北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (4): 692-696. doi: 10.19723/j.issn.1671-167X.2020.04.018
内镜联合超声与单纯超声引导建立皮肾通道在多镜联合术中的应用
康宁,蒋一航,蒋宇光,吴栗洋,张际青,牛亦农,张军晖( )
)
- 首都医科大学附属北京朝阳医院泌尿外科,北京 100020
Endoscopic combined ultrasound-guided access vs. ultrasound-guided access in endoscopic combined intrarenal surgery
Ning KANG,Yi-hang JIANG,Yu-guang JIANG,Li-yang WU,Ji-qing ZHANG,Yi-nong NIU,Jun-hui ZHANG()
- Department of Urology Beijing Chao-Yang Hospital, Capital Medical University, Beijing 100020, China
摘要:
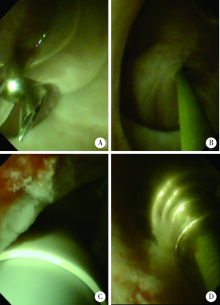
目的: 评估多镜联合(endoscopic combined intrarenal surgery,ECIRS)治疗上尿路结石术中内镜联合超声引导(endoscopic assisted ultrasound-guided access, EUGA)和单纯超声引导(ultrasound-guided access,UGA)建立皮肾通道的效果。方法: 选择2017年1月至2019年10月首都医科大学附属北京朝阳医院采用ECIRS治疗复杂上尿路结石的病例进行回顾性分析,共收集病例53例,分析其建立皮肾通道的方法。患者全身麻醉下斜仰卧截石位实施手术,根据术中输尿管软镜能否有效观察目标肾盏并引导皮肾通道的建立分为2组,其中25例采用输尿管软镜联合超声引导,穿刺和通道扩张全过程于输尿管软镜直视下完成,28例采用单纯超声引导建立皮肾通道。对两组术前基线情况、结石大小、受累肾盏数量、肾积水比例进行统计。对数据进行对比分析,手术相关数据包括手术用时,建立皮肾通道用时、通道建立重复操作比例,血红蛋白变化、围手术期并发症以及清石率等。结果: 53例多镜联合手术均成功完成,EUGA组与UGA组年龄、性别比例差异无统计学意义。EUGA组与UGA组BMI分别为(29.21±3.14) kg/m2和(28.53±2.56) kg/m2,结石负荷分别为(37.68±6.89) mm和(35.53±6.52) mm,受累肾盏数量分别为 2.72±0.68和 2.86±0.71,肾积水病例所占比例分别为56.0%和46.4%,组间差异均无统计学意义(P>0.05)。EUGA组与UGA组手术相关数据中手术用时分别为(93.0±12.2) min和(96.8±14.2) min,血色素下降分别为(6.56±2.16) g/L 和(7.54±2.64) g/L,清石率分别为92%和92.8%,住院时间分别为(5.52±0.59) d和(5.64±0.62) d,术后并发症分别为8.0%和7.2%,EUGA组血尿和泌尿系感染各1例,UGA组泌尿系感染2例,2组均无输血病例,组间比较差异均无统计学意义(P>0.05)。EUGA组与UGA组建立皮肾通道用时分别为(4.0±0.7) min和(6.8±2.6) min,EUGA组用时少于UGA组(P<0.01), EUGA组无重复通道建立病例,UGA组4例出现重复通道建立,EUG组通道建立重复操作比例低于UGA组(P<0.05)。结论: 多镜联合手术中采用内镜联合超声引导建立皮肾通道安全有效,可以缩短建立皮肾通道用时,提高通道建立一次性成功率。
中图分类号:
- R691.4

| [1] |
Zeng G, Mai Z, Xia S, et al. Prevalence of kidney stones in China: an ultrasonography based cross-sectional study[J]. BJU Int, 2017,120(1):109-116.
doi: 10.1111/bju.13828 pmid: 28236332 |
| [2] | Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American Urological Association/Endourological Society Guideline. PART Ⅱ[J]. J Urol, 2016,196(4):1161-1169. |
| [3] |
Türk C, Petřík A, Sarica K, et al. EAU guidelines on interventional treatment for urolithiasis[J]. Eur Urol, 2016,69(3):475-482.
doi: 10.1016/j.eururo.2015.07.041 pmid: 26344917 |
| [4] | 那彦群, 叶章群, 孙颖浩, 等. 中国泌尿外科疾病诊断治疗指南2014版[M]. 北京: 人民卫生出版社, 2013: 1. |
| [5] |
Atis G, Culpan M, Pelit ES, et al. Comparison of percutaneous nephrolithotomy and retrograde intrarenal surgery in treating 20-40 mm renal stones[J]. Urol J, 2017,14(2):2995-2999.
pmid: 28299761 |
| [6] | 杨波, 李建兴, 胡卫国, 等. 两步法建立标准通道经皮肾镜取石3 052例临床报告[J]. 北京大学学报(医学版), 2010,42(4):447-450. |
| [7] |
Kwon O, Park J, Cho MC, et al. Feasibility of single-session endoscopic combined intrarenal surgery for ipsilateral large renal stones and retrograde intrarenal surgery for contralateral renal stones: initial experience[J]. INT J Urol, 2017,24(5):377-382.
pmid: 28281312 |
| [8] | Ping H, Zhang JH, Wang MS, et al. Endoscopic combined intrarenal surgery for the treatment of postpercutaneous nephrolithotomy residual stones[J]. Chin Med J (Engl), 2016,129(23):2885-2887. |
| [9] |
Wen J, Xu G, Du C, et al. Minimally invasive percutaneous nephrolithotomy versus endoscopic combined intrarenal surgery with flexible ureteroscope for partial staghorn calculi: a randomised controlled trial[J]. Int J Surg, 2016,28:22-27.
pmid: 26898135 |
| [10] |
Grasso M, Lang G, Taylor FC. Flexible ureteroscopically assisted percutaneous renal access[J]. Tech Urol, 1995,1(1):39-43.
pmid: 9118366 |
| [11] | Chi T, Masic S, Li J, et al. Ultrasound guidance for renal tract access and dilation reduces radiation exposure during percutaneous nephrolithotomy[J/OL]. Adv Urol, 2016 (2016): 1-8 [2020-04-10]. https://www.hindawi.com/journals/au/2016/3840697/. |
| [12] |
Ng FC, Yam WL, Lim TY, et al. Ultrasound-guided percutaneous nephrolithotomy: advantages and limitations[J]. Investig Clin Urol, 2017,58(5):346-352.
pmid: 28868506 |
| [13] | de la Rosette J, Assimos D, Desai M, et al. The clinical research office of the endourological society percutaneous nephrolithotomy globalstudy: indications, complications, and outcomes in 5 803 patients[J]. J Endourol, 2011,25(1):11-17. |
| [14] |
Kawahara T, Ito H, Terao H, et al. Ureteroscopy assisted retrograde nephrostomy: a new technique for percutaneous nephroli-thotomy (PCNL)[J]. BJU Int, 2011,110(4):588-590.
pmid: 22142188 |
| [1] | 汤易, 赵雪竹, 杨旭, 贾惠梅, 刘云松. 超声洁治对种植修复基台螺丝扭矩的影响[J]. 北京大学学报(医学版), 2026, 58(1): 84-88. |
| [2] | 王翠萍, 陈哲, 程永静. 超微血流成像评估与膝骨关节炎临床症状的关联研究[J]. 北京大学学报(医学版), 2025, 57(6): 1096-1100. |
| [3] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [4] | 朱灵丽, 唐琳, 李博文, 王梅, 刘玉华. 两种玷污层去除方法对牙本质表面性能的影响[J]. 北京大学学报(医学版), 2025, 57(2): 340-346. |
| [5] | 王明瑞, 赖金惠, 姬家祥, 唐鑫伟, 胡浩浦, 王起, 许克新, 徐涛, 胡浩. 使用中文版威斯康星结石生活质量问卷预测肾结石患者生活质量降低的危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1069-1074. |
| [6] | 原晋芳, 王新利, 崔蕴璞, 王雪梅. 尿促黄体生成素在女童中枢性性早熟预测中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 788-793. |
| [7] | 王明瑞,刘军,熊六林,于路平,胡浩,许克新,徐涛. 经皮微通道-微电子肾镜-微超声探针碎石术治疗1.5~2.5 cm肾结石的疗效和安全性[J]. 北京大学学报(医学版), 2024, 56(4): 605-609. |
| [8] | 郑生旗,花天池,殷桂草,张伟,姚曳,李一帆. 甘油三酯葡萄糖指数与男性肾结石风险的关联[J]. 北京大学学报(医学版), 2024, 56(4): 610-616. |
| [9] | 杨捷,冯杰莉,张树栋,马潞林,郑清. 经食管超声心动图在肾切除术联合Mayo Ⅲ~Ⅳ级静脉瘤栓取栓术不同手术方式中的临床作用[J]. 北京大学学报(医学版), 2024, 56(4): 631-635. |
| [10] | 陈延,李况蒙,洪锴,张树栋,程建星,郑仲杰,唐文豪,赵连明,张海涛,姜辉,林浩成. 阴茎海绵体注射试验对阴茎血管功能影响的回顾性研究[J]. 北京大学学报(医学版), 2024, 56(4): 680-686. |
| [11] | 魏越,姚兰,陆希,王军,蔺莉,刘鲲鹏. 胃超声检查评估剖宫产产妇术前饮用碳水化合物后胃排空的效果[J]. 北京大学学报(医学版), 2023, 55(6): 1082-1087. |
| [12] | 魏越,陆希,张静,刘鲲鹏,王永军,姚兰. 术前2 h口服碳水化合物对妇科腹腔镜特殊体位手术患者胃容量及反流误吸风险的影响[J]. 北京大学学报(医学版), 2023, 55(5): 893-898. |
| [13] | 田聪,刘军,杨波,乔佳佳,黄晓波,许清泉. 经皮肾镜取石术中异常肾盂黏膜活检结果分析[J]. 北京大学学报(医学版), 2023, 55(5): 948-952. |
| [14] | 傅强,高冠英,徐雁,林卓华,孙由静,崔立刚. 无症状髋关节前上盂唇撕裂超声与磁共振检查的对比研究[J]. 北京大学学报(医学版), 2023, 55(4): 665-669. |
| [15] | 刘杨,程昉,王艳玲,艾香艳,朱振航,赵福涛. 唾液腺超声对干燥综合征的诊断价值[J]. 北京大学学报(医学版), 2022, 54(6): 1123-1127. |
|
||
