北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (3): 571-578. doi: 10.19723/j.issn.1671-167X.2019.03.029
数字化下颌运动记录及咀嚼肌肌电图在下颌骨肿瘤患者口颌功能评价中的应用
王晶,陈俊鹏,王洋,许向亮,郭传瑸△( )
)
- 北京大学口腔医学院·口腔医院,口腔颌面外科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
Application of digital mandibular movement record and masticatory muscle electromyography in the evaluation of stomatognathic function in patients with mandibular tumor
Jing WANG,Jun-peng CHEN,Yang WANG,Xiang-liang XU,Chuan-bin GUO△()
- Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
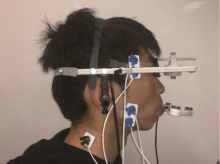
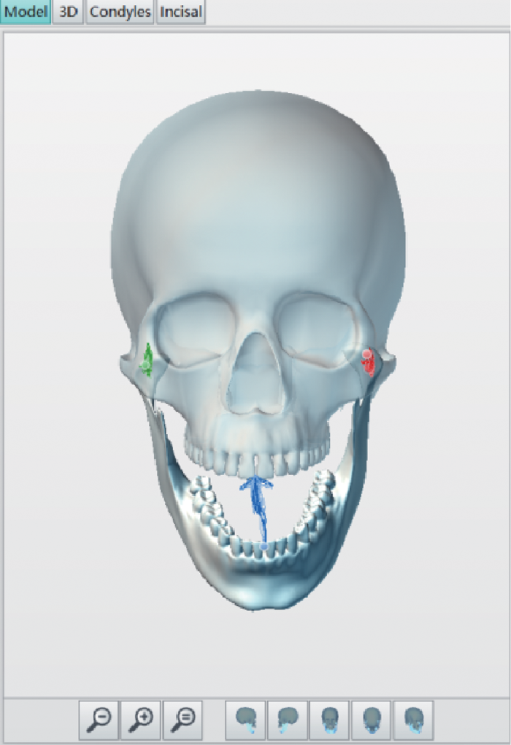
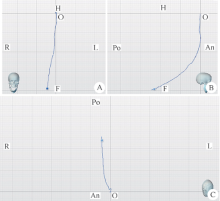
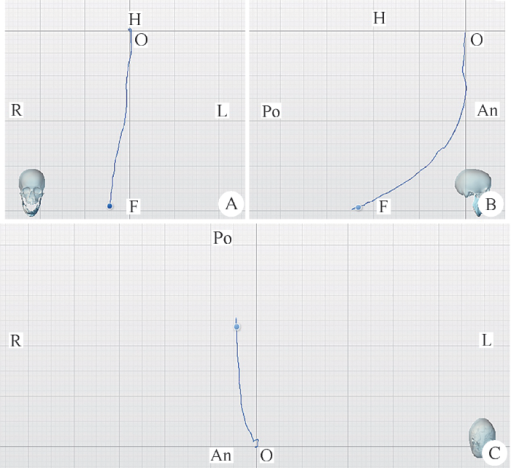
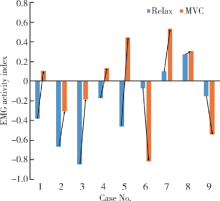
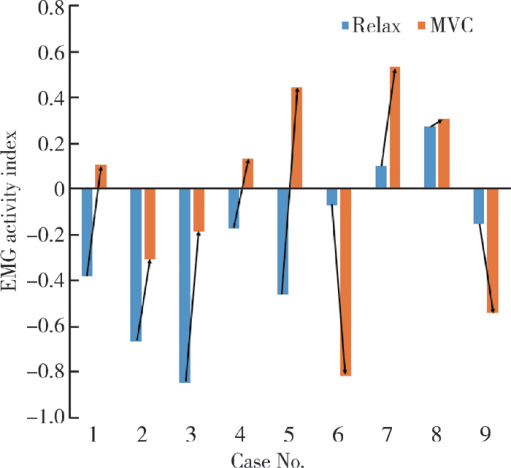
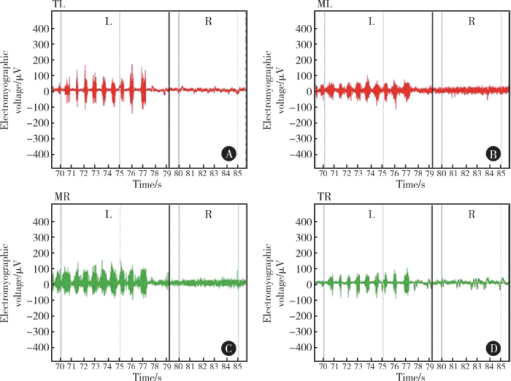
摘要: 目的 将数字化下颌运动记录与肌电图相结合,观察单侧下颌骨体部及升支肿瘤患者术前、术后下颌运动和咀嚼肌功能临床特点,初步探索运动和咀嚼肌功能的相互关系和产生机制。方法 纳入单侧下颌骨体部及升支病变术前患者6例以及下颌骨单侧病变节段性切除及颌骨重建术后患者3例。采用下颌运动记录系统及表面肌电图系统,采集患者下颌边缘运动、咀嚼运动的运动轨迹,同时记录双侧咬肌、颞肌表面肌电图,采集患者静息、最大力咬合时双侧咬肌、颞肌表面肌电图。在数字化虚拟模型上观测运动轨迹,并分析下颌边缘运动的幅度和方向。分析患者健、患侧静息,最大力咬合,双侧咀嚼时的咀嚼肌电活动特点,计算不对称指数、活动指数。结果 术前患者最大开口度均值为(35.20±6.87) mm,3例患者轻度张口受限,所有患者张口轨迹均偏向患侧。侧向运动中患侧运动平均幅度(10.34±1.27) mm,健侧(6.94±2.41) mm,差异有统计学意义。术后患者最大开口度均值为(30.65±17.32) mm,下颌边缘运动特点与术前患者一致。术前患者最大力咬合时,患侧咬肌肌电活动[44.20 (5.70, 197.90) μV]和颞肌的肌电活动中位数[42.15 (22.90, 155.00) μV]略低于健侧咬肌[45.60 (7.50, 235.40) μV]和健侧颞肌[63.30 (44.10, 126.70) μV],咀嚼时未见异常。术后则出现了个性化的改变,部分患者患侧肌电活动减弱,部分患者患侧肌电活动亢进。结论 良、恶性肿瘤及手术均可造成下颌运动和双侧咬肌和颞肌的肌电活动异常。
中图分类号:
- R782.13



| [1] | 袁道英, 杨佑成, 宋冰 . 下颌骨髁状突骨软骨瘤一例报告[J]. 中华肿瘤防治杂志, 2007,14(22):1759-1760. |
| [2] |
Krause I, Eisenstein B, Davidovits M , et al. Maxillomandibular brown tumor: a rare complication of chronic renal failure[J]. Pediatr Nephrol, 2000,14(6):499-501.
doi: 10.1007/s004670050803 |
| [3] |
Park SR, chung SM, Lim JY , et al. Giant cell tumor of the mandible[J]. Clin Exp Otorhinolaryngol, 2012,5(1):49-52.
doi: 10.3342/ceo.2012.5.1.49 |
| [4] | 徐保华, 史宗道 . 下颌髁突原发肿瘤:附12例报告[J]. 实用口腔医学杂志, 2001,17(3):249-250. |
| [5] |
Marunick MT, Mathog RH . Mastication in patients treated for head and neck cancer: a pilot study.[J]. J Prosthet Dent, 1990,63(5):566-573.
doi: 10.1016/0022-3913(90)90078-Q |
| [6] |
Hidalgo DA . Fibula free flap: a new method of mandible reconstruction[J]. Plast Reconstr Surg, 1989,84(1):71-79.
doi: 10.1097/00006534-198907000-00014 |
| [7] | Urken ML, Buchbinder D, Weinberg H , et al. Functional evaluation following microvascular oromandibular reconstruction of the oral cancer patient: a comparative study of reconstructed and nonreconstructed patients[J]. Laryngoscope, 1991,101(9):935-950. |
| [8] |
Lee R, Slevin N, Musgrove B , et al. Prediction of post-treatment trismus in head and neck cancer patients[J]. Br J Oral Maxillofac Surg, 2012,50(4):328-332.
doi: 10.1016/j.bjoms.2011.06.009 |
| [9] |
Kreeft AM, Krap M, Wismeijer D , et al. Oral function after maxillectomy and reconstruction with an obturator[J]. Int J Oral Max Surg, 2012,41(11):1387-1392.
doi: 10.1016/j.ijom.2012.07.014 |
| [10] |
Akashi M, Shibuya Y, Takahashi S , et al. Four-dimensional computed tomography evaluation of jaw movement following mandibular reconstruction: a pilot study[J]. J Cranio Maxill Surg, 2016,44(5):637-641.
doi: 10.1016/j.jcms.2016.01.027 |
| [11] | Haraguchi M, Mukohyama H, Reisberg DJ , et al. Electromyographic activity of masticatory muscles and mandibular movemet during function in marginal mandibulectomy patients[J]. J Med Dent Sci, 2003,50(4):257-264. |
| [12] |
Yen CI, Chou PY, Chen CH , et al. Kinematic, kinetic and surface electromyography analysis following zygomatic fracture reconstruction[J]. J Med Biol Eng, 2017,37(4):468-473.
doi: 10.1007/s40846-017-0271-z |
| [13] |
Ishida S, Shibuya Y, Kobayashi M , et al. Assessing stomatognathic performance after mandibulectomy according to the method of mandibular reconstruction[J]. Int J Oral Max Surg, 2015,44(8):948-955.
doi: 10.1016/j.ijom.2015.03.011 |
| [14] | 樊英显, 孙宏晨, 徐勇忠 . 颞下颔关节紊乱综合征患者咀嚼肌肌电分析[J]. 口腔医学研究, 1994(3):149-150. |
| [15] | Campillo B, Martín C, Palma JC , et al. Electromyographic activity of the jaw muscles and mandibular kinematics in young adults with theoretically ideal dental occlusion: reference values[J]. Med Oral Patol Oral Cir Bucal, 2017,22(3):e383-e391. |
| [16] | 黄超, 许向亮, 孙玉春 , 等. 下颌髁突功能面三维运动轨迹的初步推算和模拟[J]. 中华口腔医学杂志, 2018,53(10):669-673. |
| [1] | 单珅瑶, 杨咏涛, 李文博, 温奥楠, 高梓翔, 商相宜, 王勇, 赵一姣. 基于下颌运动轨迹的𬌗架关键参数计算方法[J]. 北京大学学报(医学版), 2026, 58(1): 115-125. |
| [2] | 余霄腾, 黄奕瑄, 李新飞, 陈昶甫, 赵方舟, 应鸿刚, 陶子豪, 张一鸣, 徐丽清, 李志华, 杨昆霖, 周利群, 李学松, 赵峥. 结石相关输尿管狭窄的上尿路修复手术技术与临床结局[J]. 北京大学学报(医学版), 2025, 57(4): 670-675. |
| [3] | 田素青, 孙海涛, 赵田地, 王巍. 6D治疗床辅助影像引导下放射治疗头颈部肿瘤摆位误差分析[J]. 北京大学学报(医学版), 2024, 56(6): 1097-1100. |
| [4] | 徐心雨,吴灵,宋凤岐,李自力,张益,刘筱菁. 基于下颌运动轨迹的正颌外科术中下颌骨髁突定位方法及初步精度验证[J]. 北京大学学报(医学版), 2024, 56(1): 57-65. |
| [5] | 刘梅歌,方朴,王严,丛璐,范洋溢,袁远,徐燕,张俊,洪道俊. 远端型遗传性运动神经病8例的临床、病理及遗传学特点[J]. 北京大学学报(医学版), 2021, 53(5): 957-963. |
| [6] | 房硕博,杨广聚,康艳凤,孙玉春,谢秋菲. 数字化辅助确定再定位牙合垫颌位方法的探索和精度评价[J]. 北京大学学报(医学版), 2021, 53(1): 76-82. |
| [7] | 刘小璇,张朔,刘娜,孙阿萍,张英爽,樊东升. 震颤分析用于早期帕金森病的诊断价值[J]. 北京大学学报(医学版), 2019, 51(6): 1096-1102. |
| [8] | 闫树东,杨广聚,莫思怡,刘云,谢秋菲. 大鼠后肢长期抗阻训练对慢性咬肌机械痛觉敏感性的影响[J]. 北京大学学报(医学版), 2019, 51(1): 21-27. |
| [9] | 李健男,冯芝恩,王琳,王衣祥,郭传瑸. 乏氧诱导因子-1α在口腔鳞状细胞癌颈淋巴转移中的作用[J]. 北京大学学报(医学版), 2018, 50(1): 26-32. |
| [10] | 于尧, 章文博, 王洋, 刘筱菁, 郭传瑸, 俞光岩, 彭歆. iPlan CMF软件辅助下增强CT三维重建在头颈部肿瘤治疗中的应用[J]. 北京大学学报(医学版), 2017, 49(5): 878-882. |
| [11] | 王威,郑磊,刘树铭,黄明伟,石妍,吕晓鸣,张杰,张建国. 单纯放射性粒子治疗后的头颈部腺源性癌远处转移[J]. 北京大学学报(医学版), 2017, 49(3): 547-550. |
| [12] | 刘存瑞, 徐啸翔, 曹烨, 谢秋菲. 咬合干扰时间因素对大鼠咀嚼肌机械痛觉敏感的影响[J]. 北京大学学报(医学版), 2016, 48(1): 51-56. |
| [13] | 张杰, 郑磊, 刘树铭, 黄明伟, 高岩, 张祖燕, 张建国. 空心针穿刺活检在口腔颌面部肿瘤的应用[J]. 北京大学学报(医学版), 2012, 44(5): 801-803. |
| [14] | 江萍, 马月, 王俊杰, 冉维强, 姜玉良, 曲昂. 超声引导放射性125I粒子植入治疗头颈部复发肿瘤[J]. 北京大学学报(医学版), 2012, 44(2): 291-294. |
| [15] | 马长城, 王振宇, 于涛. C1-2哑铃型肿瘤的手术治疗[J]. 北京大学学报(医学版), 2011, 43(2): 301-303. |
|
||
