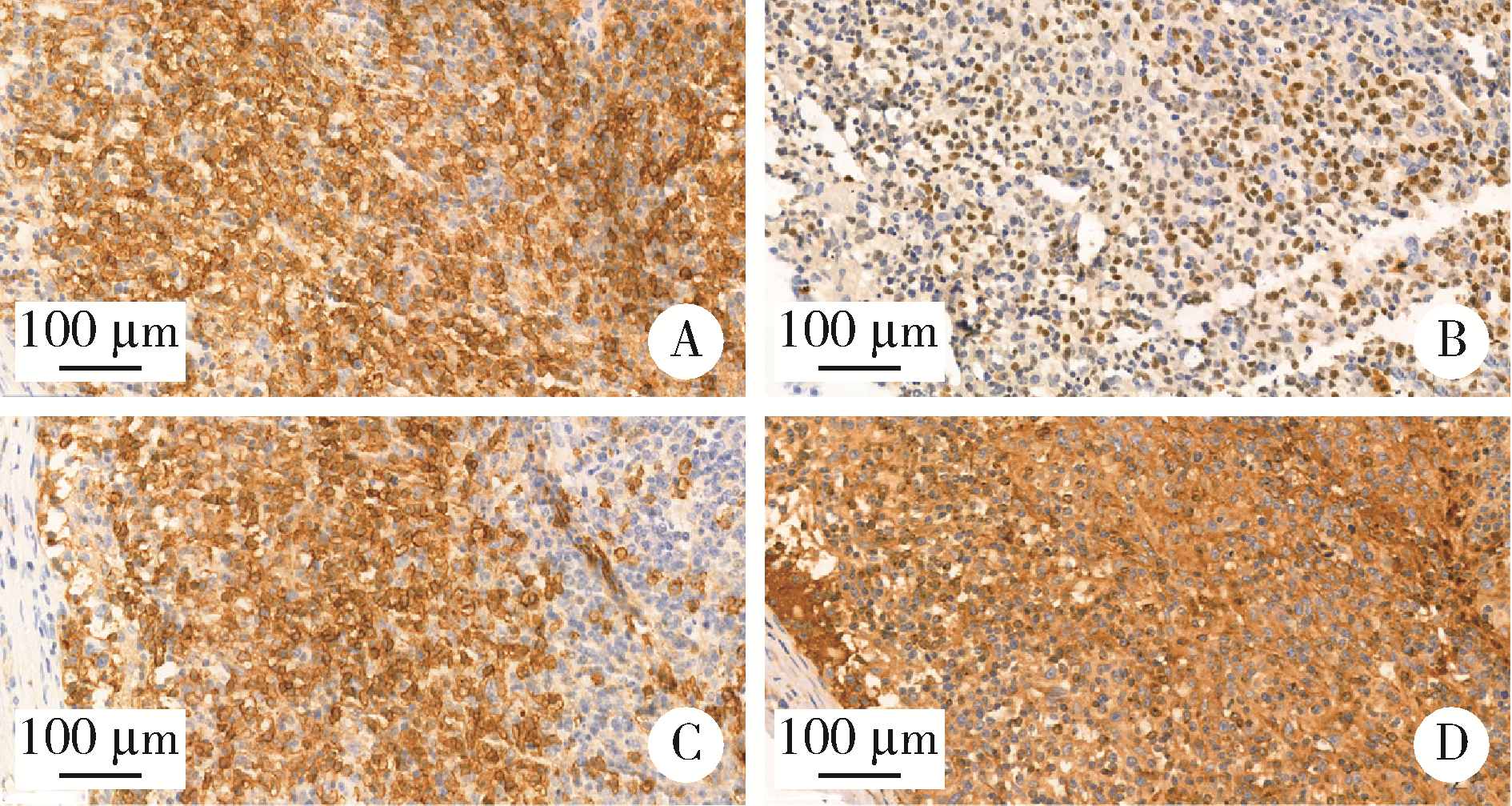
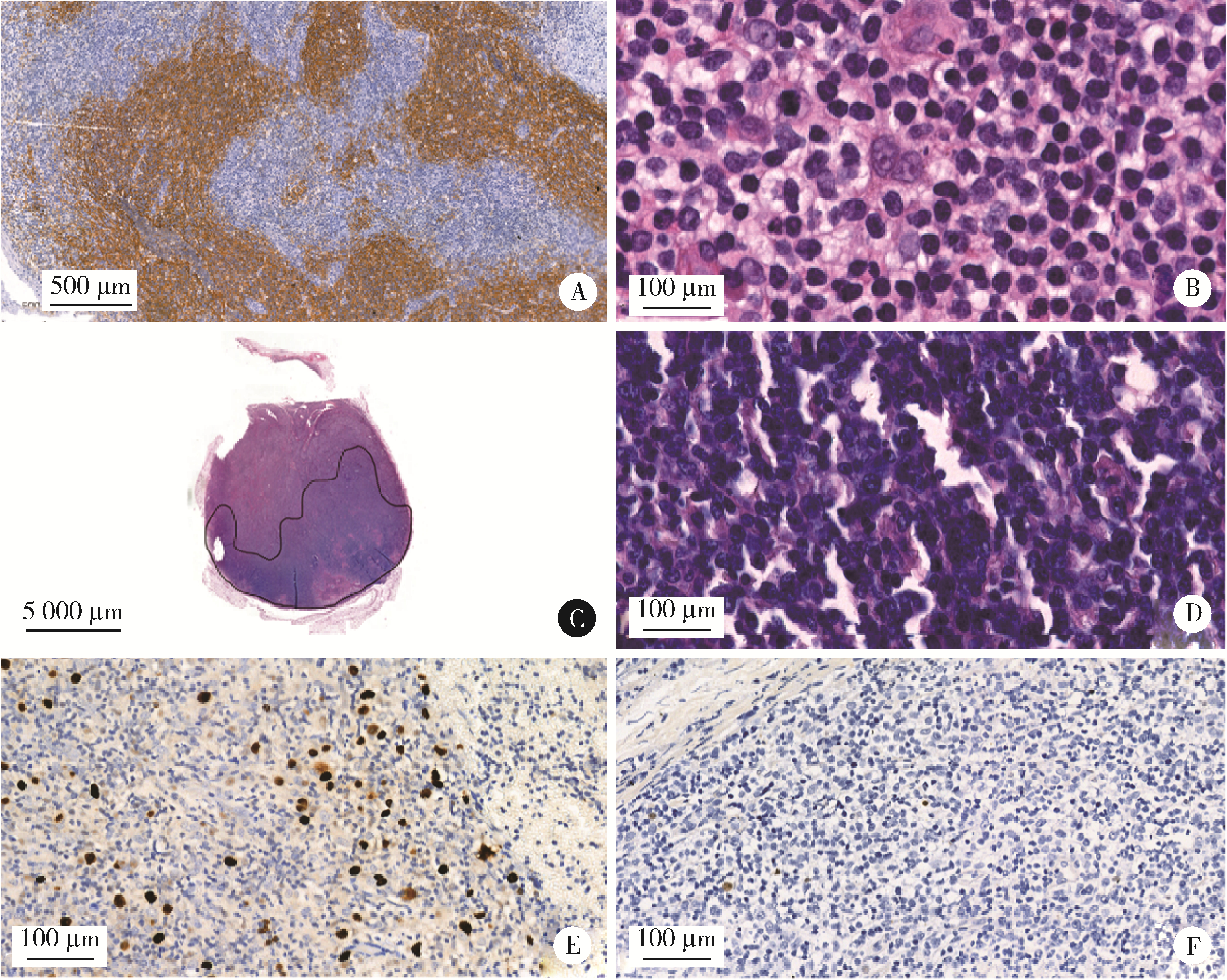
Analysis of clinicopathological and molecular abnormalities of angioimmunoblastic T-cell lymphoma
Yun-fei SHI1,Hao-jie WANG2,Wei-ping LIU3,Lan MI3,Meng-ping LONG1,Yan-fei LIU3,Yu-mei LAI1,Li-xin ZHOU1,Xin-ting DIAO1,Xiang-hong LI1,*( )
)
- 1. Department of Pathology, Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Peking University Cancer Hospital & Institute, Beijing 100142, China
2. Central Laboratory, Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Peking University Cancer Hospital & Institute, Beijing 100142, China
3. Department of Lymphoma, Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Peking University Cancer Hospital & Institute, Beijing 100142, China
CLC Number:
- R732.2





| 1 |
Swerdlow SH , Campo E , Pileri SA , et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms[J]. Blood, 2016, 127 (20): 2375- 2390.
doi: 10.1182/blood-2016-01-643569 |
| 2 |
Laurent C , Baron M , Amara N , et al. Impact of expert pathologic review of lymphoma diagnosis: Study of patients from the French lymphopath network[J]. J Clin Oncol, 2017, 35 (18): 2008- 2017.
doi: 10.1200/JCO.2016.71.2083 |
| 3 | van Krieken JHJM , Langerak AW , Macintyre EA , et al. Improved reliability of lymphoma diagnostics via PCR-based clonality testing: Report of the BIOMED-2 concerted action BHM4-CT98-3936[J]. Leukemia, 2006, 21 (2): 201- 206. |
| 4 |
Langerak AW , Groenen PJTA , Brüggemann M , et al. Euro-Clonality/BIOMED-2 guidelines for interpretation and reporting of Ig/TCR clonality testing in suspected lymphoproliferations[J]. Leukemia, 2012, 26 (10): 2159- 2171.
doi: 10.1038/leu.2012.246 |
| 5 |
Cortes JR , Palomero T . The curious origins of angioimmunoblastic T-cell lymphoma[J]. Curr Opin Hematol, 2016, 23 (4): 434- 443.
doi: 10.1097/MOH.0000000000000261 |
| 6 | 郭艳敏, 刘雪霏, 焦莉娟, 等. 血管免疫母细胞性T细胞淋巴瘤组织学分级与预后分析[J]. 中华病理学杂志, 2019, 48 (10): 784- 790. |
| 7 |
Zhang C , Mi L , Wu M , et al. Angioimmunoblastic T-cell lymphoma: Treatment strategies and prognostic factors from a retrospective multicenter study in China[J]. Leuk Lymphoma, 2022, 63 (5): 1152- 1159.
doi: 10.1080/10428194.2021.2015586 |
| 8 |
Hsu YT , Wang YC , Chen RY , et al. Angioimmunoblastic T-cell lymphoma in Taiwan reveals worse progression-free survival for RHOA G17V mutated subtype[J]. Leuk Lymphoma, 2020, 61 (5): 1108- 1118.
doi: 10.1080/10428194.2019.1702179 |
| 9 | 李婷婷, 罗璐婷, 陈溢, 等. 84例血管免疫母细胞性T细胞淋巴瘤的临床特征及预后: 单中心分析[J]. 中华血液学杂志, 2020, 41 (11): 915- 920. |
| 10 |
Steinhilber J , Mederake M , Bonzheim I , et al. The pathological features of angioimmunoblastic T-cell lymphomas with IDH2(R172) mutations[J]. Mod Pathol, 2019, 32 (8): 1123- 1134.
doi: 10.1038/s41379-019-0254-4 |
| 11 |
Hsi ED , Said J , Macon WR , et al. Diagnostic accuracy of a defined immunophenotypic and molecular genetic approach for peripheral T/NK-cell lymphomas. A North American PTCL study group project[J]. Am J Surg Pathol, 2014, 38 (6): 768- 775.
doi: 10.1097/PAS.0000000000000188 |
| 12 |
Heavican TB , Bouska A , Yu J , et al. Genetic drivers of oncogenic pathways in molecular subgroups of peripheral T-cell lymphoma[J]. Blood, 2019, 133 (15): 1664- 1676.
doi: 10.1182/blood-2018-09-872549 |
| 13 |
Schwartz FH , Cai Q , Fellmann E , et al. TET2 mutations in B cells of patients affected by angioimmunoblastic T-cell lymphoma[J]. J Pathol, 2017, 242 (2): 129- 133.
doi: 10.1002/path.4898 |
| 14 |
Palomero T , Couronne L , Khiabanian H , et al. Recurrent mutations in epigenetic regulators, RHOA and FYN kinase in peripheral T cell lymphomas[J]. Nature Genetics, 2014, 46 (2): 166.
doi: 10.1038/ng.2873 |
| 15 |
Yoo HY , Sung MK , Lee SH , et al. A recurrent inactivating mutation in RHOA GTPase in angioimmunoblastic T cell lymphoma[J]. Nat Genet, 2014, 46 (4): 371- 375.
doi: 10.1038/ng.2916 |
| 16 |
Fukumoto K , Nguyen TB , Chiba S , et al. Review of the biologic and clinical significance of genetic mutations in angioimmunoblastic T-cell lymphoma[J]. Cancer Sci, 2018, 109 (3): 490- 496.
doi: 10.1111/cas.13393 |
| 17 |
Chiba S , Sakata-Yanagimoto M . Advances in understanding of angioimmunoblastic T-cell lymphoma[J]. Leukemia, 2020, 34 (10): 2592- 2606.
doi: 10.1038/s41375-020-0990-y |
| 18 | 中国临床肿瘤学会肿瘤标志物专家委员会, 中国肿瘤驱动基因分析联盟. 二代测序技术在肿瘤精准医学诊断中的应用专家共识[J]. 中华医学杂志, 2018, 98 (26): 2057- 2065. |
| 19 | 中国抗癌协会血液肿瘤专业委员会, 中华医学会血液学分会, 中华医学会病理学分会. 二代测序技术在血液肿瘤中的应用中国专家共识(2018年版)[J]. 中华血液学杂志, 2018, 39 (11): 881- 886. |
| 20 |
Ondrejka SL , Grzywacz B , Bodo J , et al. Angioimmunoblastic T-cell lymphomas with the RHOA p.Gly17Val mutation have classic clinical and pathologic features[J]. Am J Surg Pathol, 2016, 40 (3): 335- 341.
doi: 10.1097/PAS.0000000000000555 |
| 21 | 张晨, 王小沛, 郑文, 等. 血管免疫母细胞性T细胞淋巴瘤42例临床分析[J]. 中华医学杂志, 2013, 93 (46): 3671- 3674. |
| 22 | Eladl AE , Shimada K , Suzuki Y , et al. EBV status has prognostic implication among young patients with angioimmunoblastic T-cell lymphoma[J]. Cancer Med, 2020, 9 (2): 678- 688. |
| 23 | 王芳, 张瑰红, 丁凯阳, 等. EBER、PTEN和VEGF在血管免疫母T细胞淋巴瘤中的表达及其临床病理学意义[J]. 中国实验血液学杂志, 2015, 23 (3): 663- 668. |
| 24 | Liang JH , Lu L , Zhu HY , et al. The prognostic role of circulating Epstein-Barr Virus DNA copy number in angioimmunoblastic T-cell lymphoma treated with dose-adjusted EPOCH[J]. Cancer Res Treat, 2019, 51 (1): 150- 157. |
| 25 | Kim TY , Min GJ , Jeon YW , et al. Impact of Epstein-Barr virus on peripheral T-cell lymphoma not otherwise specified and angioimmunoblastic T-cell lymphoma[J]. Front Oncol, 2021, 11, 797028. |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Doudou MA, Xiaocai MA, Tianjing CHANG, Lifang WANG, Yan DING, Lianjie SHI. Bone marrow infiltration of large B-cell lymphoma with clinical manifestations similar to systemic lupus erythematosus: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 666-669. |
| [4] | Jingyao WEI, Juxiang YE, Meiling ZHOU, Weiwei FU, Xin LIU, Kangle ZHAI, Yanyan SHI, Shigang DING, Jing ZHANG. Endoscopic characteristics of primary gastric lymphoma and prediction of treatment response [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 342-350. |
| [5] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [6] | Yirui LIAN, Jingxuan LIU, Liang ZHAO, Jing ZHAO, Sitian ZANG, Yuhui LI. Rheumatic disease spectrum and immunological profile of anti-PM/Scl antibodies in idiopathic inflammatory myopathies [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1018-1023. |
| [7] | Qi DONG, Jing HE, Yuan JIA, Haihong YAO, Xia ZHANG. VEXAS syndrome mimicking relapsing polychondritis: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1180-1183. |
| [8] | Xiaolin WANG, Luyao LI, Wen ZHANG, Hongyan WANG. Clinicopathological analysis of mesonephric-like adenocarcinoma in the corpusuteri: A report of 3 cases [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1208-1212. |
| [9] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [10] | Yuan NING, Xiaoying ZHANG, Xue LI, Yuan LI, Jing HE, Yuebo JIN. Sjögren disease complicated by primary breast lymphoma: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 808-811. |
| [11] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [12] | Guangyan YU, Xin PENG, Min GAO, Peng YE, Na GE, Mengqi JIA, Bingyu LI, Zunan TANG, Leihao HU, Wenbo ZHANG. Research progress in diagnosis and treatment of salivary gland tumors [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 1-6. |
| [13] | Jialu CHE, Zichen LIU, Kun LI, Chen ZHANG, Nanying CHE. Clinical value of automated EasyNAT system for the diagnosis of tuberculosis in paraffin-embedded tissues [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1047-1051. |
| [14] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [15] | Yinji JIN, Rui LIU. Hereditary protein S deficiency in a patient with prominent mesenteric venous thrombosis: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1106-1109. |
|
||