北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (1): 193-195. doi: 10.19723/j.issn.1671-167X.2020.01.031
• 疑难/罕见病例分析 • 上一篇
表现为耳后区巨大肿物的口外型舌下腺囊肿1例
杨洁1,2,张然3,刘宇楠1,王佃灿1,△( )
)
- 1. 北京大学口腔医学院·口腔医院,口腔颌面外科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
2. 山西医科大学口腔医学院·口腔医院,太原 030001
3. 北京大学口腔医学院·口腔医院病理科,北京 100081
Plunging ranula presenting as a giant retroauricular mass: A case report
Jie YANG1,2,Ran ZHANG3,Yu-nan LIU1,Dian-can WANG1,△()
- 1. Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
2. Shanxi Medical University School and Hospital of Stomatology, Taiyuan 030001, China
3. Department of Oral Pathology, Peking University School and Hospital of Stomatology, Beijing 100081, China
摘要:
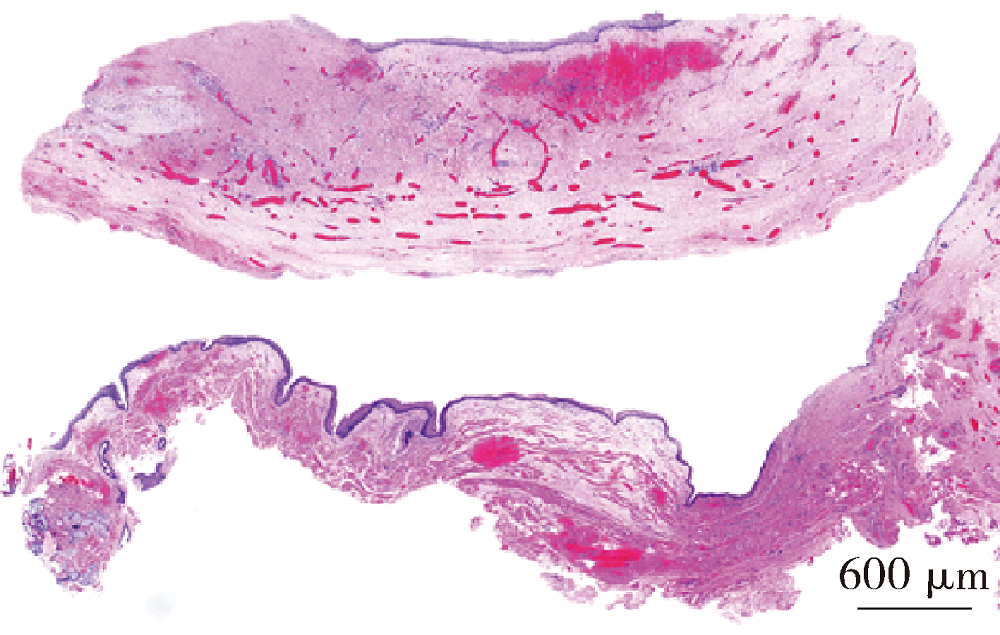
口外型舌下囊肿发病较少,其主要表现为无口内表征的颌下或颏下区囊性肿物,临床上易造成误诊误治。本文报道1例以耳后区巨大肿物为主要临床表现的口外型舌下腺囊肿。患者无明显诱因出现左耳后区反复肿胀半年,皮肤表面破溃后有黄色黏稠液体溢出。首次于北京大学口腔医院就诊时以左侧鳃裂囊肿继发感染为临床诊断,并于2018年11月在全身麻醉下行“左颈部肿物、瘘管切除术”,术中向颈部解剖追踪瘘道至口底舌下腺附近。术后1个月,患者左侧外耳道有可拉丝的“蛋清样”透明黏性液体流出,考虑为舌下腺囊肿口外型,遂于2019年1月在全身麻醉下于口腔内完整摘除同侧舌下腺。经9个月随访,肿物未见复发,外耳道未见溢液。因此,本病例最后诊断为口外型舌下腺囊肿。本病例提示:口外型舌下腺囊肿也可位于耳后区,其最主要的特征是含有“蛋清样”可拉丝的黏性液体,其治疗方法是口内摘除患侧舌下腺。
中图分类号:
- R783









| [1] | Zhao YF, Jia Y, Chen XM , et al. Clinical review of 580 ranulas[J]. Oral Surq Oral Med Oral Pathol Oral Radiol Endod, 2004,98(3):281-287. |
| [2] | Chen JX, Zenga J, Emerick K , et al. Sublingual gland excision for the surgical management of plunging ranula[J]. Am J Otolarygol, 2018,39(5):497-500. |
| [3] | 赵怡芳, 贾俊 . 舌下腺囊肿手术的疗效与并发症[J]. 中国实用口腔科杂志. 2019,12(2):77-81. |
| [4] | 吴海威, 郑家伟 . 头颈部脉管畸形循证医学治疗进展[J/OL]. 中华口腔医学研究杂志(电子版), 2016, 10(4): 231-237[ 2019- 09- 01]. . |
| [5] | Seront E, Vikkula M, Boon LM . Venous malformations of the head and neck[J]. Otolaryngol Clin North Am, 2018,51(1):173-184. |
| [6] | Lee JY, Lee HY, Kim HJ , et al. Plunging ranulas revisited: a CT study with emphasis on a defect of the mylohyoid muscle as the primary route of lesion propagation[J]. Korean J Radiol, 2016,17(2):264-270. |
| [1] | 陈斌,吴超,刘彬,于涛,王振宇. 脊髓髓内海绵状血管瘤患者不同治疗方式的预后[J]. 北京大学学报(医学版), 2023, 55(4): 652-657. |
| [2] | 王薇,蔡林,高莹,郭晓蕙,张俊清. 原发性醛固酮增多症术后持续性重度高钾血症1例[J]. 北京大学学报(医学版), 2022, 54(2): 376-380. |
| [3] | 洪鹏,田晓军,赵小钰,杨飞龙,刘茁,陆敏,赵磊,马潞林. 肾移植术后双侧乳头状肾癌1例[J]. 北京大学学报(医学版), 2021, 53(4): 811-813. |
| [4] | 王子乔,刘燕鹰,张霞,刘田,任立敏,沈丹华,王屹,栗占国. 17例误诊为IgG4相关疾病患者的临床特点及误诊原因分析[J]. 北京大学学报(医学版), 2019, 51(6): 1025-1031. |
| [5] | 唐琦,林榕城,姚林,张争,郝瀚,张崔建,蔡林,李学松,何志嵩,周利群. 肾癌术后局部复发患者的临床病理特征及预后分析[J]. 北京大学学报(医学版), 2019, 51(4): 628-631. |
| [6] | 王云云,孙葳,黄一宁. 颈椎病误诊为脑梗死1例[J]. 北京大学学报(医学版), 2015, 47(5): 883-884. |
| [7] | 岑溪南, 马明信, 郭辉, 武淑兰, 王颖, 邱志祥, 王文生, 欧晋平, 许蔚林, 董玉君, 朱平, 虞积仁. 原发结外淋巴瘤139例临床及误诊分析[J]. 北京大学学报(医学版), 2003, 35(2): 143-145. |
|
||
