北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (5): 1021-1027. doi: 10.19723/j.issn.1671-167X.2022.05.032
术中超声辅助下环形减压术治疗多节段胸椎后纵韧带骨化症
翟书珩,胡攀攀,刘晓光*( )
)
- 北京大学第三医院骨科, 骨与关节精准医学工程研究中心, 脊柱疾病研究北京市重点实验室, 北京 100191
Intraoperative ultrasound assisted circumferential decompression for multilevel ossification of the posterior longitudinal ligament in thoracic vertebrae
Shu-heng ZHAI,Pan-pan HU,Xiao-guang LIU*()
- Department of Orthopaedics, Peking University Third Hospital; Engineering Research Center of Bone and Joint Precision Medicine; Beijing Key Laboratory of Spinal Disease Research, Beijing 100191, China
摘要:
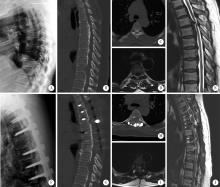
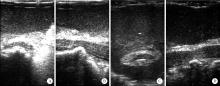
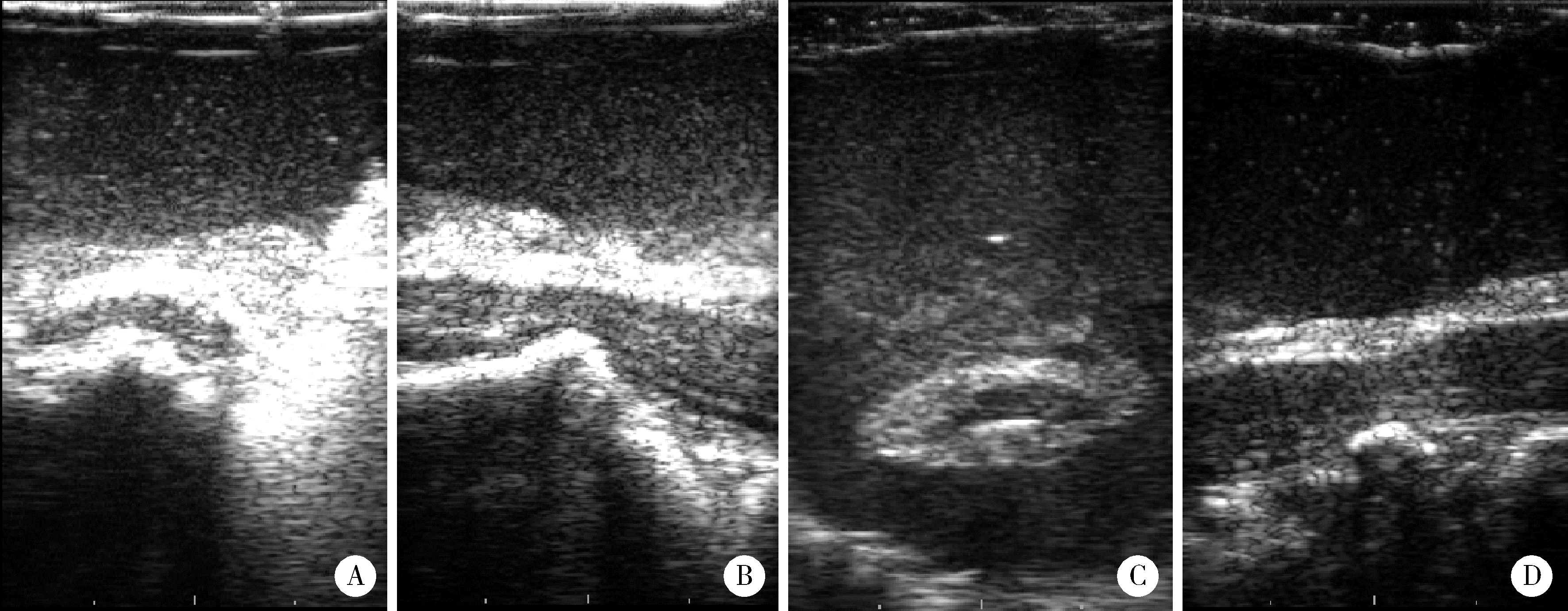
目的: 分析多节段胸椎后纵韧带骨化症(ossification of the posterior longitudinal ligament, OPLL)术中超声辅助下环形减压术的手术疗效和术后神经功能改善情况。方法: 选择2016年1月至2021年1月北京大学第三医院多节段胸椎OPLL患者的病例资料进行回顾性分析, 所有病例均完成后壁切除后行术中超声检查确定环形减压节段, 并进行环形减压。纳入研究的30例患者男性14例, 女性16例, 平均年龄(49.3±11.4)岁。首发症状以下肢麻木无力为主(83.3%), 平均症状持续时间为(33.9±42.9)个月(1~168个月)。神经功能通过术前及末次随访时改良日本骨科协会(modified Japanese Orthopedic Association, mJOA)评分(0~11分)评估, 神经功能改善率根据Harabayashi法计算。根据神经功能改善率是否大于25%将患者分为较优改善组和较差改善组, 收集两组患者的年龄、体重指数(body mass index, BMI)、病程时间、手术时间、出血量、mJOA评分、手术节段、脑脊液漏并进行分析比较。结果: 病例平均手术时间为(137.4±33.8) min(56~190 min), 平均出血量为(653.7±534.2) mL(200~3 000 mL); 术前mJOA评分为(6.0±2.1)分(2~9分), 末次随访时mJOA评分为(7.6±1.9)分(4~11分), 所有患者神经功能均较术前改善(P < 0.001)。神经功能改善率平均为(38.1±24.4)%(14.3~100.0%), 其中神经功能改善率75%~100% 4例, 50%~74% 3例, 25%~49% 14例, 0~24% 9例。较优改善组与较差改善组相比较, 术中出血量差异具有统计学意义(P=0.047)。结论: 通过术中超声辅助下胸椎环形减压术可以对长节段OPLL患者进行有效的减压, 并显著改善患者的神经功能, 控制患者术中出血量有助于术后神经功能的改善。
中图分类号:
- R61

| 1 |
Chen G , Fan T , Yang X , et al. The prevalence and clinical characteristics of thoracic spinal stenosis: A systematic review[J]. Eur Spine J, 2020, 29 (9): 2164- 2172.
doi: 10.1007/s00586-020-06520-6 |
| 2 |
Hou X , Sun C , Liu X , et al. Clinical features of thoracic spinal stenosis-associated myelopathy: A retrospective analysis of 427 cases[J]. Clin Spine Surg, 2016, 29 (2): 86- 89.
doi: 10.1097/BSD.0000000000000081 |
| 3 | Ando K, Nakashima H, Machino M, et al. Postoperative progression of ligamentum flavum ossification after posterior instrumented surgery for thoracic posterior longitudinal ligament ossification: Long-term outcomes during a minimum 10-year follow-up [J/OL]. J Neurosurg Spine, 2021(2021-12-24)[2022-06-01]. https://pubmed.ncbi.nlh.gov/34952516/. |
| 4 |
Kato S , Murakami H , Demura S , et al. Indication for anterior spinal cord decompression via a posterolateral approach for the treatment of ossification of the posterior longitudinal ligament in the thoracic spine: A prospective cohort study[J]. Eur Spine J, 2020, 29 (1): 113- 121.
doi: 10.1007/s00586-019-06047-5 |
| 5 |
刘晓光. 胸椎管狭窄症的手术技术要点[J]. 中国脊柱脊髓杂志, 2017, 27 (7): 670- 672.
doi: 10.3969/j.issn.1004-406X.2017.07.17 |
| 6 |
刘晓光, 刘忠军, 陈仲强, 等. "涵洞塌陷法"360°脊髓环形减压术治疗胸椎管狭窄症[J]. 中华骨科杂志, 2010, 30 (11): 1059- 1062.
doi: 10.3760/cma.j.issn.0253-2352.2010.11.010 |
| 7 |
Zheng C , Zhu Y , Lyu F , et al. Motor-evoked potentials in the intraoperative decision-making of circumferential decompression via posterior approach for treating thoracic posterior longitudinal ligament ossification[J]. Spine J, 2021, 21 (7): 1168- 1175.
doi: 10.1016/j.spinee.2021.01.023 |
| 8 |
Hu P , Yu M , Liu X , et al. A circumferential decompression-based surgical strategy for multilevel ossification of thoracic posterior longitudinal ligament[J]. Spine J, 2015, 15 (12): 2484- 2492.
doi: 10.1016/j.spinee.2015.08.060 |
| 9 |
Yang P , Ge R , Chen ZQ , et al. Treatment of thoracic ossification of posterior longitudinal ligament with one-stage 360 degree circumferential decompression assisted by piezosurgery[J]. J Invest Surg, 2022, 35 (2): 249- 256.
doi: 10.1080/08941939.2020.1839149 |
| 10 |
Gao A , Yu M , Wei F , et al. One-stage posterior surgery with intraoperative ultrasound assistance for thoracic myelopathy with simultaneous ossification of the posterior longitudinal ligament and ligamentum flavum at the same segment: A minimum 5-year follow-up study[J]. Spine J, 2020, 20 (9): 1430- 1437.
doi: 10.1016/j.spinee.2020.05.097 |
| 11 | Yang X, Liu X, Liu X, et al. Clinical outcomes of intraoperative contrast-enhanced ultrasound compared with intraoperative neurophysiological monitoring during circumferential decompression for myelopathy associated with thoracic-ossification of the posterior longitudinal ligament [J/OL]. Med Sci Monit, 2020, 26: e921129(2020-04-29)[2022-06-22]. http://pubmid.ncbi.nlh.gov/32345957/. |
| 12 |
Hu P , Yu M , Liu X , et al. Cerebrospinal fluid leakage after surgeries on the thoracic spine: A review of 362 cases[J]. Asian Spine J, 2016, 10 (3): 472- 479.
doi: 10.4184/asj.2016.10.3.472 |
| 13 |
Hu PP , Liu XG , Yu M . Cerebrospinal fluid leakage after thoracic decompression[J]. Chin Med J (Engl), 2016, 129 (16): 1994- 2000.
doi: 10.4103/0366-6999.187854 |
| [1] | 王军, 姚兰, 张宁, 索利斌, 李红培, 魏越, 查鹏, 梁正, 刘鲲鹏. 单侧胸椎旁阻滞对实施双腔气管插管患者血流动力学和意识水平的影响[J]. 北京大学学报(医学版), 2024, 56(5): 890-895. |
| [2] | 王永强,刘晓光,姜亮,韦峰,于淼,吴奉梁,党礌,周华,刘忠军. 胸椎管狭窄症术后脑脊液漏继发皮下积液的治疗[J]. 北京大学学报(医学版), 2018, 50(4): 657-661. |
| [3] | 许挺,李民,田杨,宋金涛,倪诚,郭向阳. 超声引导下平面内经外侧肋间入路行胸椎旁阻滞的临床评价[J]. 北京大学学报(医学版), 2017, 49(1): 148-152. |
| [4] | 张志平, 郭昭庆, 孙垂国, 曾岩, 李危石, 齐强, 陈仲强. 胸、腰椎后路内固定术后深部手术切口感染的微生物学分析[J]. 北京大学学报(医学版), 2015, 47(2): 358-360. |
| [5] | 程诚, 佟怀宇, 张远征. 胸椎髓外硬脊膜内、外炎性肌纤维母细胞瘤1例[J]. 北京大学学报(医学版), 2014, 46(2): 333-335. |
| [6] | 方礼明, 张亚军, 张军, 黄楠, 左镇华, 李兵, 王博, 林华刚. 经皮微创短节段固定治疗伴后方韧带复合体损伤的胸腰段骨折[J]. 北京大学学报(医学版), 2012, 44(6): 851-854. |
|
||
