北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (4): 769-774. doi: 10.19723/j.issn.1671-167X.2019.04.031
圆锥马尾部黏液乳头型室管膜瘤继发中枢神经系统表面铁沉积症1例报道及文献复习
许力1,胡明洁2,李玉玉1,屈洪党1,钱伟东1,刘晓林1,△( )
)
- 1. 蚌埠医学院第一附属医院神经内科, 安徽蚌埠 233004
2. 蚌埠医学院生命科学学院, 安徽蚌埠 233020
Superficial siderosis of the central nervous system caused by myxopapillary ependymoma of conus medullaris and cauda equine: a case report and literature review
Li XU1,Ming-jie HU2,Yu-yu LI1,Hong-dang QU1,Wei-dong QIAN1,Xiao-lin LIU1,△()
- 1. Department of Neurology, The First Affiliated Hospital of Bengbu Medical College, Bengbu 233004, Anhui, China
2. School of Life Sciences, Bengbu Medical College, Bengbu 233020, Anhui, China
摘要:
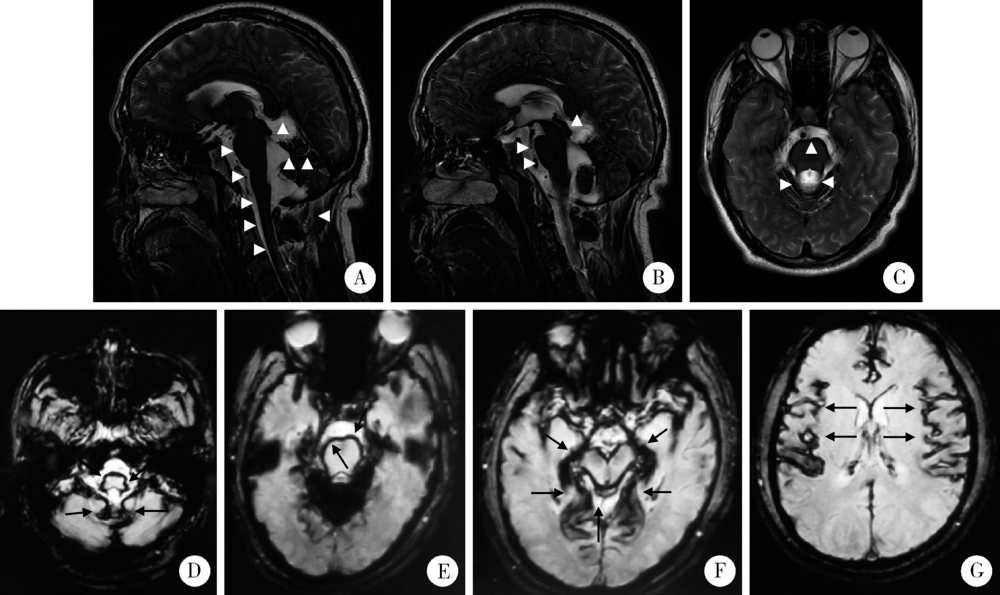
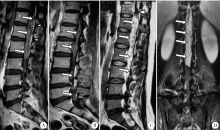
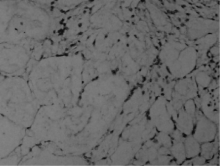
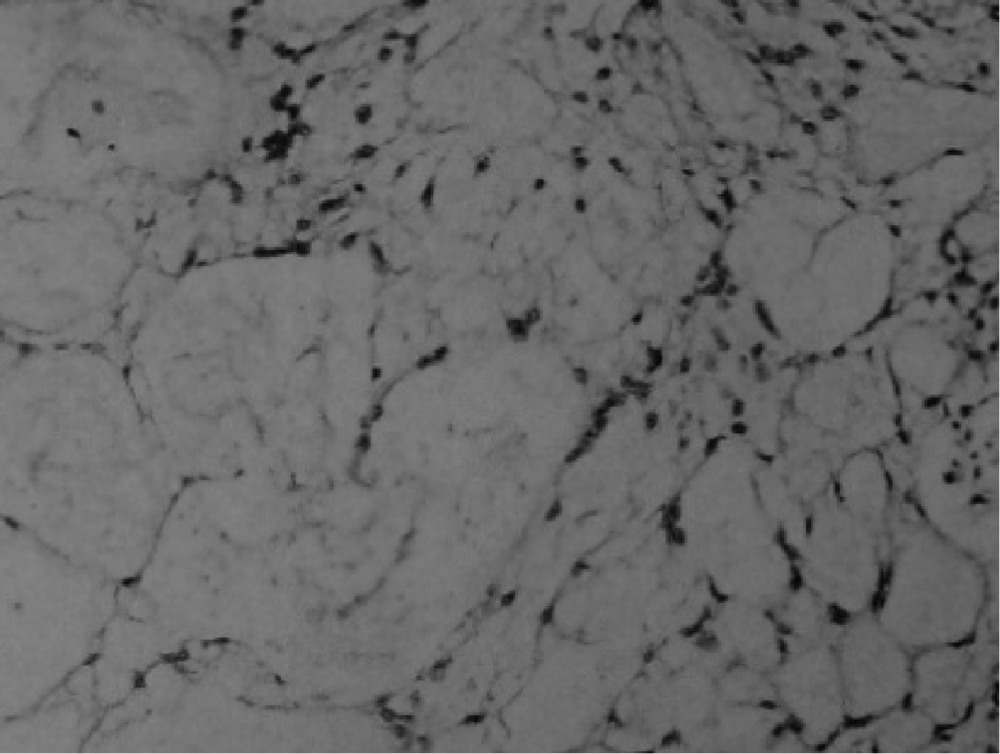
中枢神经系统表面铁沉积症(superficial siderosis of the central nervous system, SSCNS)是由于慢性反复性出血进入脑脊液而导致过多的铁沉积在脑干、小脑、脊髓乃至部分脑神经表面所致的神经系统损害,较为罕见,肿瘤是出血源之一。目前国内在其诊治方面存在以下不足:认识较晚,诊断病例较少,长期随访资料匮乏,病因诊断不够重视,漏诊率较高,治疗水平较国外存在较大差距。SSCNS典型临床表现为:双侧进行性神经性耳聋、小脑共济失调和锥体束征阳性,称为SSCNS三联征,但同时具备三联征的患者较少,给及时诊断带来一定困难。MRI对确诊该病有重要意义,铁沉积在小脑、脑干、脊髓等表面呈特征性线状低信号,SE-T2WI呈细线条,GE-T2WI及磁敏感加权成像序列(susceptibility weighted imaging,SWI)呈显著粗线条。唯一有效的治疗方法是确定出血源并清除,MRI检查同样有助于寻找出血源,因此,如果考虑SSCNS,必须进行脑、脊柱MRI检查以寻找病因。本文报道1例37岁男性SSCNS患者,临床主要表现为共济失调、神经性耳聋和嗅觉减退,MRI表现有典型的中枢神经系统表面T2加权低信号,病因追查发现脊髓下端及马尾、终丝部巨大占位病变,经手术切除并组织病理学检查提示黏液乳头型室管膜瘤(myxopapillary ependymoma,MPE)。结合文献复习探讨了MPE继发SSCNS的机制,并对SSCNS的病因、临床表现、诊断以及治疗进行综述,以提高临床医师对该病的认识及诊断水平,尤其强调对该病病因的查找有利于治疗方案的准确制定。
中图分类号:
- R739.4

| [1] | Wang K, Xu Z, Xiong G , et al. Superficial siderosis of the central nervous system manifested with seizures[J]. J Clin Neurosci, 2010,17(2):277-278. |
| [2] | Levy M, Turtzo C, Llinas RH . Superficial siderosis: a case report and review of the literature[J]. Nat Clin Pract Neurol, 2007,3(1):54-58. |
| [3] | Sydlowski SA, Cevette MJ, Shallop J . Superficial siderosis of the central nervous system: phenotype and implications for audiology and otology[J]. Otol Neurotol, 2011,32(6):900-908. |
| [4] | Savoiardo M, Grisoli M . Further in-depth look at superficial side-rosis (and intracranial hypotension)[J]. AJNR Am J Neurora-diol, 2010,31(8):E72-E73. |
| [5] | Rodriguez FR, Srinivasan A . Superficial siderosis of the CNS[J]. AJR Am J Roentgenol, 2011,197(1):W149-W152. |
| [6] | Wang J, Gong X . Superficial siderosis of the central nervous system: MR findings with susceptibility-weighted imaging[J]. Clin Imaging, 2011,35(3):217-221. |
| [7] | Kumar N . Neuroimaging in superficial siderosis: an in-depth look[J]. AJNR Am J Neuroradiol, 2010,31(1):5-14. |
| [8] | Khalatbari K . Case 141: superficial siderosis[J]. Radiology, 2009,250(1):292-297. |
| [9] | Koeppen AH, Michael SC, Li D , et al. The pathology of superficial siderosis of the central nervous system[J]. Acta Neuropathol, 2008,116(4):371-382. |
| [10] | Tosaka M, Sato K, Amanuma M , et al. Superficial siderosis of the central nervous system caused by hemorrhagic intraventricular craniopharyngioma: case report and literature review[J]. Neurol Med Chir (Tokyo), 2015,55(1):89-94. |
| [11] | Friedman DP, Hollander MD . Neuroradiology case of the day. Myxopapillary ependymoma of the conus medullaris or filum terminale resulting in superficial siderosis and dissemination of tumor along CSF pathways[J]. Radiographics, 1998,18(3):794-798. |
| [12] | Lemmerling M, De Praeter G, Mollet P , et al. Secondary superficial siderosis of the central nervous system in a patient presenting with sensorineural hearing loss[J]. Neuroradiology, 1998,40(5):312-314. |
| [13] | Messori A, Di Bella P, Herber N , et al. The importance of suspecting superficial siderosis of the central nervous system in clinical practice[J]. J Neurol Neurosurg Psychiatry, 2004,75(2):188-190. |
| [14] | Spengos K, Vassilopoulou S, Tsivgoulis G , et al. Superficial siderosis due to a lumbar ependymoma mimicking adult-onset spinocerebellar ataxia[J]. Clin Neurol Neurosurg, 2007,109(8):705-707. |
| [15] | Grech R, Galvin L, Looby S , et al. Spinal ependymoma complicated by superficial siderosis [J]. BMJ Case Rep, 2013: pii: bcr2013201036. doi: 10.1136/bcr-2013-201036. |
| [16] | Pikis S, Cohen JE, Vargas AA , et al. Superficial siderosis of the central nervous system secondary to spinal ependymoma[J]. J Clin Neurosci, 2014,21(11):2017-2019. |
| [17] | Ulrich CT, Beck J, Seifert V , et al. Ependymoma of conus medullaris presenting as subarachnoid haemorrhage[J]. Acta Neurochir (Wien), 2008,150(2):185-188 |
| [18] | Argyropoulou PI, Argyropoulou MI, Tsampoulas C , et al. Myxopapillary ependymoma of the conus medullaris with subarachnoid haemorrhage: MRI in two cases[J]. Neuroradiology, 2001,43(6):489-491. |
| [19] | Busche K . Neurologic disorders associated with weight lifting and body building[J]. Neurol Clin, 2008,26(1):309-324. |
| [20] | Khalatbari MR, Moharamzad Y . Myxopapillary ependymoma of the conus medullaris presenting with intratumoral hemorrhage during weight lifting in a teenager Childs[J]. Nerv Syst, 2014,30(1):181-183. |
| [21] | Boncoraglio GB, Ballabio E, Erbetta A , et al. Superficial siderosis due to dural defect with thoracic spinal cord herniation[J]. J Neurol Sci, 2012,312(1-2):170-172. |
| [22] | Levy M, Llinas RH . Update on a patient with superficial siderosis on deferiprone[J]. AJNR Am J Neuroradiol, 2012,33(6):E99-E100. |
| [1] | 王泽远, 于栓宝, 郑浩轲, 陶金, 范雅峰, 张雪培. 基于临床特征和多参数MRI的前列腺癌盆腔淋巴结转移的术前预测模型[J]. 北京大学学报(医学版), 2025, 57(4): 684-691. |
| [2] | 孙建军, 马千权, 尹晓亮, 杨辰龙, 张嘉, 陈素华, 吴超, 谢京城, 韩芸峰, 林国中, 司雨, 杨军, 邬海博, 赵强. 任意维度重建磁共振对骶管囊肿进行精准分型对于指导微创手术和康复的意义[J]. 北京大学学报(医学版), 2025, 57(2): 303-308. |
| [3] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [4] | 田宇轩,阮明健,刘毅,李德润,吴静云,沈棋,范宇,金杰. 双参数MRI改良PI-RADS评分4分和5分病灶的最大径对临床有意义前列腺癌的预测效果[J]. 北京大学学报(医学版), 2024, 56(4): 567-574. |
| [5] | 刘毅,袁昌巍,吴静云,沈棋,肖江喜,赵峥,王霄英,李学松,何志嵩,周利群. 靶向穿刺+6针系统穿刺对PI-RADS 5分患者的前列腺癌诊断效能[J]. 北京大学学报(医学版), 2023, 55(5): 812-817. |
| [6] | 袁昌巍,李德润,李志华,刘毅,山刚志,李学松,周利群. 多参数磁共振成像中动态对比增强状态在诊断PI-RADS 4分前列腺癌中的应用[J]. 北京大学学报(医学版), 2023, 55(5): 838-842. |
| [7] | 刘颖,霍然,徐慧敏,王筝,王涛,袁慧书. 磁共振血管壁成像评估颈动脉中重度狭窄患者斑块特征与脑血流灌注的相关性[J]. 北京大学学报(医学版), 2023, 55(4): 646-651. |
| [8] | 傅强,高冠英,徐雁,林卓华,孙由静,崔立刚. 无症状髋关节前上盂唇撕裂超声与磁共振检查的对比研究[J]. 北京大学学报(医学版), 2023, 55(4): 665-669. |
| [9] | 叶珊,金萍萍,张楠,邬海博,石林,赵强,杨坤,袁慧书,樊东升. 肌萎缩侧索硬化患者认知功能改变与脑皮层厚度分析[J]. 北京大学学报(医学版), 2022, 54(6): 1158-1162. |
| [10] | 蔡颖,万巧琴,蔡宪杰,高亚娟,韩鸿宾. 光生物调节加速脑组织间液引流及其机制[J]. 北京大学学报(医学版), 2022, 54(5): 1000-1005. |
| [11] | 王书磊,高阳旭,张宏武,杨海波,李辉,李宇,沈笠雪,姚红新. 儿童基底节区生殖细胞瘤30例临床分析[J]. 北京大学学报(医学版), 2022, 54(2): 222-226. |
| [12] | 张帆,陈曲,郝一昌,颜野,刘承,黄毅,马潞林. 术前及术后膜性尿道长度与腹腔镜根治性前列腺切除术后控尿功能恢复的相关性[J]. 北京大学学报(医学版), 2022, 54(2): 299-303. |
| [13] | 吴一凡,张晓圆,任爽,玉应香,常翠青. 基于磁共振的青年男性股四头肌的测量和评估[J]. 北京大学学报(医学版), 2021, 53(5): 843-849. |
| [14] | 盛荟,梁磊,周童亮,贾彦兴,王彤,袁兰,韩鸿宾. 光磁双模态探针钆-[4,7-双-羧甲基-10-(2-荧光素硫脲乙基)-1,4,7,10-四氮杂环十二烷-1-基]-乙酸络合物合成方法的改进[J]. 北京大学学报(医学版), 2020, 52(5): 959-963. |
| [15] | 赵世明,杨铁军,许春苗,郭孝峰,马永康,陈学军,李祥,何朝宏. 3.0T磁共振成像在接受过经尿道膀胱肿瘤切除术膀胱癌中诊断肌层浸润的应用[J]. 北京大学学报(医学版), 2020, 52(4): 701-704. |
|
||
