北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (1): 30-34. doi: 10.19723/j.issn.1671-167X.2020.01.005
唾液腺腺样囊性癌淋巴结转移相关的临床病理分析
张晔,张妮,刘晓筱,周传香( )
)
- 北京大学口腔医学院·口腔医院,口腔病理科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
Cervical lymph node metastasis in adenoid cystic carcinoma of the salivary glands: A clinicopathologic study
Ye ZHANG,Ni ZHANG,Xiao-xiao LIU,Chuan-xiang ZHOU()
- Department of Oral Pathology, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
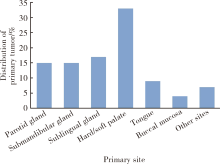
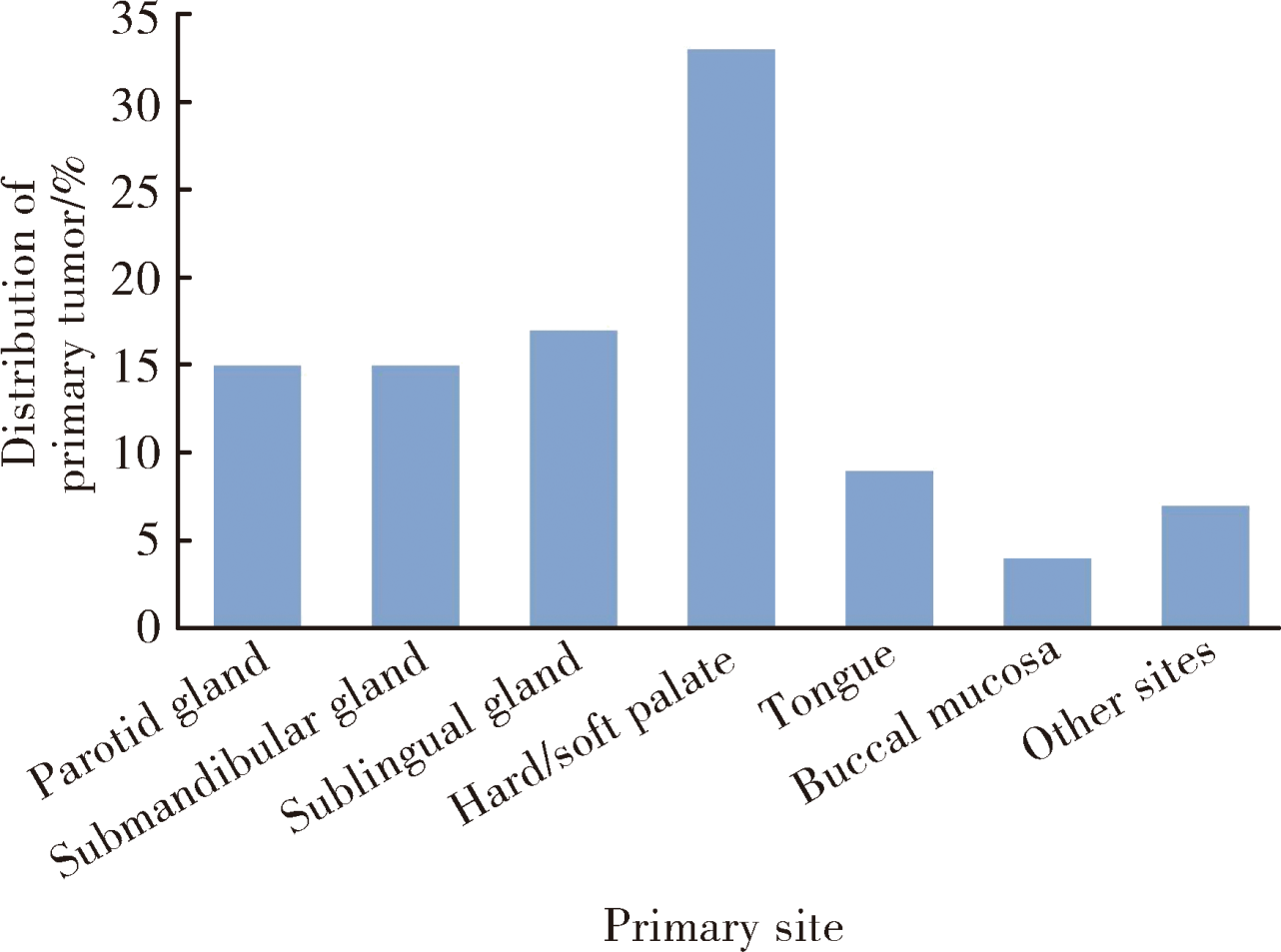
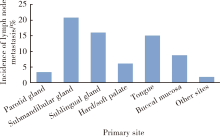
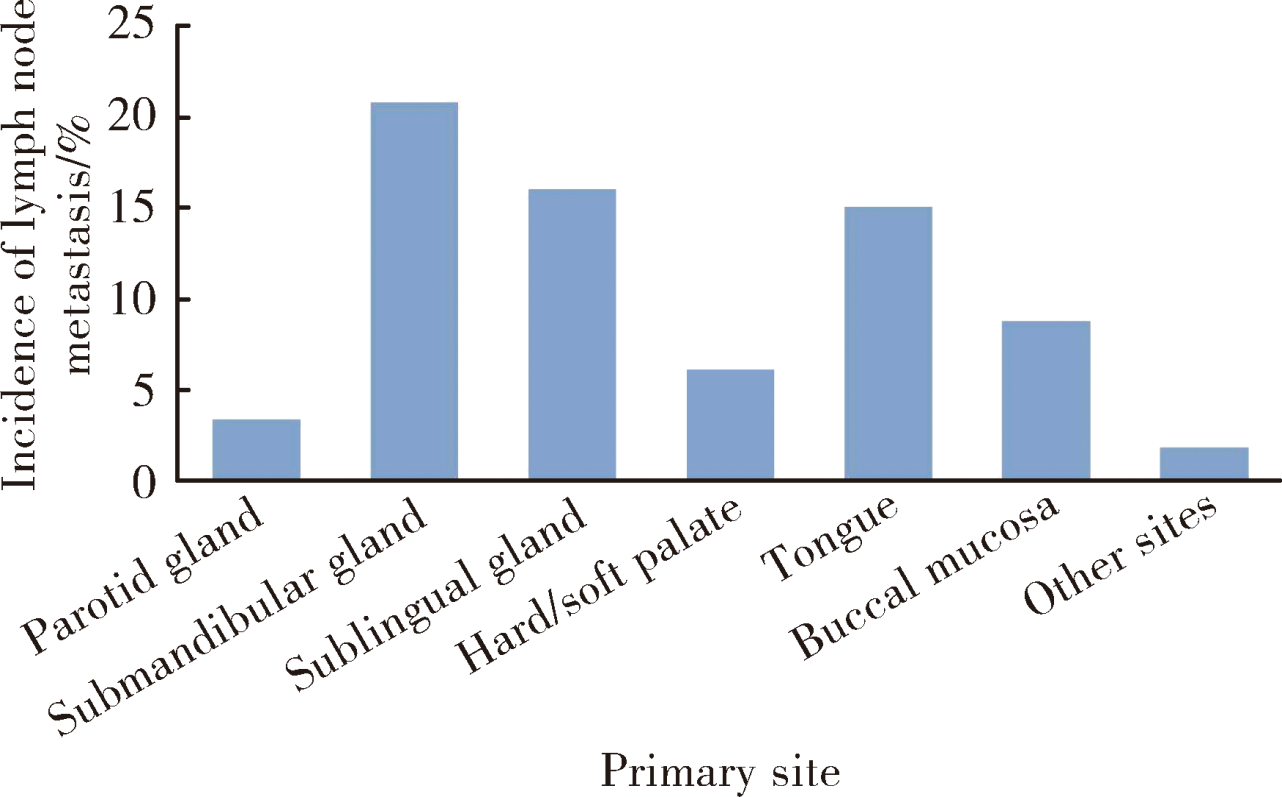
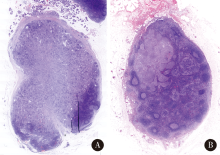
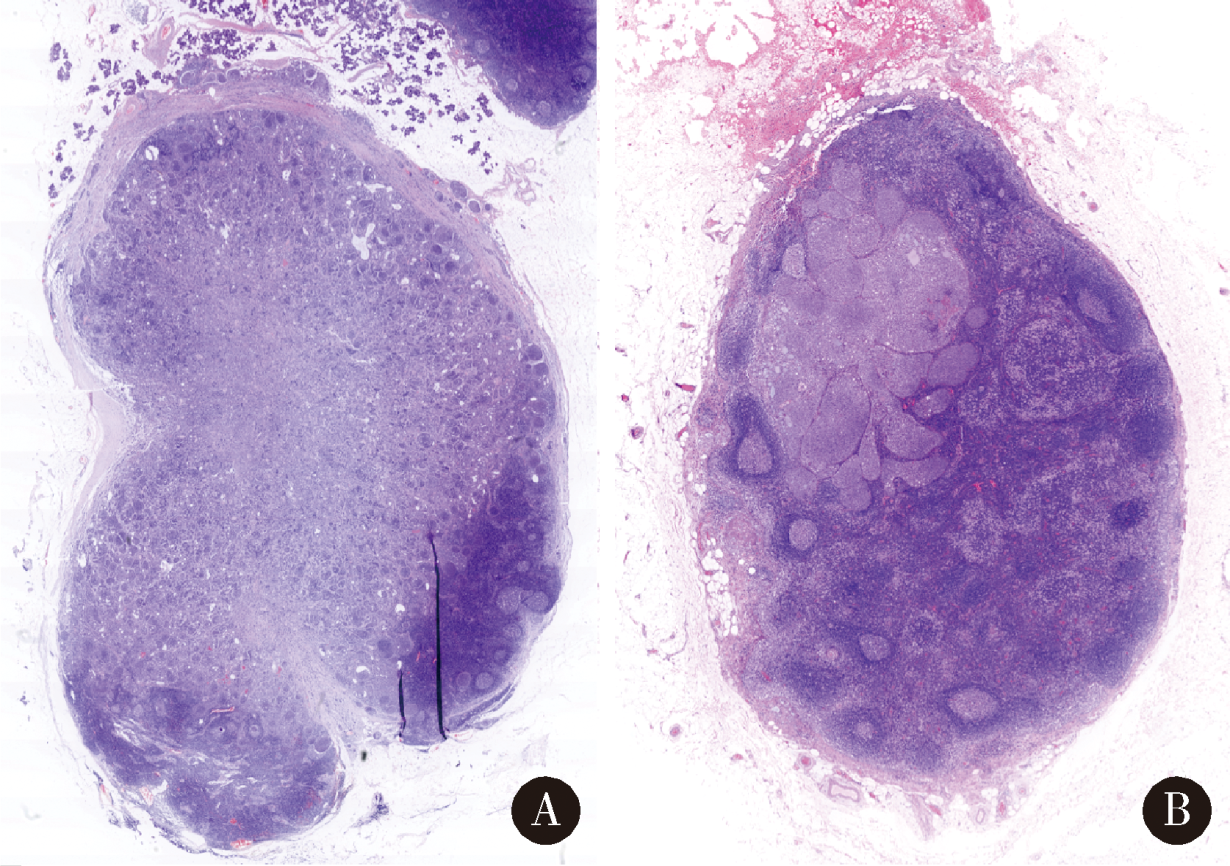
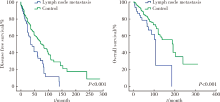
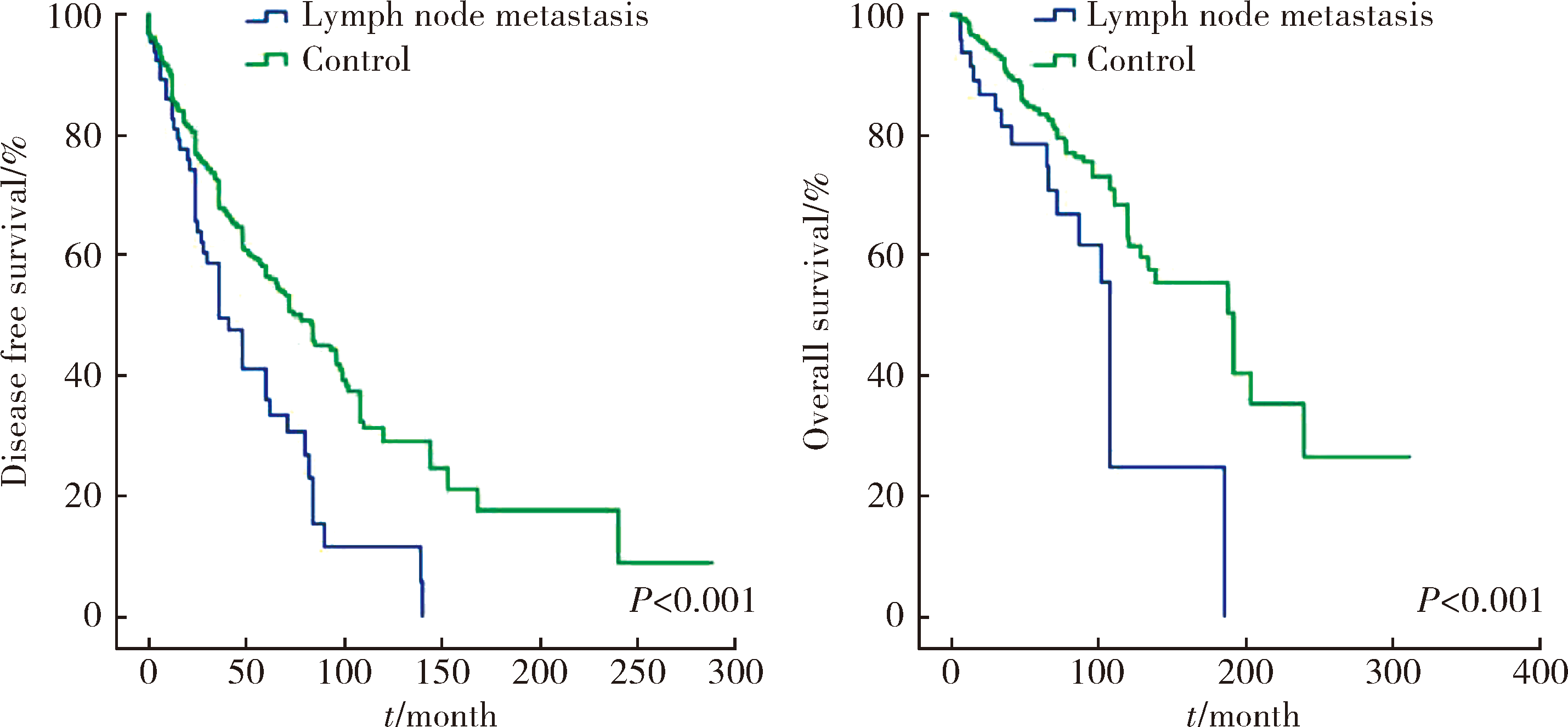
目的:回顾性分析唾液腺腺样囊性癌颈部淋巴结转移的发病率及其临床病理特征。方法:回顾性分析2001年1月至2019年1月在北京大学口腔医院诊治并经病理确诊为腺样囊性癌的798例患者的临床病理资料,对82例发生颈部淋巴结转移的患者进行详细的临床病理及统计学分析。结果:纳入研究的腺样囊性癌患者798例,腭部、舌下口底区域和腮腺区是腺样囊性癌常见的发病部位。经病理学检查证实发生颈部淋巴结转移者82例,总体转移率约10.3%(82/798),其中原发于颌下腺、舌下口底区及舌部的颈部淋巴结转移率较高,分别为20.8%、16.1%、15.1%,而腭部、腮腺原发病例颈部淋巴结转移率较低,分别为6.1%、3.4%。颈Ⅰ、Ⅱ区为常见转移区域,极少累及Ⅳ、Ⅴ区淋巴结。主要转移模式是由癌细胞沿经典的淋巴管/血管通路转移(70.7%),部分颌下及舌下病例不除外直接侵犯淋巴结。82例伴淋巴结转移的患者5年和10年总生存率分别为77.4% 和 20.6%。淋巴结转移阳性组患者总生存率和无瘤生存率均显著低于转移阴性组,且组织学呈现实性型的腺样囊性癌颈部淋巴结转移率显著高于筛孔型和管状型肿瘤。结论:舌下、口底及颌下腺为唾液腺腺样囊性癌颈部淋巴转移常见原发部位,实性型组织学结构与转移率显著正相关,在临床诊治及随访中需要更多关注。
中图分类号:
- R739.87


| [1] | Tian Z, Li L, Wang L , et al. Salivary gland neoplasms in oral and maxillofacial regions: A 23-year retrospective study of 6 982 cases in an eastern Chinese population[J]. Int J Oral Maxillofac Surg, 2010,39(3):235-242. |
| [2] | Gao M, Hao Y, Huang MX , et al. Clinicopathological study of distant metastases of salivary adenoid cystic carcinoma[J]. Int J Oral Maxillofac Surg, 2013,42(8):923-928. |
| [3] | Shen C, Xu T, Huang C , et al. Treatment outcomes and prognostic features in adenoid cystic carcinoma originated from the head and neck[J]. Oral Oncol, 2012,48(5):445-449. |
| [4] | Lloyd S, Yu JB, Wilson LD , et al. Determinants and patterns of survival in adenoid cystic carcinoma of the head and neck, including an analysis of adjuvant radiation therapy[J]. Am J Clin Oncol, 2011,34(1):76-81. |
| [5] | Bhayani MK, Yener M, El-Naggar A , et al. Prognosis and risk factors for early-stage adenoid cystic carcinoma of the major salivary glands[J]. Cancer, 2012,118(11):2872-2878. |
| [6] | Armstrong JG, Harrison LB, Thaler HT , et al. The indications for elective treatment of the neck in cancer of the major salivary glands[J]. Cancer, 1992,69(3):615-619. |
| [7] | Suárez C, Barnes L, Silver CE , et al. Cervical lymph node metastasis in adenoid cystic carcinoma of oral cavity and oropharynx: A collective international review[J]. Auris Nasus Larynx, 2016,43(5):477-484. |
| [8] | Ardekian L, Kokemueller H, Eckardt A , et al. Adenoid cystic carcinoma of the head and neck: A 20 years experience[J]. Int J Oral Maxillofac Surg, 2004,33(1):25-31. |
| [9] | Bianchi B, Copelli C, Cocchi R , et al. Adenoid cystic carcinoma of intraoral minor salivary glands[J]. Oral Oncol, 2008,44(11):1026-1031. |
| [10] | Coca-Pelaz A, Rodrigo JP, Bradley PJ , et al. Adenoid cystic carcinoma of the head and neck: An update[J]. Oral Oncol, 2015,51(7):652-661. |
| [11] | Zhang M, Xu ZF, Tao Y , et al. Clinical analysis of 25 patients with glossal adenoid cystic carcinoma[J]. Int J Stomt, 2009,36(2):148-151. |
| [12] | Min R, Siyi L, Wenjun Y , et al. Salivary gland adenoid cystic carcinoma with cervical lymph node metastasis: A preliminary study of 62 cases[J]. Int J Oral Maxillofac Surg, 2012,41(8):952-957. |
| [13] | Amit M, Binenbaum Y, Sharma K , et al. Incidence of cervical lymph node metastasis and its association with outcomes in patients with adenoid cystic carcinoma. An international collaborative study[J]. Head Neck, 2015,37(7):1032-1037. |
| [14] | Weinreb I, Lee SY, Kim BH , et al. Nineteen-year oncologic outcomes and the benefit of elective neck dissection in salivary gland adenoid cystic carcinoma[J]. Head Neck, 2014,36(12):1796-1801. |
| [15] | Ali S, Palmer FL, Katabi N , et al. Long-term local control rates of patients with adenoid cystic carcinoma of the head and neck managed by surgery and postoperative radiation[J]. Laryngoscope, 2017,127(10):2265-2269. |
| [16] | Nakada M, Nishizaki K, Akagi H , et al. Oncocytic carcinoma of the submandibular gland: a case report and literature review[J]. J Oral Pathol Med, 1998,27(5):225-228. |
| [17] | Amit M, Na’ara S, Sharma K , et al. Elective neck dissection in patients with head and neck adenoid cystic carcinoma: An international collaborative study[J]. Ann Surg Oncol, 2015,22(4):1353-1359. |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 杨静, 许晓韵, 郑丹妮, 凌晓彤, 屈留洋, 柳登高. 544例慢性唾液腺炎的临床与影像学特点及病因分析[J]. 北京大学学报(医学版), 2026, 58(3): 650-657. |
| [4] | 步召德, 冯梦宇, 季科. 早期胃癌行前哨淋巴结导航手术的实践与思考[J]. 北京大学学报(医学版), 2026, 58(2): 239-243. |
| [5] | 王海, 江一舟. 靶向血管治疗在乳腺癌精准治疗中的分子机制与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 251-256. |
| [6] | 罗必显, 刘洪铭, 谢伟勋, 龚渭华. 产甲胎蛋白胃癌的新临床特征和前沿科学问题[J]. 北京大学学报(医学版), 2026, 58(2): 257-265. |
| [7] | 付浩, 申潞艳, 黄冰洋, 马少华. 免疫治疗背景下食管鳞状细胞癌围手术期治疗的临床思考[J]. 北京大学学报(医学版), 2026, 58(2): 266-271. |
| [8] | 殷昊明, 王子杰, 舒帆, 张展奕, 梁会, 张树栋. 肾透明细胞癌FABP6基因长转录本的表达及意义[J]. 北京大学学报(医学版), 2026, 58(2): 393-398. |
| [9] | 李嘉临, 陈力侨, 唐家天, 吴艳, 王安强. 胃肝样腺癌转化治疗1例[J]. 北京大学学报(医学版), 2026, 58(2): 399-404. |
| [10] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [11] | 潘子晨, 陈凯, 侯钰坤, 杨博涵, 张继新, 马永蔌, 田孝东, 杨尹默. 胰腺腺鳞癌临床病理特征与分子机制研究进展[J]. 北京大学学报(医学版), 2026, 58(2): 431-435. |
| [12] | 丛馨, 苏家增, 吴立玲, 丁冲, 李巍, 俞光岩. 唾液腺非肿瘤性疾病诊治研究进展[J]. 北京大学学报(医学版), 2026, 58(1): 1-9. |
| [13] | 杨雨婷, 屈留洋, 郑丹妮, 凌晓彤, 许晓韵, 柳登高. 1 812例唾液腺结石患者的人口学特征和临床特点[J]. 北京大学学报(医学版), 2026, 58(1): 153-159. |
| [14] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [15] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
|
||
