北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 670-673. doi: 10.19723/j.issn.1671-167X.2026.03.030
胸锁关节痛风1例
甘地1, 付强1, 唐小惠1, 李楚炜1, 舒兆平2,*( )
)
- 1. 南华大学附属第一医院风湿免疫科,湖南衡阳 421001
2. 南华大学附属第一医院医院感染管理科,湖南衡阳 421001
Gout of the manubriosternal joints: A case report
Di GAN1, Qiang FU1, Xiaohui TANG1, Chuwei LI1, Zhaoping SHU2,*()
- 1. Department of Rheumatology and Immunology, The First Affiliated Hospital, Hengyang Medical School, University of South China, Hengyang 421001, Hunan, China
2. Department of Healthcare-associated Infection Management, The First Affiliated Hospital, Hengyang Medical School, University of South China, Hengyang 421001, Hunan, China
摘要:
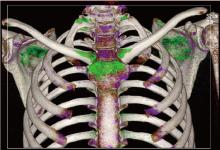
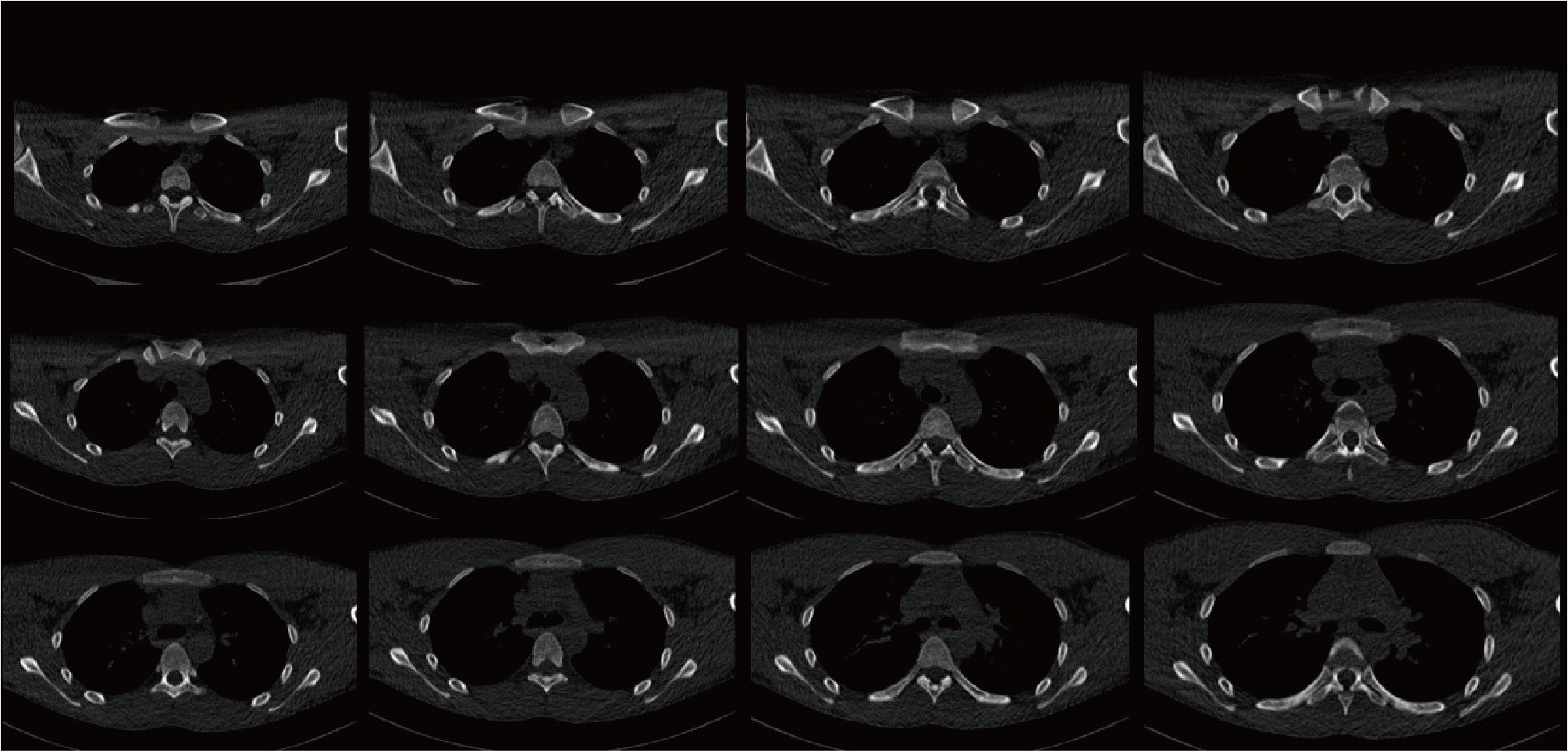
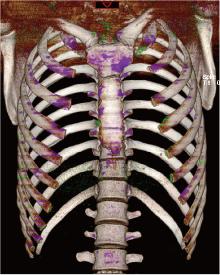
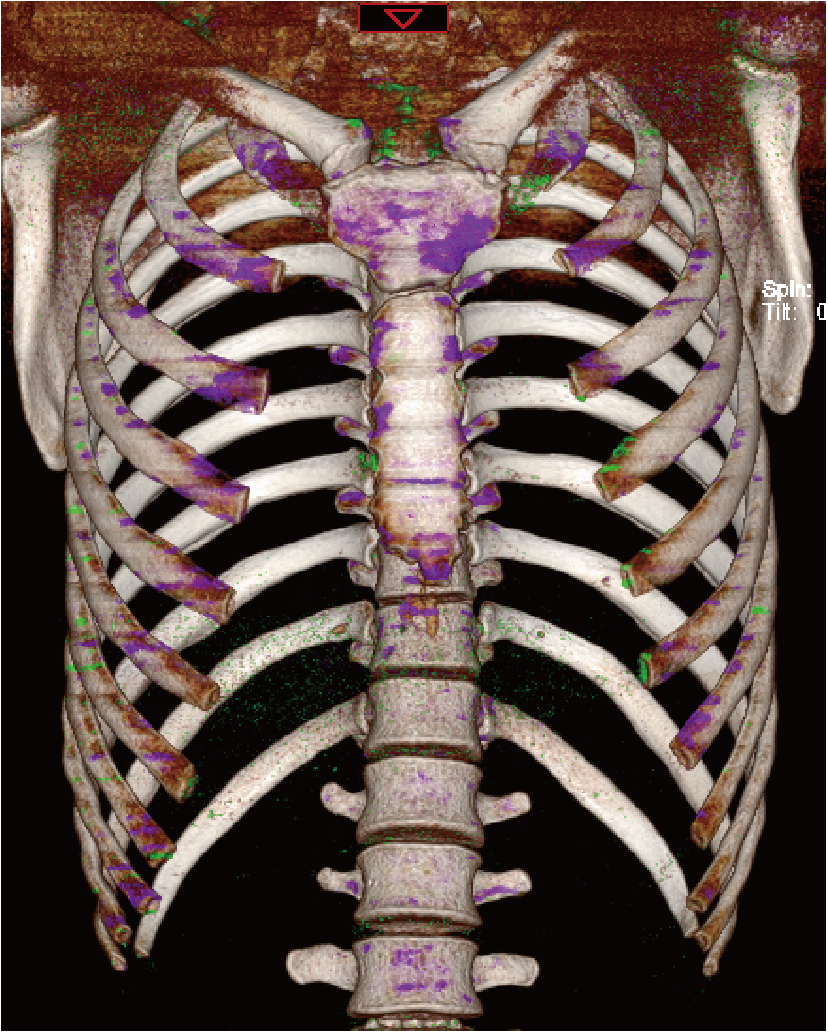
痛风是嘌呤代谢异常和/或尿酸排泄障碍所致的代谢性疾病,以单钠尿酸盐结晶沉积于关节或软组织引发的复发性急性关节炎为特征,根据病因可分为原发性和继发性。多数病例与尿酸排泄障碍相关,其自然病程包括无症状期、急性关节炎期与间歇期、痛风石及慢性关节炎期。急性痛风性关节炎常表现为突发性关节剧痛,伴受累关节及周围软组织红肿、发热、压痛,大关节受累时可出现关节积液,发作常于夜间或清晨,具有自限性,多在两周内自行缓解。急性痛风发作最常见的部位是第一跖趾关节,其次为中足、踝、膝、腕、指和肘关节,极少累及中轴关节。疼痛常伴有活动受限,严重影响患者的日常生活与生活质量。若累及罕见部位或血尿酸正常时易致误诊,因此需结合病史、查体、实验室及影像学检查综合判断。本例为19岁男性,因反复前胸痛入院,外院曾疑诊强直性脊柱炎。查体可见双侧胸锁关节压痛、红肿,皮温增高伴活动受限。骶髂关节MRI无异常,血清尿酸正常。胸部双能量CT显示胸骨、双侧锁骨、肩胛骨、多根肋骨及胸骨边缘多处痛风石。依据患者病史、体征及影像学检查确诊为痛风,给予降尿酸、镇痛及饮食调整治疗。随访两年,患者胸痛未再发作,多次血尿酸检查均低于300 μmol/L,复查双能量CT显示胸锁关节等处的痛风石明显减少。
中图分类号:
- R589.7

| 1 |
doi: 10.1016/S0140-6736(21)00569-9 |
| 2 |
doi: 10.1136/annrheumdis-2015-208237 |
| 3 |
doi: 10.1136/annrheumdis-2019-215315 |
| 4 |
doi: 10.3899/jrheum.080938 |
| 5 |
doi: 10.1093/rheumatology/keaa923 |
| 6 |
doi: 10.1148/radiol.2015142631 |
| 7 |
|
| 8 |
doi: 10.1093/rheumatology/keab301 |
| 9 |
doi: 10.1164/rccm.201301-0097IM |
| 10 |
doi: 10.31486/toj.20.0143 |
| 11 |
doi: 10.4103/2156-7514.103058 |
| 12 |
doi: 10.1016/j.clinre.2011.09.003 |
| 13 |
|
| 14 |
doi: 10.1111/j.1524-4741.2011.01129.x |
| 15 |
中华医学会内分泌学分会. 中国高尿酸血症与痛风诊疗指南(2019)[J]. 中华内分泌代谢杂志, 2020, 36 (1): 1- 13.
|
| 16 |
doi: 10.1001/jama.2011.1169 |
| [1] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [2] | 董泓,王丽敏,王志强,刘彦卿,张晓刚,张明明,刘娟,李振彬. 急性痛风发作的昼夜差异: 一项男性痛风患者的临床研究[J]. 北京大学学报(医学版), 2023, 55(5): 915-922. |
| [3] | 叶一林,刘恒,潘利平,柴卫兵. 全膝关节置换术后假体周围痛风发作误诊1例[J]. 北京大学学报(医学版), 2023, 55(2): 362-365. |
| [4] | 王昱,张慧敏,邓雪蓉,刘伟伟,陈璐,赵宁,张晓慧,宋志博,耿研,季兰岚,王玉,张卓莉. 尿枸橼酸定量检测在原发性痛风患者肾结石诊断中的应用价值[J]. 北京大学学报(医学版), 2022, 54(6): 1134-1140. |
| [5] | 谢晓炜,李芬,凌光辉,谢希,许素清,陈谊月. 痛风患者健康教育知识知晓度测量问卷的研制及临床应用[J]. 北京大学学报(医学版), 2022, 54(4): 699-704. |
| [6] | 彭喆,丁亚敏,裴林,姚海红,张学武,唐素玫. 痛风患者发生关节及肌腱内晶体沉积的临床特点[J]. 北京大学学报(医学版), 2021, 53(6): 1067-1071. |
| [7] | 张学武. 痛风关节炎治疗中几个备受关注的问题[J]. 北京大学学报(医学版), 2021, 53(6): 1017-1019. |
| [8] | 王贵红,左婷,李然,左正才. 瑞巴派特在大鼠痛风性关节炎急性发作中的作用[J]. 北京大学学报(医学版), 2021, 53(4): 716-720. |
| [9] | 谢一帆,王昱,邓雪蓉,耿研,季兰岚,张卓莉. 影响双能CT尿酸盐结晶检出率的因素[J]. 北京大学学报(医学版), 2021, 53(2): 261-265. |
| [10] | 王昱,邓雪蓉,季兰岚,张晓慧,耿研,张卓莉. 超声检测痛风患者肌腱受累的危险因素和诊断价值[J]. 北京大学学报(医学版), 2021, 53(1): 143-149. |
| [11] | 季兰岚,郝燕捷,张卓莉. 原发性骨髓纤维化引起的继发性痛风1例[J]. 北京大学学报(医学版), 2018, 50(6): 1117-1119. |
| [12] | 张倩茹,王昱,张卓莉. 2015 ACR/EULAR痛风分类标准与既往标准诊断价值的比较研究[J]. 北京大学学报(医学版), 2017, 49(6): 979-984. |
| [13] | 赵卫, 高辉, 朱佳鑫, 张学武, 栗占国. 血清Dickkopf-1与原发性痛风性关节炎骨破坏的相关性[J]. 北京大学学报(医学版), 2012, 44(2): 254-258. |
| [14] | 武丽君, 宋小芸, 库尔班江, 石亚妹, 黄慈波, 黄嘉, 刘爱华, 米克拉依, 滕玉芬, 古丽娜, 孟新艳, 单新洁, 木亚赛, 苑爱萍, 张莉. 新疆吐鲁番地区维吾尔族人群高尿酸血症和痛风的流行病学调查[J]. 北京大学学报(医学版), 2012, 44(2): 250-253. |
| [15] | 刘湘源, 郑晓娟. 尿酸持续达标是难治性痛风治疗的关键[J]. 北京大学学报(医学版), 2012, 44(2): 168-170. |
|
||
