北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (6): 1067-1073. doi: 10.19723/j.issn.1671-167X.2025.06.008
SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估
高雅静1,2,3, 李正芳1,3, 马梦思1,2,3, 武丽君1,3,*( )
)
- 1. 新疆维吾尔自治区人民医院风湿免疫科,乌鲁木齐 830000
2. 新疆医科大学,乌鲁木齐 830000
3. 新疆类风湿关节炎临床医学研究中心,乌鲁木齐 830000
Role of the SII and SIRI in risk prediction, disease activity assessment, and prog-nostic evaluation of Behçet disease uveitis
Yajing GAO1,2,3, Zhengfang LI1,3, Mengsi MA1,2,3, Lijun WU1,3,*()
- 1. Department of Rheumatology and Immunology, People's Hospital of Xinjiang Uygur Autonomous Region, Uygur 830000, China
2. Xinjiang Medical University, Uygur 830000, China
3. Xinjiang Clinical Research Center for Rheumatoid Arthritis, Uygur 830000, China
摘要:
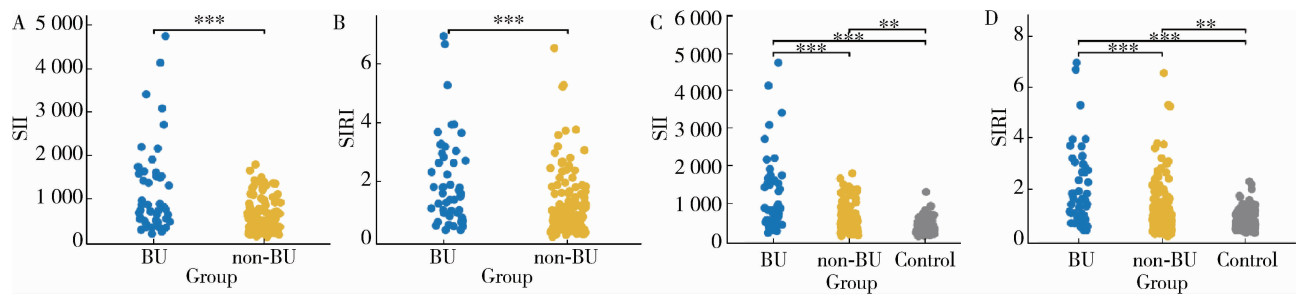
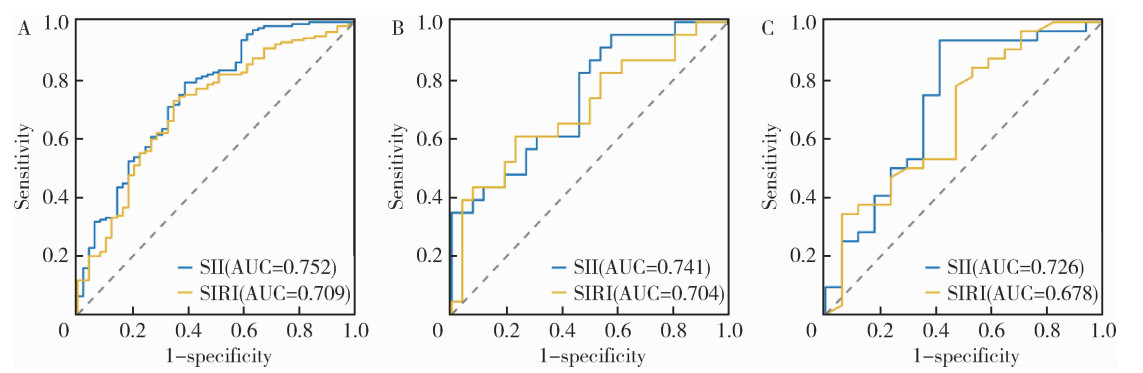
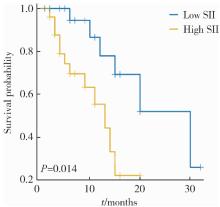
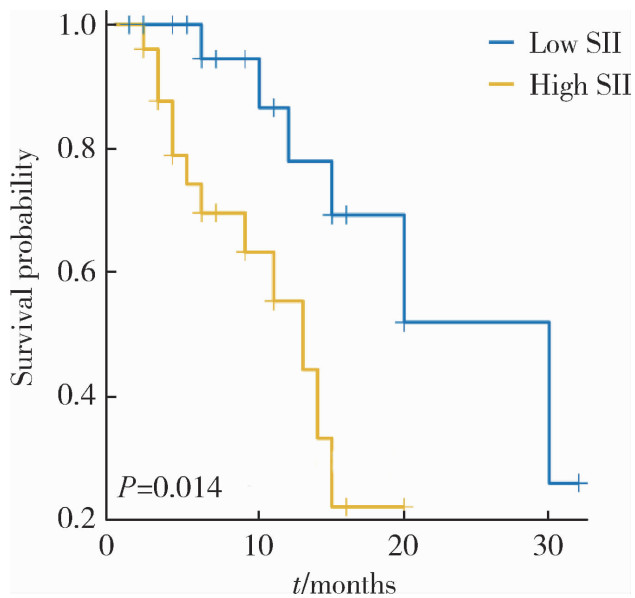
目的: 探讨全身免疫炎症指数(systemic immune inflammation index,SII)和全身炎症反应指数(systemic inflammatory response index,SIRI)与白塞病葡萄膜炎(Behçet disease uveitis, BU)的相关性,及其在BU患者疾病活动度及临床预后评估中的预测价值。方法: 回顾性纳入194例白塞病(Behçet disease, BD)患者和122例健康志愿者,按BD疾病活动与否分为疾病活动期(90例)和疾病稳定期(104例),按是否发生葡萄膜炎分为BU组(49例)与非BU组(145例),BU组按葡萄膜炎是否活动分为炎症活动期BU组(26例)与炎症稳定期BU组(23例)。基于常规血液检验指标(血小板、中性粒细胞、淋巴细胞、单核细胞计数)计算SII和SIRI。采用Spearman相关性分析评估SII和SIRI与BU发病风险、疾病活动及炎症标志物的相关性;通过受试者工作特征(receiver operating characteristic, ROC)曲线分析确定SII和SIRI预测BU发病风险及疾病活动的最佳阈值与预测效能。结果: BD疾病活动期的SII和SIRI水平均高于BD疾病稳定期(P < 0.05);有葡萄膜炎或血管受累BD患者的SII和SIRI水平高于有其他临床表现的患者(P < 0.05)。BU组患者的SII与SIRI水平均显著高于非BU组及健康对照组(P < 0.001),其中炎症活动期BU组的SII与SIRI高于炎症稳定期BU组(P=0.004)。Spearman相关性分析显示,SII与BD疾病活动(ρ=0.303,P < 0.001)呈正相关,SIRI与BD疾病活动无相关性(ρ=0.049,P=0.500);SII与BU发病风险(ρ=0.442, P < 0.001)、炎症活动(ρ=0.392, P=0.005)、炎症标志物C反应蛋白(ρ=0.272, P < 0.001)、红细胞沉降率(ρ=0.285, P < 0.001)呈正相关;SIRI仅与BU发病风险呈正相关(ρ=0.301, P=0.006)。Logistic回归分析显示,高SII是BU发病风险的独立危险因素(OR=1.003,95%CI:1.001~1.004,P<0.001)。ROC曲线分析表明,SII预测BU发病风险的阈值为711.800 [ROC曲线下的面积(area under curve, AUC)= 0.752],预测BU炎症活动的阈值为1 622.300(AUC=0.741),预测BU预后不良的阈值为1 634.200(AUC=0.726);SIRI预测BU发病风险的阈值为1.260(AUC=0.709),预测BU炎症活动的阈值为1.390(AUC=0.704),预测BU预后不良的阈值为2.790(AUC=0.678)。Kaplan-Meier曲线分析发现高SII水平是预后不良事件的独立预测因素(HR=3.440, 95%CI: 1.040~11.410, P=0.043)。结论: SII和SIRI可作为BD合并BU患者风险预测、疾病活动度及预后评估的潜在临床指标,为临床早期识别高风险BU患者及干预决策提供了依据。
中图分类号:
- R593.22

| 1 |
|
| 2 |
doi: 10.1002/art.41998 |
| 3 |
doi: 10.1007/s10067-020-05026-2 |
| 4 |
doi: 10.1016/j.preteyeres.2023.101216 |
| 5 |
doi: 10.4103/tjem.tjem_198_23 |
| 6 |
doi: 10.3389/fimmu.2025.1530534 |
| 7 |
doi: 10.3389/fnut.2024.1353964 |
| 8 |
doi: 10.1111/jdv.12107 |
| 9 |
doi: 10.1093/rheumatology/38.8.728 |
| 10 |
doi: 10.1080/25785826.2020.1800244 |
| 11 |
|
| 12 |
doi: 10.1002/advs.202411524 |
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
doi: 10.1007/s12026-021-09194-4 |
| [1] | 吴滔, 林建子, 朱亚锋, 马剑达, 贾霈雯, 杨莉娟, 潘婕, 邹耀威, 杨迎, 卢烨, 戴冽. 血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物[J]. 北京大学学报(医学版), 2025, 57(6): 1024-1031. |
| [2] | 吕雪冰, 俞烜华, 张伟桢, 刘昌泉, 林互涵, 曾珊婷, 黄惠娟, 吴月萍. 类风湿关节炎合并坏死性筋膜炎1例[J]. 北京大学学报(医学版), 2025, 57(6): 1198-1202. |
| [3] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [4] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [5] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
| [6] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [7] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [8] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [9] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
| [10] | 黄会娜,赵静,赵祥格,白自然,李霞,王冠. 乳酸对类风湿关节炎患者外周血CD4+T细胞亚群的调控作用[J]. 北京大学学报(医学版), 2024, 56(3): 519-525. |
| [11] | 汤晓菲,李永红,丁秋玲,孙卓,张阳,王育梅,田美伊,刘坚. 类风湿关节炎患者下肢深静脉血栓发病率及危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 279-283. |
| [12] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
| [13] | 金银姬,孙琳,赵金霞,刘湘源. 血清IgA型抗鼠科肉瘤病毒癌基因同源物B1抗体在类风湿关节炎中的意义[J]. 北京大学学报(医学版), 2023, 55(4): 631-635. |
| [14] | 蔡文心,李仕成,刘一鸣,梁如玉,李静,郭建萍,胡凡磊,孙晓麟,李春,刘栩,叶华,邓立宗,李茹,栗占国. 类风湿关节炎临床分层及其特征的横断面研究[J]. 北京大学学报(医学版), 2022, 54(6): 1068-1073. |
| [15] | 程昉,杨邵英,房星星,王璇,赵福涛. CCL28-CCR10通路在类风湿关节炎单核细胞迁移中的作用[J]. 北京大学学报(医学版), 2022, 54(6): 1074-1078. |
|
||
