北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (3): 510-518. doi: 10.19723/j.issn.1671-167X.2019.03.020
腹膜透析患者营养不良-炎症-心血管疾病与认知功能恶化的关系
段丽萍1,郑朝霞1,张宇慧2,董捷2△( )
)
- 1. 邯郸市中心医院肾内一科,河北邯郸 056001
2. 北京大学第一医院肾内科,北京大学肾脏病研究所,卫生部重点实验室,教育部慢性肾脏病防治重点实验室,北京 100034
Association of malnutrition-inflammation-cardiovascular disease with cognitive deterioration in peritoneal dialysis patients
Li-ping DUAN1,Zhao-xia ZHENG1,Yu-hui ZHANG2,Jie DONG2△()
- 1. Handan Central Hospital, Department 1 of Nephrology, Handan 056001, Hebei, China
2. Renal Division, Department of Medicine; Institute of Nephrology, Peking University First Hospital; Key Laboratory of Renal Disease, Ministry of Health of China; Key Laboratory of Chronic Kidney Disease Prevention and Treatment, Ministry of Education, Beijing 100034, China
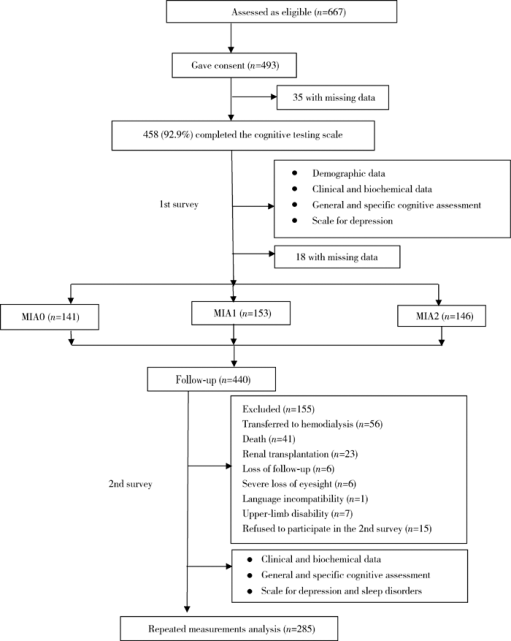
摘要: 目的 探讨腹膜透析(peritoneal dialysis, PD)患者存在的营养不良-炎症状态-心血管疾病(动脉硬化)(malnutrition-inflammation-atherosclerosis,MIA)综合征与认知功能恶化的关系。方法 采用前瞻性纵向队列研究,于2013年3—11月,对符合入选标准的腹膜透析患者完成总体和特定认知功能测定,结合基线是否有心血管疾病病史,白蛋白≤35 g/L,超敏C-反应蛋白(high-sensitive C-reactive protein, hs-CRP)≥3 mg/L,将患者分为MIA0(全为否)、MIA1(1项为是)、MIA2(≥2项为是)3个组,并于随访2年后对患者重复认知功能测定。采用卡方检验、单因素方差分析、Kruskal-Wallis H 检验比较基线及2年后组间一般资料、生化指标,以及总体和特定认知功能参数。进一步的组间多重两两比较采用Bonferroni方法调整显著性值。以每一项总体和特异认知功能得分差值为因变量,以年龄、性别、教育水平、体重指数、抑郁分数、糖尿病、血钠和MIA(MIA0为对照,MIA1和MIA2为哑变量)为自变量,以多元线性回归分析影响认知功能恶化的因素,每一项认知领域的分析都以其相应的基线参数进行校正。结果 随访2年后,认知障碍(cognitive impairment, CI)的发生率从20.0%上升到24.7%。MIA2和MIA1组修正的简易智力状态检查量表(the modified mini-mental state examination, 3MS)得分下降绝对值明显高于MIA0组(-3.9±12.0 vs. 1.1±6.7, P<0.01;-2.3±11.8 vs. 1.1±6.7, P<0.05),而特定认知功能测定包括执行功能(连线试验A和B,P=0.401,P=0.176)、即时记忆(P=0.437)、延迟记忆(P=0.104)、视觉空间能力(P=0.496)和语言能力(P=0.171)的变化3组间差异无统计学意义。经多元线性回归分析,年龄、教育水平、糖尿病、抑郁等均是一项或多项认知功能恶化的危险因素,存在MIA综合征一项因素是整体认知恶化的独立危险因素(P=0.022),存在MIA综合征两项及以上因素者不仅是整体认知恶化的独立危险因素(P<0.001),而且是延迟记忆、视觉功能及语言功能恶化的独立危险因素(P=0.002,P=0.007,P=0.004)。结论 腹膜透析患者存在MIA综合征一项及以上因素是总体认知功能恶化的高危人群;存在MIA综合征因素越多,患者的特异认知功能领域影响越广泛。
中图分类号:
- R459.5

| [1] |
Griva K, Stygall J, Hankins M , et al. Cognitive impairment and 7-year mortality in dialysis patients[J]. Am J Kidney Dis, 2010,56(4):693-703.
doi: 10.1053/j.ajkd.2010.07.003 |
| [2] |
Shea YF, Lam MF, Lee MS , et al. Prevalence of cognitive impairement among peritoneal dialysis patients, impact on peritonitis and role of assisted dialysis[J]. Perit Dial Int, 2016,36(3):284-290.
doi: 10.3747/pdi.2014.00247 |
| [3] |
Kalirao P, Pederson S, Foley RN , et al. Cognitive impairment in peritoneal dialysis patients[J]. Am J Kidney Dis, 2011,57(4):612-620.
doi: 10.1053/j.ajkd.2010.11.026 |
| [4] |
Kurella M, Chertow GM, Luan J , et al. Cognitive impairment in chronic kidney disease[J]. J Am Geriatr Soc, 2004,52(11):1863-1869.
doi: 10.1111/jgs.2004.52.issue-11 |
| [5] |
Dong J, Pi HC , Xiong ZY, et a1. Depression and cognitive impairment in peritoneal dialysis: A multi-center cross-sectional study[J]. Am J Kidney Dis, 2016,67(1):111-118.
doi: 10.1053/j.ajkd.2015.06.025 |
| [6] |
Zhang YH, Yang ZK, Wang JW , et al. Cognitive changes in peritoneal dialysis patients: a multi-center prospective cohort study[J]. Am J Kidney Dis, 2018,72(5):691-700.
doi: 10.1053/j.ajkd.2018.04.020 |
| [7] |
Kurella M, Mapes DL , Port FK, et a1. Correlates and outcomes of dementia among dialysis patients: the dialysis outcomes and practice patterns study[J]. Nephrol Dial Transplant, 2006,21(9):2543-2548.
doi: 10.1093/ndt/gfl275 |
| [8] |
Weiner DE, Scott TM , Giang LM, et a1. Cardiovascular disease and cognitive function in maintenance hemodialysis patients[J]. Am J Kidney Dis, 2011,58(5):773-781.
doi: 10.1053/j.ajkd.2011.03.034 |
| [9] |
Roberts RO, Geda YE , Knopman DS, et a1. Association of C-reactive protein with mild cognitive impairment[J]. Alzheimers Dement, 2009,5(5):398-405.
doi: 10.1016/j.jalz.2009.01.025 |
| [10] |
Radi c ' J , Ljutic D , Radi c ' M , et al. Cognitive-psychomotor functions and nutritional status in maintenance hemodialysis patients: are they related[J]. Ther Apher Dial, 2011,15(6):532-539.
doi: 10.1111/tap.2011.15.issue-6 |
| [11] |
Tamura MK, Yaffe K . Dementia and cognitive impairment in ESRD: diagnostic and therapeutic strategies[J]. Kidney Int, 2011,79(1):14-22.
doi: 10.1038/ki.2010.336 |
| [12] |
Etgen T, Chonchol M, Förstl H , et al. Chronic kidney disease and cognitive impairment: a systematic review and meta-analysis[J]. Am J Nephrol, 2012,35(5):474-482.
doi: 10.1159/000338135 |
| [13] | 段丽萍, 郑朝霞, 吕宁 , 等. 腹膜透析患者营养不良-炎症-心血管疾病和认知功能的关系[J]. 中国血液净化, 2016,15(11):600-604. |
| [14] |
Smith SC, Jackson R, Pearson TA , et al. Principles for national and regional guidelines on cardiovascular disease prevention: a scientific statement from the World Heart and Stroke Forum[J]. Circulation, 2004,109(25):3112-3121.
doi: 10.1161/01.CIR.0000133427.35111.67 |
| [15] | Teng EL, Chui HC . The modified mini-mental state (3MS) examination[J]. J Clin Psychiatry, 1987,48(8):314-318. |
| [16] |
Kurella M, Chertow GM, Fried LF , et al. Chronic kidney disease and cognitive impairment in the elderly: the health, aging, and body composition study[J]. J Am Soc Nephrol, 2005,16(7):2127-2133.
doi: 10.1681/ASN.2005010005 |
| [17] |
Lin FR, Yaffe K, Xia J , et al. Hearing loss and cognitive decline in older adults[J]. JAMA Intern Med, 2013,173(4):293-299.
doi: 10.1001/jamainternmed.2013.1868 |
| [18] | Randolph C . Repeatable battery for the assessment of neuropsychological status (RBANS)[Z]. San Antonio, TX: The Psychological Corporation, 1998. |
| [19] | Cheng Y, Wu W, Wang J , et al. Reliability and validity of the repeatable battery for the assessment of neuropsychological status in community-dwelling elderly[J]. Arch Med Sci, 2011,7(5):850-857. |
| [20] | 张保华, 谭云龙, 张五芳 , 等. 重复性成套神经心理状态测验的信度、效度分析[J]. 中国心理卫生杂志, 2008,22(12):865-869. |
| [21] | 杨贵刚, 田菊, 谭云龙 , 等. 重复性成套神经心理状态测验在北京地区正常人群中的应用[J]. 中国心理卫生杂志, 2010,24(12):926. |
| [22] |
Zung WW . A self-rating depression scale[J]. Arch Gen Psychiatry, 1965,12:63-70.
doi: 10.1001/archpsyc.1965.01720310065008 |
| [23] |
Papagianni A, Kalovoulos M, Kirmizis D , et al. Carotid atherosclerosis is associated with inflammation and endothelial cell adhesion molecules in chronic haemodialysis patients[J]. Nephrol Dial Transplant, 2003,18(1):113-119.
doi: 10.1093/ndt/18.1.113 |
| [24] | Bartens W, Nauck M, Schollmeyer P , et al. Elevated lipoprotein(a)and fibrinogen levels [corrected] increase the cardiovascular risk in continuous ambulatory peritoneal dialysis patients[J]. Perit Dial Int, 1996,16(1):27-33. |
| [25] |
Irish A . Cardiovascular disease, fibrinogen and theacute phase response: associations with lipids and blood pressure in patients with chronic renal disease[J]. Atherosclerosis, 1998,137(1):133-139.
doi: 10.1016/S0021-9150(97)00273-6 |
| [26] | Pi HC, Xu YF, Xu R , et al. Cognitive impairment and structural neuroimaging abnormalities among patients with chronic kidney disease [J]. Kidney Blood Press Res, 2016,41(6):986-996. |
| [1] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [2] | 刘爱春, 赵慧萍, 武蓓, 郑姝颖, 左力, 王梅. 腹膜透析相关性腹膜炎拔管患者导管内细菌生物膜的形成[J]. 北京大学学报(医学版), 2025, 57(1): 161-165. |
| [3] | 谢芳菲, 乔虹, 李博雅, 袁翠, 王芳, 孙瑜, 李双玲. 妊娠期重度营养不良合并急性肾盂肾炎致脓毒症、难治性感染性休克、多器官功能衰竭1例[J]. 北京大学学报(医学版), 2025, 57(1): 202-207. |
| [4] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [5] | 侯婉音,董捷. 腹膜透析患者获得性肾囊肿出血3例[J]. 北京大学学报(医学版), 2024, 56(3): 546-550. |
| [6] | 陈楚云,孙蓬飞,赵静,贾佳,范芳芳,王春燕,李建平,姜一梦,霍勇,张岩. 北京社区人群促红细胞生成素相关因素及其与10年心血管疾病风险的关系[J]. 北京大学学报(医学版), 2023, 55(6): 1068-1073. |
| [7] | 鲍雷,蔡夏夏,张明远,任磊磊. 维生素D3对2型糖尿病小鼠轻度认知障碍的改善作用及机制研究[J]. 北京大学学报(医学版), 2023, 55(4): 587-592. |
| [8] | 闫晓晋,刘云飞,马宁,党佳佳,张京舒,钟盼亮,胡佩瑾,宋逸,马军. 《中国儿童发展纲要(2011-2020年)》实施期间中小学生营养不良率变化及其政策效应分析[J]. 北京大学学报(医学版), 2023, 55(4): 593-599. |
| [9] | 乔婕,芦丽霞,何玉婷,门春翠,楚新新,武蓓,赵慧萍,王梅. 真菌性腹膜透析导管出口感染合并隧道感染1例[J]. 北京大学学报(医学版), 2023, 55(4): 748-754. |
| [10] | 张紫薇,花语蒙,刘爱萍. 中国中老年人群抑郁症状、缺血性心血管疾病10年风险对心血管疾病的联合影响[J]. 北京大学学报(医学版), 2023, 55(3): 465-470. |
| [11] | 张云静,乔丽颖,祁萌,严颖,亢伟伟,刘国臻,王明远,席云峰,王胜锋. 乳腺癌患者新发心血管疾病预测模型的建立与验证:基于内蒙古区域医疗数据[J]. 北京大学学报(医学版), 2023, 55(3): 471-479. |
| [12] | 张明露,刘秋萍,巩超,王佳敏,周恬静,刘晓非,沈鹏,林鸿波,唐迅,高培. 阿司匹林用于心血管病一级预防的不同策略比较:一项马尔可夫模型研究[J]. 北京大学学报(医学版), 2023, 55(3): 480-487. |
| [13] | 董尔丹. 心血管受体的信号转导与疾病[J]. 北京大学学报(医学版), 2022, 54(5): 796-802. |
| [14] | 郭子宁, 梁志生, 周仪, 张娜, 黄捷. 基于国际疾病分类的心血管疾病亚型的基因组学研究[J]. 北京大学学报(医学版), 2021, 53(3): 453-459. |
| [15] | 刘秋萍,陈汐瑾,王佳敏,刘晓非,司亚琴,梁靖媛,沈鹏,林鸿波,唐迅,高培. 基于马尔可夫模型的社区人群心血管病筛查策略的效果评价[J]. 北京大学学报(医学版), 2021, 53(3): 460-466. |
|
||
