北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (4): 712-718. doi: 10.19723/j.issn.1671-167X.2022.04.021
无症状中国年轻人颈椎矢状位曲度正常值及其与全脊柱平衡的关系
唐彦超1,赵文奎2,于淼1,刘晓光1,*( )
)
- 1. 北京大学第三医院骨科,北京 100191
2. 北京大学第三医院疼痛科,北京 100191
Normative values of cervical sagittal alignment according to the whole spine balance: Based on 126 asymptomatic Chinese young adults
Yan-chao TANG1,Wen-kui ZHAO2,Miao YU1,Xiao-guang LIU1,*()
- 1. Department of Orthopaedics, Peking University Third Hospital, Beijing 100191, China
2. Pain Medicine Center, Peking University Third Hospital, Beijing 100191, China
摘要:
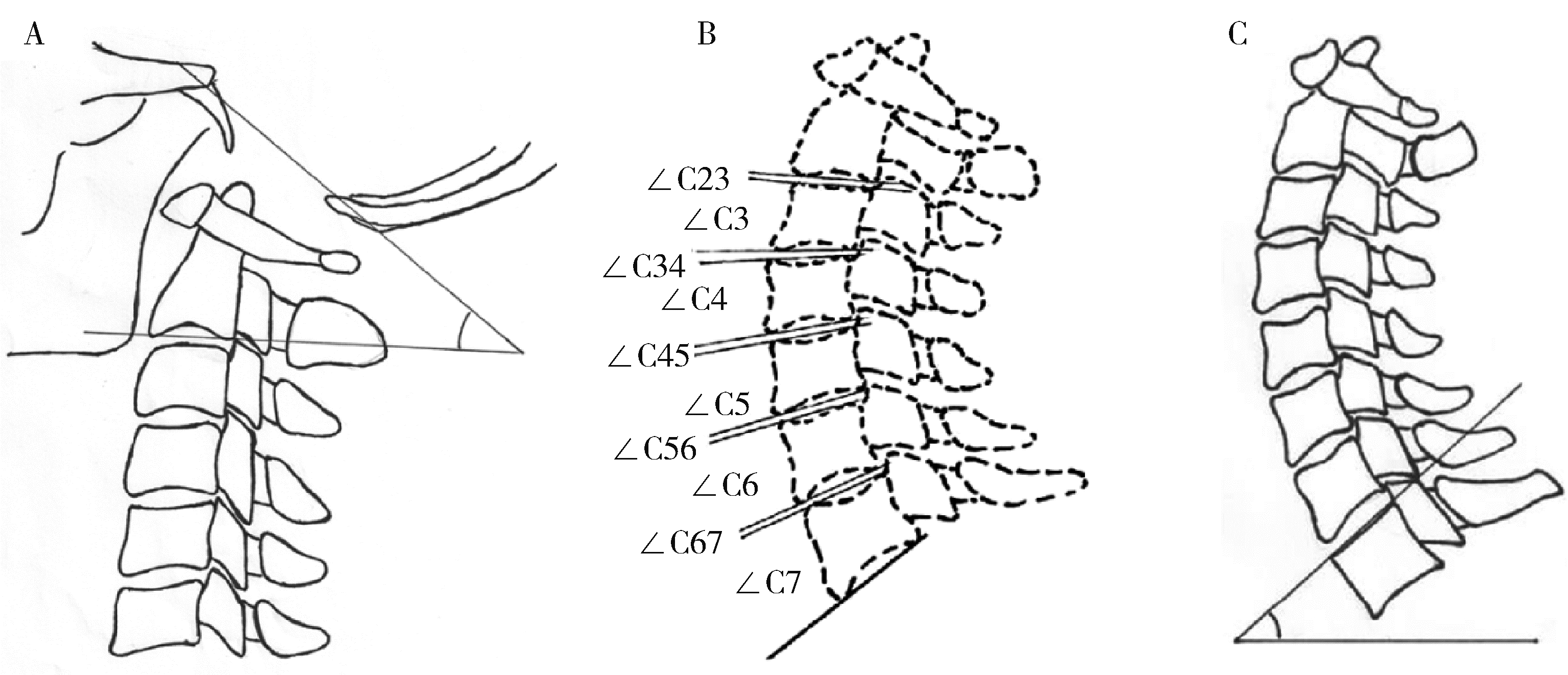
目的: 探讨无症状中国年轻人颈椎矢状位曲度的正常值及其与全脊柱平衡的关系。方法: 2011年11月—2014年12月招募并选择年龄18~30岁的志愿者行全脊柱侧位X线检查,在X线片上测量指标包括C0-C2角、从C2-C3到C6-C7的间盘角、从C3到C7的椎体角、T1倾斜角、胸椎后凸角(thoracic kyphosis, TK)、腰椎前凸角(lumbar lordosis, LL)、骨盆入射角(pelvic incidence, PI)、骶骨倾斜角(sacral slope, SS)、C2-C7矢状轴向垂线(C2-C7 sagittal vertical axis, C2-C7SVA)、头重心至C7的矢状位轴向垂线(center of gravity of head to C7SVA, CGH-C7SVA)、C7到S1的矢状位轴向垂线(C7-S1SVA)。依据脊柱骨盆矢状位形态进行Roussouly分型,比较不同Roussouly分型下的颈椎曲度及形态。结果: 共纳入126名志愿者参与研究,其中男性67名,女性59名,平均年龄(21.4±2.3)岁。C0-C7前凸角平均为26.0°±12.8°,其中C0-C2前凸角平均为15.2°±6.7°,C2-C3到C6-C7间盘前凸角总和平均为9.1°±12.1°,C3到C7的椎体前凸角总和平均仅为1.4°±10.2°。C2-C7SVA(18.6±7.9) mm和CGH-C7SVA[(22.9±12.3) mm]由C7-S1SVA[(-21.6±31.0) mm]完美代偿。不同的Roussouly分型间颈椎曲度差异有统计学意义(P < 0.01)。颈椎曲度与T1倾斜角(P < 0.01)、胸椎后凸角(P < 0.01)有显着相关性。从T1倾斜角到C0-C2角,相邻节段间盘角之间存在显著相关性(P < 0.05)。结论: 测量并计算了无症状中国年轻人颈椎椎体角和间盘角的正常值,发现颈椎前凸主要发生在C0-C2和椎间盘水平,这些角度受到其他脊柱部位形态(T1倾斜角、胸椎后凸角和Roussouly分型)的影响,且相邻间盘角之间存在显著的相关性。
中图分类号:
- R681.5



| 1 |
Le Huec JC , Demezon H , Aunoble S . Sagittal parameters of global cervical balance using EOS imaging: normative values from a prospective cohort of asymptomatic volunteers[J]. Eur Spine J, 2015, 24 (1): 63- 71.
doi: 10.1007/s00586-014-3632-0 |
| 2 |
Lee SH , Son ES , Seo EM , et al. Factors determining cervical spine sagittal balance in asymptomatic adults: correlation with spinopelvic balance and thoracic inlet alignment[J]. Spine J, 2015, 15 (4): 705- 712.
doi: 10.1016/j.spinee.2013.06.059 |
| 3 |
Nunez-Pereira S , Hitzl W , Bullmann V , et al. Sagittal balance of the cervical spine: an analysis of occipitocervical and spinopelvic interdependence, with C-7 slope as a marker of cervical and spinopelvic alignment[J]. J Neurosurg Spine, 2015, 23 (1): 16- 23.
doi: 10.3171/2014.11.SPINE14368 |
| 4 |
Sakai K , Yoshii T , Hirai T , et al. Cervical sagittal imbalance is a predictor of kyphotic deformity after laminoplasty in cervical spondylotic myelopathy patients without preoperative kyphotic alignment[J]. Spine (Phila Pa 1976), 2016, 41 (4): 299- 305.
doi: 10.1097/BRS.0000000000001206 |
| 5 |
Kato M , Namikawa T , Matsumura A , et al. Effect of cervical sagittal balance on laminoplasty in patients with cervical myelopathy[J]. Global Spine J, 2017, 7 (2): 154- 161.
doi: 10.1177/2192568217694011 |
| 6 |
Theologis AA , Iyer S , Lenke LG , et al. Cervical and cervicothoracic sagittal alignment according to Roussouly thoracolumbar subtypes[J]. Spine (Phila Pa 1976), 2019, 44 (11): E634- E639.
doi: 10.1097/BRS.0000000000002941 |
| 7 |
Pepke W , Almansour H , Lafage R , et al. Cervical spine alignment following surgery for adolescent idiopathic scoliosis (AIS): A pre-to-post analysis of 81 patients[J]. BMC Surg, 2019, 19 (1): 7.
doi: 10.1186/s12893-019-0471-2 |
| 8 |
Khalil N , Bizdikian AJ , Bakouny Z , et al. Cervical and postural strategies for maintaining horizontal gaze in asymptomatic adults[J]. Eur Spine J, 2018, 27 (11): 2700- 2709.
doi: 10.1007/s00586-018-5753-3 |
| 9 |
Yu M , Zhao WK , Li M , et al. Analysis of cervical and global spine alignment under Roussouly sagittal classification in Chinese cervical spondylotic patients and asymptomatic subjects[J]. Eur Spine J, 2015, 24 (6): 1265- 1273.
doi: 10.1007/s00586-015-3832-2 |
| 10 |
Hardacker JW , Shuford RF , Capicotto PN , et al. Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms[J]. Spine (Phila Pa 1976), 1997, 22 (13): 1472- 1480.
doi: 10.1097/00007632-199707010-00009 |
| 11 |
Ohara A , Miyamoto K , Naganawa T , et al. Reliabilities of and correlations among five standard methods of assessing the sagittal alignment of the cervical spine[J]. Spine (Phila Pa 1976), 2006, 31 (22): 2585.
doi: 10.1097/01.brs.0000240656.79060.18 |
| 12 |
Roussouly P , Gollogly S , Berthonnaud E , et al. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position[J]. Spine (Phila Pa 1976), 2005, 30 (3): 346- 353.
doi: 10.1097/01.brs.0000152379.54463.65 |
| 13 |
Diebo BG , Challier V , Henry JK , et al. Predicting cervical alignment required to maintain horizontal gaze based on global spinal alignment[J]. Spine (Phila Pa 1976), 2016, 41 (23): 1795- 1800.
doi: 10.1097/BRS.0000000000001698 |
| 14 | Patwardhan AG , Khayatzadeh S , Havey RM , et al. Cervical sagittal balance: a biomechanical perspective can help clinical practice[J]. Eur Spine J, 2018, 27 (Suppl 1): 25- 38. |
| 15 |
Nori S , Shiraishi T , Aoyama R , et al. Upper cervical lordosis compensates lower cervical kyphosis to maintain whole cervical lordosis after selective laminectomy[J]. J Clin Neurosci, 2018, 58, 64- 69.
doi: 10.1016/j.jocn.2018.10.049 |
| 16 |
Kim JT , Lee HJ , Choi DY , et al. Sequential alignment change of the cervical spine after anterior cervical discectomy and fusion in the lower cervical spine[J]. Eur Spine J, 2016, 25 (7): 2223- 2232.
doi: 10.1007/s00586-016-4401-z |
| 17 |
Kim JH , Park JY , Yi S , et al. Anterior cervical discectomy and fusion alters whole-spine sagittal alignment[J]. Yonsei Med J, 2015, 56 (4): 1060- 1070.
doi: 10.3349/ymj.2015.56.4.1060 |
| 18 |
Tang R , Ye IB , Cheung ZB , et al. Age-related changes in cervical sagittal alignment: A radiographic analysis[J]. Spine (Phila Pa 1976), 2019, 44 (19): E1144- E1150.
doi: 10.1097/BRS.0000000000003082 |
| 19 |
Iyer S , Lenke LG , Nemani VM , et al. Variations in occipitocervical and cervicothoracic alignment parameters based on age: A prospective study of asymptomatic volunteers using full-body radiographs[J]. Spine (Phila Pa 1976), 2016, 41 (23): 1837- 1844.
doi: 10.1097/BRS.0000000000001644 |
| 20 |
Yang BS , Lee SK , Song KS , et al. The use of T1 sagittal angle in predicting cervical disc degeneration[J]. Asian Spine J, 2015, 9 (5): 757- 761.
doi: 10.4184/asj.2015.9.5.757 |
| 21 |
Mac-Thiong JM , Roussouly P , Berthonnaud E , et al. Sagittal parameters of global spinal balance: normative values from a prospective cohort of seven hundred nine Caucasian asymptomatic adults[J]. Spine (Phila Pa 1976), 2010, 35 (22): E1193- E1198.
doi: 10.1097/BRS.0b013e3181e50808 |
| 22 |
Lee CS , Chung SS , Kang KC , et al. Normal patterns of sagittal alignment of the spine in young adults radiological analysis in a Korean population[J]. Spine (Phila Pa 1976), 2011, 36 (25): E1648- E1654.
doi: 10.1097/BRS.0b013e318216b0fd |
| 23 | Zhu Z , Xu L , Zhu F , et al. Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations[J]. Spine (Phila Pa 1976), 2014, 39 (1): E1- E6. |
| 24 | Gutman G , Labelle H , Barchi S , et al. Normal sagittal parameters of global spinal balance in children and adolescents: A prospective study of 646 asymptomatic subjects[J]. Eur Spine J, 2016, 25 (11): 3650- 3657. |
| [1] | 田杨, 韩永正, 李娇, 王明亚, 曲音音, 房景超, 金辉, 李民, 王军, 徐懋, 王圣林, 郭向阳. 颈椎前路手术后硬膜外血肿的发生率和危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1058-1064. |
| [2] | 林国中,马长城,吴超,司雨,杨军. 微通道技术在颈椎管肿瘤微创切除术中的应用[J]. 北京大学学报(医学版), 2024, 56(2): 318-321. |
| [3] | 胡攀攀,李彦,刘啸,唐彦超,李梓赫,刘忠军. 自稳式人工椎体在颈椎前路手术中的应用[J]. 北京大学学报(医学版), 2024, 56(1): 161-166. |
| [4] | 周华,王仁吉,刘忠军,刘晓光,吴奉梁,党礌,韦峰. 3D打印人工椎体在颈椎脊索瘤全脊椎切除术中的应用[J]. 北京大学学报(医学版), 2023, 55(1): 144-148. |
| [5] | 张璐,胡小红,陈澄,蔡月明,王庆文,赵金霞. 类风湿关节炎初治患者颈椎失稳情况及临床特征[J]. 北京大学学报(医学版), 2021, 53(6): 1049-1054. |
| [6] | 林国中, 马长城, 王振宇, 谢京城, 刘彬, 陈晓东. 颈1~2硬膜外神经鞘瘤的显微微创治疗[J]. 北京大学学报(医学版), 2021, 53(3): 586-589. |
| [7] | 张璐,胡小红,王庆文,蔡月明,赵金霞,刘湘源. 类风湿关节炎合并颈椎失稳的人群分布及临床特征[J]. 北京大学学报(医学版), 2020, 52(6): 1034-1039. |
| [8] | 韩永正,井凤云,徐懋,郭向阳. 颈椎脊索瘤行肿瘤切除术的麻醉管理1例[J]. 北京大学学报(医学版), 2019, 51(5): 981-983. |
| [9] | 洪洪,钱宇婷,付磊,王武,李成辉,尹毅青. 困难气道中运用CT 三维重建技术指导硬质纤维气管镜行气管插管[J]. 北京大学学报(医学版), 2019, 51(5): 870-874. |
| [10] | 吴超,王振宇,林国中,于涛,刘彬,司雨,张一博,李元超. 单侧半椎板及不同程度小关节切除术对羊颈椎生物力学的影响[J]. 北京大学学报(医学版), 2019, 51(4): 728-732. |
| [11] | 杨泽川,刘朝旭,林阳,胡伟华,陈文坚,李锋,曾恒. 颈后路单开门椎管扩大成形术全钛板与交替钛板、缝线固定治疗颈椎病的对比研究[J]. 北京大学学报(医学版), 2019, 51(1): 187-193. |
| [12] | 李彦,姜亮,刘忠军,刘晓光,韦峰,于淼,陶立元. 超声骨刀在颈椎后路单开门椎管扩大成形术中应用的安全性和有效性[J]. 北京大学学报(医学版), 2018, 50(6): 1092-1097. |
| [13] | 刘洪,越雷,陈顺伦,胡博,李淳德△,邑晓东,李宏,卢海霖,王宇,于峥嵘,孙浩林,. 前路椎间盘切除椎间融合术治疗伴有交感神经症状的颈椎病[J]. 北京大学学报(医学版), 2018, 50(2): 347-351. |
| [14] | 安岩,田伟,曾成,李加宁,刘亚军. 以斜坡枢椎角评价上颈椎畸形患者术中脊髓压迫解除情况的可行性研究[J]. 北京大学学报(医学版), 2016, 48(2): 215-217. |
| [15] | 周华,孙宇,王少波,张凤山,张立,潘胜发,周非非. 椎管扩大成形术后颈椎后纵韧带骨化进展的再手术治疗[J]. 北京大学学报(医学版), 2016, 48(2): 210-214. |
|
||
