北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (4): 673-677. doi: 10.19723/j.issn.1671-167X.2019.04.013
MRI对肾细胞癌静脉瘤栓侵犯下腔静脉壁的术前评估
吴静云1,米悦2,刘水1,姚林2,唐琦2,何志嵩2,王霄英1,△( )
)
- 1. 北京大学第一医院医学影像科,北京 100034
2. 北京大学第一医院泌尿外科,北京 100034
Evaluating inferior vena cava wall invasion in renal cell carcinoma tumor thrombus with MRI
Jing-yun WU1,Yue MI2,Shui LIU1,Lin YAO2,Qi TANG2,Zhi-song HE2,Xiao-ying WANG1,△()
- 1.Department of Radiology, Peking University First Hospital, Beijing 100034, China
2.Department of Urology, Peking University First Hospital, Beijing 100034, China
摘要:
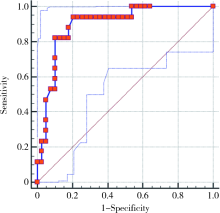
目的:评价MRI对肾细胞癌下腔静脉瘤栓侵犯下腔静脉壁的诊断价值。方法:回顾性分析2010—2018年在北京大学第一医院行肾根治性切除术及下腔静脉取栓术的肾细胞癌患者,术前行1.5 T或3.0 T MRI检查的56例患者被纳入本研究。由两位影像科医生测量术前MRI图像瘤栓所在水平肾静脉及下腔静脉最大径、下腔静脉瘤栓的长度,并评判瘤栓是否充满下腔静脉腔达两侧缘、瘤栓边缘是否光滑、瘤栓与下腔静脉壁分界是否清晰、下腔静脉壁正常信号是否改变等征象。基于病理证实下腔静脉壁受累与否将患者分为两组,对临床资料及MRI征象进行单因素分析及多因素回归分析。结果:56例患者中男性43例、女性13例,平均年龄(55.64±0.43)岁,有17例(30.4%)病理证实下腔静脉壁受累, 大部分为透明细胞癌。下腔静脉壁受累组与非受累组比较,下腔静脉瘤栓的长度更长[(7.91±3.59) cm vs. (5.94±3.57) cm,P=0.049]、瘤栓充满下腔静脉腔(P=0.002)、瘤栓边缘不光滑(P=0.005)、瘤栓与下腔静脉壁分界不清晰(P=0.001)、下腔静脉壁正常信号改变(P<0.001)出现的概率更大,结合这五个指标诊断下腔静脉壁受累的敏感性及特异性为94.12%和79.49%。结论:MRI可作为评估下腔静脉瘤栓侵犯静脉壁的方法,结合下腔静脉瘤栓的长度及MRI征象可以获得较高的诊断敏感性及特异性。
中图分类号:
- R737.11

| [1] | Motzer RJ, Jonasch E, Agarwal N , et al. Kidney cancer, version 2.2017: NCCN Clinical Practice Guidelines in oncology[J]. J Natl Compr Canc Netw, 2017,15(6):804-834. |
| [2] | Ljungberg B, Bensalah K, Canfield S , et al. EAU guidelines on renal cell carcinoma: 2014 update[J]. Eur Urol, 2015,67(5):913-924. |
| [3] | Hatcher PA, Anderson EE, Paulson DF , et al. Surgical management and prognosis of renal cell carcinoma invading the vena cava[J]. J Urol, 1991,145(1):20-23. |
| [4] | Lawindy SM, Kurian T, Kim T , et al. Important surgical consi-derations in the management of renal cell carcinoma (RCC) with inferior vena cava (IVC) tumour thrombus[J]. BJU Int, 2012,110(7):926-939. |
| [5] | Guo HF, Song Y, Na YQ , et al. Value of abdominal ultrasound scan, CT and MRI for diagnosing inferior vena cava tumour thrombus in renal cell carcinoma[J]. Chin Med J (Engl), 2009,122(19):2299-2302. |
| [6] | Neves RJ, Zincke H . Surgical treatment of renal cancer with vena cava extension[J]. Br J Urol, 1987,59(5):390-395. |
| [7] | Ciancio G, Livingstone AS, Soloway M . Surgical management of renal cell carcinoma with tumor thrombus in the renal and inferior vena cava: the University of Miami experience in using liver transplantation techniques[J]. Eur Urol, 2007,51(4):988-994. |
| [8] | Kwon TW, Kim H, Moon KM , et al. Surgical treatment of inferior vena cava tumor thrombus in patients with renal cell carcinoma[J]. J Korean Med Sci, 2010,25(1):104-109. |
| [9] | Hatakeyama S, Yoneyama T, Hamano I , et al. Prognostic benefit of surgical management in renal cell carcinoma patients with thrombus extending to the renal vein and inferior vena cava: 17-year experience at a single center[J]. BMC Urol, 2013(13):47. |
| [10] | Chen X, Li S, Xu Z , et al. Clinical and oncological outcomes in Chinese patients with renal cell carcinoma and venous tumor thrombus extension: single-center experience[J]. World J Surg Oncol, 2015(13):14. |
| [11] | Whitson JM, Reese AC, Meng MV . Population based analysis of survival in patients with renal cell carcinoma and venous tumor thrombus[J]. Urol Oncol, 2013,31(2):259-263. |
| [12] | 中华医学会泌尿外科学分化中国肾癌联盟, 中国肾癌伴下腔静脉癌栓诊疗写作组. 肾癌伴静脉癌栓诊治专家共识[J]. 中华泌尿外科杂志, 2018,39(12):881-884. |
| [13] | Psutka SP, Boorjian SA, Thompson RH , et al. Clinical and radiographic predictors of the need for inferior vena cava resection du-ring nephrectomy for patients with renal cell carcinoma and caval tumour thrombus[J]. BJU Int, 2015,116(3):388-396. |
| [14] | Hallscheidt PJ, Fink C, Haferkamp A , et al. Preoperative staging of renal cell carcinoma with inferior vena cava thrombus using multidetector CT and MRI: prospective study with histopathological correlation[J]. J Comput Assist Tomogr, 2005,29(1):64-68. |
| [15] | Gupta NP, Ansari MS, Khaitan A , et al. Impact of imaging and thrombus level in management of renal cell carcinoma extending to veins[J]. Urol Int, 2004,72(2):129-134. |
| [16] | Cuevas C, Raske M, Bush WH , et al. Imaging primary and se-condary tumor thrombus of the inferior vena cava: multi-detector computed tomography and magnetic resonance imaging[J]. Curr Probl Diagn Radiol, 2006,35(3):90-101. |
| [17] | Lawrentschuk N, Gani J, Riordan R , et al. Multidetector computed tomography vs magnetic resonance imaging for defining the upper limit of tumour thrombus in renal cell carcinoma: a study and review[J]. BJU Int, 2005,96(3):291-295. |
| [18] | Adams LC, Ralla B, Bender YY , et al. Renal cell carcinoma with venous extension: prediction of inferior vena cava wall invasion by MRI[J]. Cancer imaging, 2018,18(1):17. |
| [19] | Aslam Sohaib SA, Teh J , et al. Assessment of tumor invasion of the vena caval wall in renal cell carcinoma cases by magnetic resonance imaging[J]. J Urol, 2002,167(3):1271-1275. |
| [20] | Oto A, Herts BR, Remer EM , et al. Inferior vena cava tumor thrombus in renal cell carcinoma: staging by MR imaging and impact on surgical treatment[J]. AJR Am J Roentgenol, 1998,171(6):1619-1624. |
| [21] | Laissy JP, Menegazzo D, Debray MP , et al. Renal carcinoma: diagnosis of venous invasion with Gd-enhanced MR venography[J]. Eur Radiol, 2000,10(7):1138-1143. |
| [22] | Alayed A, Krishna Sk, Breau RH , et al. Diagnostic accuracy of MRI for detecting inferior vena cava wall invasion in renal cell carcinoma tumor thrombus using quantitative and subjective analysis[J]. AJR Am J Roentgenol, 2019,212(3):562-569. |
| [23] | Myneni L, Hricak H, Carroll PR . Magnetic resonance imaging of renal carcinoma with extension into the vena cava: staging accuracy and recent advances[J]. Br J Urol, 1991,68(6):571-578. |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 杨静, 许晓韵, 郑丹妮, 凌晓彤, 屈留洋, 柳登高. 544例慢性唾液腺炎的临床与影像学特点及病因分析[J]. 北京大学学报(医学版), 2026, 58(3): 650-657. |
| [4] | 步召德, 冯梦宇, 季科. 早期胃癌行前哨淋巴结导航手术的实践与思考[J]. 北京大学学报(医学版), 2026, 58(2): 239-243. |
| [5] | 王海, 江一舟. 靶向血管治疗在乳腺癌精准治疗中的分子机制与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 251-256. |
| [6] | 罗必显, 刘洪铭, 谢伟勋, 龚渭华. 产甲胎蛋白胃癌的新临床特征和前沿科学问题[J]. 北京大学学报(医学版), 2026, 58(2): 257-265. |
| [7] | 付浩, 申潞艳, 黄冰洋, 马少华. 免疫治疗背景下食管鳞状细胞癌围手术期治疗的临床思考[J]. 北京大学学报(医学版), 2026, 58(2): 266-271. |
| [8] | 王昕莹, 程雪原, 张孟钧, 李菲, 段晋瑜, 乔静. 浓缩生长因子联合引导性组织再生术治疗下颌磨牙根分叉病变的疗效[J]. 北京大学学报(医学版), 2026, 58(2): 372-379. |
| [9] | 殷昊明, 王子杰, 舒帆, 张展奕, 梁会, 张树栋. 肾透明细胞癌FABP6基因长转录本的表达及意义[J]. 北京大学学报(医学版), 2026, 58(2): 393-398. |
| [10] | 李嘉临, 陈力侨, 唐家天, 吴艳, 王安强. 胃肝样腺癌转化治疗1例[J]. 北京大学学报(医学版), 2026, 58(2): 399-404. |
| [11] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [12] | 潘子晨, 陈凯, 侯钰坤, 杨博涵, 张继新, 马永蔌, 田孝东, 杨尹默. 胰腺腺鳞癌临床病理特征与分子机制研究进展[J]. 北京大学学报(医学版), 2026, 58(2): 431-435. |
| [13] | 单珅瑶, 杨咏涛, 李文博, 温奥楠, 高梓翔, 商相宜, 王勇, 赵一姣. 基于下颌运动轨迹的𬌗架关键参数计算方法[J]. 北京大学学报(医学版), 2026, 58(1): 115-125. |
| [14] | 杨雨婷, 屈留洋, 郑丹妮, 凌晓彤, 许晓韵, 柳登高. 1 812例唾液腺结石患者的人口学特征和临床特点[J]. 北京大学学报(医学版), 2026, 58(1): 153-159. |
| [15] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
|
||
