北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (4): 692-696. doi: 10.19723/j.issn.1671-167X.2021.04.012
前列腺尖部深度与腹腔镜前列腺癌根治术后早期控尿功能恢复的相关性
张帆,黄晓娟,杨斌,颜野,刘承,张树栋,黄毅( ),马潞林
),马潞林
- 北京大学第三医院泌尿外科,北京 100191
Relationship between prostate apex depth and early recovery of urinary continence after laparoscopic radical prostatectomy
ZHANG Fan,HUANG Xiao-juan,YANG Bin,YAN Ye,LIU Cheng,ZHANG Shu-dong,HUANG Yi(),MA Lu-lin
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
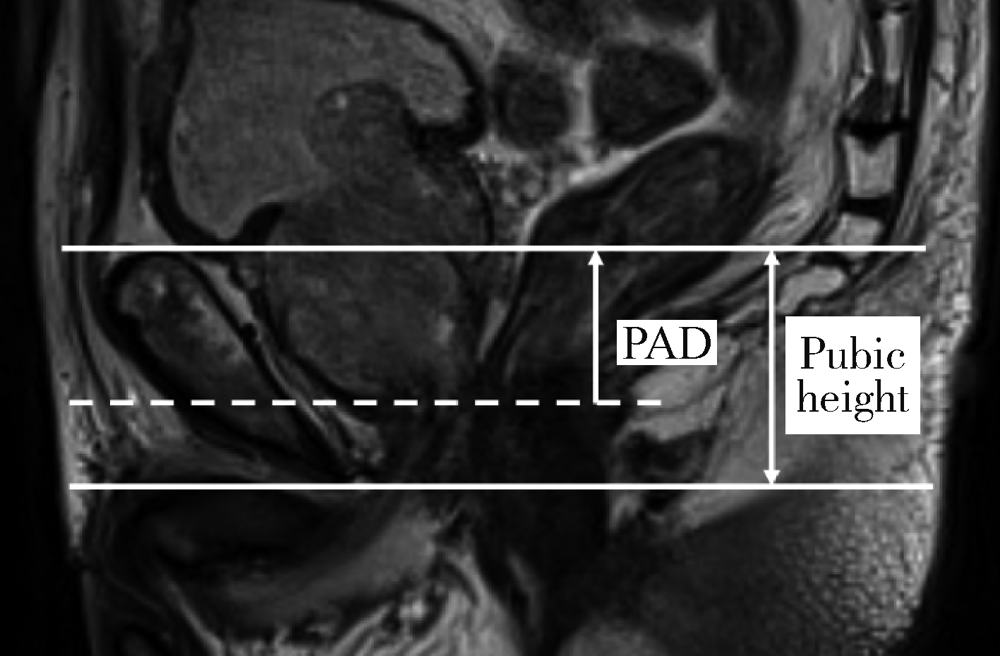
目的: 探讨术前前列腺尖部深度(prostate apex depth,PAD)与腹腔镜前列腺癌根治术(laparoscopic radical prostatectomy,LRP)后早期(3个月)控尿功能恢复的相关性。方法: 本组184例患者均经前列腺穿刺活检诊断为前列腺腺癌并于北京大学第三医院泌尿外科行LRP手术,前列腺穿刺活检前均完善MRI检查,将PAD定义为MRI矢状位前列腺尖部至耻骨上缘水平线的垂直距离,将前列腺尖部深度比(PAD ratio,PADR)定义为PAD/耻骨上缘与下缘水平线间的垂直距离(耻骨高度)。所有患者均行腹膜外LRP,自术后第一个月起每月对患者的控尿功能恢复情况进行随访,以全天不需要使用尿垫为控尿功能恢复标准。应用Logistic多因素回归分析影响术后早期控尿功能恢复的危险因素,Log-rank检验比较各组间术后控尿功能恢复曲线的统计学意义。结果: 184例患者平均年龄(69.0±7.7)岁,平均体重指数(25.07±3.29) kg/m2,平均穿刺前前列腺特异性抗原(16.80±21.99) μg/L,穿刺Gleason评分6分、7分和≥8分者分别为14例(7.6%)、81例(44.0%)和89例(48.4%),临床分期T1/T2期157例(85.3%)、T3期27例(14.7%)。术前MRI测量平均前列腺体积(prostatic volume,PV)为(39.35±25.25) mL,平均膜性尿道长度(membranous urethral length,MUL)为(14.0±3.7) mm;PAD为15~40 mm,平均(24.52±4.97)mm;PADR为0.42~1.00,平均0.70±0.14。所有患者手术均顺利完成,随访3个月和12个月完全控尿率分别为62.0%(114/184)和96.2%(177/184);术后早期(3个月)尿失禁的单因素分析中,PV(P=0.049)、MUL(P<0.001)和PADR(P=0.005)具有统计学意义,被纳入多因素分析;多因素分析结果显示,MUL<14 mm(P<0.001)和PADR≥0.70(P=0.032)是术后早期尿失禁发生的独立危险因素。采用Kaplan-Meier法绘制不同PV、MUL和PADR患者术后控尿功能恢复曲线,Log-rank检验示不同PV(P=0.001)、MUL(P<0.001)和PADR(P<0.001)分组控尿功能恢复的差异具有统计学意义。结论: MUL、PADR、PV与LRP术后控尿功能恢复存在相关性,术前MUL较短和PADR较高是术后早期尿失禁发生的独立危险因素。
中图分类号:
- R737.25



| [1] |
Siegel RL, Miller KD, Fuchis HE, et al. Cancer statistics, 2021 [J]. CA Cancer J Clin, 2021, 71(1):7-33.
doi: 10.3322/caac.v71.1 |
| [2] |
Wong MC, Goggins WB, Wang HH, et al. Global incidence and mortality for prostate cancer: Analysis of temporal patterns and trends in 36 countries [J]. Eur Urol, 2016, 70(5):862-874.
doi: 10.1016/j.eururo.2016.05.043 |
| [3] |
Mohler JL, Anarakis ES, Armstrong AJ, et al. Prostate cancer, version 2.2019, NCCN clinical practice guidelines in oncology [J]. J Natl Compr Canc Netw, 2019, 17(5):479-505.
doi: 10.6004/jnccn.2019.0023 |
| [4] |
Mungovan SF, Sandhu JS, Akin O, et al. Preoperative membranous urethral length measurement and continence recovery following radical prostatectomy: A systematic review and meta-analysis [J]. Euro Urol, 2017, 71(3):368-378.
doi: 10.1016/j.eururo.2016.06.023 |
| [5] |
Macura KJ, Genadry RR. Female urinary incontinence: Pathophysiology, methods of evaluation and role of MR imaging [J]. Abdom Imaging, 2008, 33(3):371-380.
doi: 10.1007/s00261-007-9257-6 |
| [6] |
Huang HC, Jiang YH, Lin VC, et al. Possible predictor of early recovery on urinary continence after laparoscopic radical prostatectomy: Bladder neck level and urodynamic parameters [J]. J Formos Med Assoc, 2019, 118(1 Pt 2):237-243.
doi: 10.1016/j.jfma.2018.04.009 |
| [7] |
Kageyama S, Yoshida T, Nagasawa M, et al. The location of the bladder neck in postoperative cystography predicts continence convalescence after radical prostatectomy [J]. BMC Urol, 2018, 18(1):52.
doi: 10.1186/s12894-018-0370-3 pmid: 29848326 |
| [8] |
Ficarra V, Novara G, Rosen RC, et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy [J]. Eur Urol, 2012, 62(3):405-417.
doi: 10.1016/j.eururo.2012.05.045 |
| [9] |
Heesakkeers J, Farag F, Bauer RM, et al. Pathophysiology and contributing factors in postprostatectomy incontinence: A review [J]. Eur Urol, 2017, 71(6):936-944.
doi: 10.1016/j.eururo.2016.09.031 |
| [10] |
Pavlovich CP, Rocco B, Druskin SC, et al. Urinary continence recovery after radical prostatectomy: Anatomical/reconstructive and nerve-sparing techniques to improve outcomes [J]. BJU Int, 2017, 120(2):185-196.
doi: 10.1111/bju.2017.120.issue-2 |
| [11] |
Walz J, Epstin JI, Ganzer R, et al. A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy: An update [J]. Eur Urol, 2016, 70(2):301-311.
doi: 10.1016/j.eururo.2016.01.026 |
| [12] |
Covas Moschovas M, Bhat S, Onol FF, et al. Modified apical dissection and lateral prostatic fascia preservation improves early postoperative functional recovery in robotic-assisted laparoscopic radical prostatectomy: Results from a propensity score-matched analysis [J]. Eur Urol, 2020, 78(6):875-884.
doi: 10.1016/j.eururo.2020.05.041 |
| [13] |
Lee YJ, Jung JW, Lee S, et al. Contemporary trends in radical prostatectomy and predictors of recovery of urinary continence in men aged over 70 years: Comparisons between cohorts aged over 70 and less than 70 years [J]. Asian J Androl, 2020, 22(3):280-286.
doi: 10.4103/aja.aja_62_19 |
| [14] | 张帆, 肖春雷, 张树栋, 等. 前列腺体积及前列腺突入膀胱长度与腹腔镜前列腺癌根治术后控尿功能恢复的相关性 [J]. 北京大学学报(医学版), 2018, 50(4):621-625. |
| [15] |
Grivas N, van Der RR, Schouten D, et al. Quantitative assessment of fascia preservation improves the prediction of membranous urethral length and inner levator distance on continence outcome after robot‐assisted radical prostatectomy [J]. Neurourol Urodyn, 2017, 37(1):417-425.
doi: 10.1002/nau.v37.1 |
| [16] |
Yang B, Zhang F, Xiao C, et al. Impact of preoperative magnetic resonance imaging anatomic features on urinary continence recovery after laparoscopic radical prostatectomy [J]. Urol Int, 2020, 104(3/4):239-246.
doi: 10.1159/000506021 |
| [17] |
Matsushita K, Kent MT, Vickers AJ, et al. Preoperative predictive model of recovery of urinary continence after radical prostatectomy [J]. BJU Int, 2015, 116(4):577-583.
doi: 10.1111/bju.13087 pmid: 25682782 |
| [18] |
Kadono Y, Nohara T, Kawaguchi S, et al. Investigating the mechanism underlying urinary continence recovery after radical prostatectomy: Effectiveness of a longer urethral stump to prevent urinary incontinence [J]. BJU Int, 2018, 122(3):456-462.
doi: 10.1111/bju.14181 |
| [19] | Fukui S, Kagebayashi Y, Iemura Y, et al. Preoperative MRI parameters predict urinary continence after robot-assisted laparoscopic prostatectomy in prostatic cancer patients [J]. Diagnostics (Basel), 2019, 9(3):102. |
| [1] | 郭睿霖, 张蕾, 王宇, 王晓庆, 王潇潇, 年凇汶, 张丽慧, 肖冰冰, 陆叶. 经闭孔尿道中段无张力悬吊改良术治疗女性压力性尿失禁的疗效[J]. 北京大学学报(医学版), 2026, 58(2): 337-341. |
| [2] | 李斌, 梁寒. 机器人胃癌根治术:研究进展与实践挑战[J]. 北京大学学报(医学版), 2026, 58(2): 416-422. |
| [3] | 王起, 柯涵炜, 丁泽华, 张维宇, 张晓鹏, 徐涛, 许克新. 耻骨后与经闭孔尿道中段悬吊术对术后最大尿流率及残余尿量的影响[J]. 北京大学学报(医学版), 2025, 57(4): 717-720. |
| [4] | 王焕瑞, 赖世聪, 胡浩浦, 丁泽华, 徐涛, 胡浩. 腹腔镜与输尿管软镜联合定位治疗复杂输尿管狭窄的疗效分析[J]. 北京大学学报(医学版), 2025, 57(4): 784-788. |
| [5] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [6] | 于书慧,韩佳凝,钟丽君,陈聪语,肖云翔,黄燕波,杨洋,车新艳. 术前盆底肌电生理参数对前列腺癌根治性切除术后早期尿失禁的预测价值[J]. 北京大学学报(医学版), 2024, 56(4): 594-599. |
| [7] | 李雨清,王飚,乔鹏,王玮,关星. 经耻骨后尿道中段悬吊带术治疗女性复发性压力性尿失禁的中长期疗效[J]. 北京大学学报(医学版), 2024, 56(4): 600-604. |
| [8] | 毛海,张帆,张展奕,颜野,郝一昌,黄毅,马潞林,褚红玲,张树栋. 基于MRI前列腺腺体相关参数构建腹腔镜前列腺癌术后尿失禁的预测模型[J]. 北京大学学报(医学版), 2023, 55(5): 818-824. |
| [9] | 邱敏,宗有龙,王滨帅,杨斌,徐楚潇,孙争辉,陆敏,赵磊,卢剑,刘承,田晓军,马潞林. 腹腔镜肾部分切除术治疗中高复杂程度肾肿瘤的效果[J]. 北京大学学报(医学版), 2023, 55(5): 833-837. |
| [10] | 张展奕,张帆,颜野,曹财广,李长剑,邓绍晖,孙悦皓,黄天亮,管允鹤,李楠,陆敏,胡振华,张树栋. 近红外荧光靶向探针用于前列腺神经血管束术中成像[J]. 北京大学学报(医学版), 2023, 55(5): 843-850. |
| [11] | 刘慧丽,吕彦函,王晓晓,李民. 老年患者腹腔镜泌尿系肿瘤根治术后慢性疼痛的影响因素[J]. 北京大学学报(医学版), 2023, 55(5): 851-856. |
| [12] | 许素环,王蓓蓓,庞秋颖,钟丽君,丁炎明,黄燕波,车新艳. 等体温膀胱冲洗对经尿道前列腺电切术患者干预效果的meta分析[J]. 北京大学学报(医学版), 2023, 55(4): 676-683. |
| [13] | 张铃福,侯纯升,徐智,王立新,凌晓锋,王港,崔龙,修典荣. 腹腔镜下经胆囊管胆管引流联合胆总管探查取石术治疗复杂胆管结石的临床效果[J]. 北京大学学报(医学版), 2022, 54(6): 1185-1189. |
| [14] | 安立哲,熊六林,陈亮,王焕瑞,陈伟男,黄晓波. 腹腔镜肾盂成形术联合肾盂镜超声碎石取石术治疗肾盂输尿管连接部梗阻合并肾结石[J]. 北京大学学报(医学版), 2022, 54(4): 746-750. |
| [15] | 张帆,陈曲,郝一昌,颜野,刘承,黄毅,马潞林. 术前及术后膜性尿道长度与腹腔镜根治性前列腺切除术后控尿功能恢复的相关性[J]. 北京大学学报(医学版), 2022, 54(2): 299-303. |
|
||
