北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (5): 818-824. doi: 10.19723/j.issn.1671-167X.2023.05.007
基于MRI前列腺腺体相关参数构建腹腔镜前列腺癌术后尿失禁的预测模型
毛海1,2,张帆1,张展奕1,颜野1,郝一昌1,黄毅1,*( ),马潞林1,褚红玲3,*(),张树栋1
),马潞林1,褚红玲3,*(),张树栋1
- 1. 北京大学第三医院泌尿外科, 北京 100191
2. 重庆市奉节县中医院泌尿外科, 重庆奉节 404600
3. 北京大学第三医院临床流行病学研究中心, 北京 100191
Predictive model of early urinary continence recovery based on prostate gland MRI parameters after laparoscopic radical prostatectomy
Hai MAO1,2,Fan ZHANG1,Zhan-yi ZHANG1,Ye YAN1,Yi-chang HAO1,Yi HUANG1,*(),Lu-lin MA1,Hong-ling CHU3,*(),Shu-dong ZHANG1
- 1. Department of Urology, Peking University Third Hospital, Beijing 100191, China
2. Department of Urology, Traditional Chinese Medicine Hospital of Fengjie, Fengjie 404600, Chongqing, China
3. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing 100191, China
摘要:
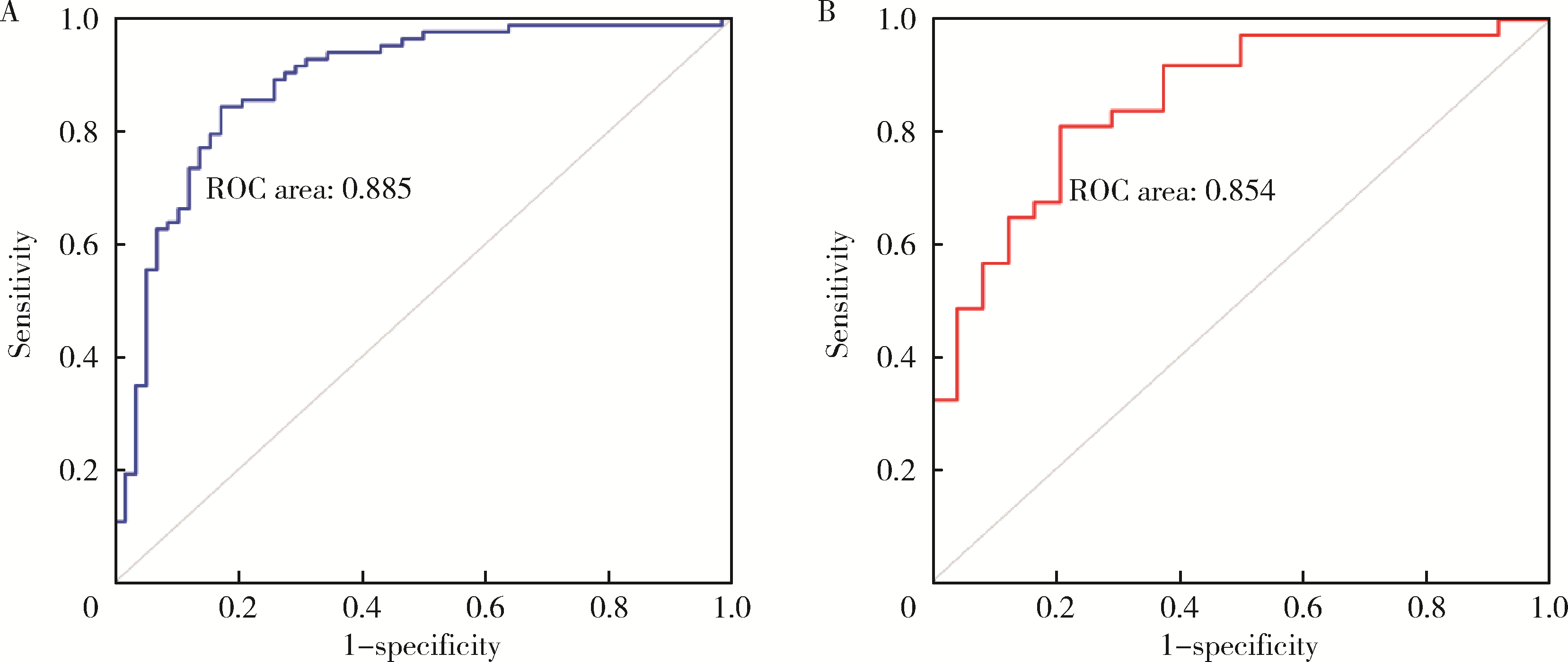
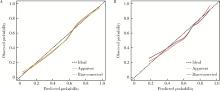
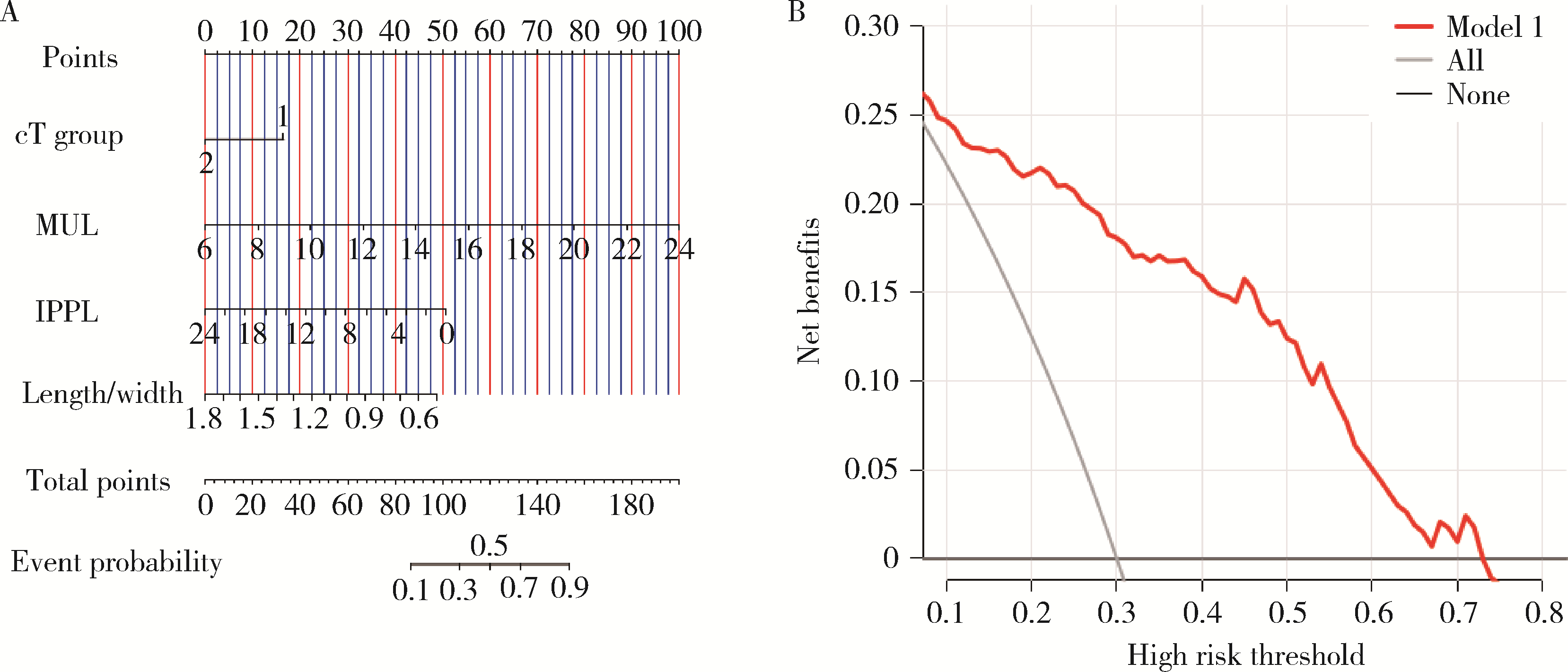
目的: 评估基于MRI前列腺腺体相关参数构建的列线图预测腹腔镜前列腺癌术后尿失禁的临床价值。方法: 纳入经前列腺穿刺活检诊断为前列腺腺癌并于北京大学第三医院行腹腔镜根治性前列腺切除术(laparo-scopic radical prostatectomy,LRP)的202例患者,所有患者的术前MRI检查于前列腺穿刺活检术前1周内完成,腺体相关参数包含前列腺上下径、左右径、前后径、前列腺体积、前列腺尖部突入深度(intravesical prostatic protrusion length,IPPL)、前列腺尖部形态分型等。自术后第1个月起,每个月对患者的控尿功能恢复情况进行随访,以全天不需要使用尿垫作为控尿功能恢复标准。应用Logistic多因素回归分析影响术后早期控尿功能恢复的危险因素,绘制各模型预测术后控尿功能恢复的受试者操作特征(receiver operator characteristic,ROC)曲线,以DeLong检验比较曲线下面积的差异,以决策曲线分析评价模型的临床净获益。结果: 202例患者的平均年龄为69.0(64.0, 75.5)岁,穿刺前平均前列腺特异性抗原(prostate specific antigen,PSA)为12.12 (7.36, 20.06) μg/L,穿刺Gleason评分 < 7分和≥7分者分别为73例(36.2%)和129例(63.9%),临床分期为T1/T2期者100例(49.5%),T3期者102例(50.5%)。经术前MRI测量,前列腺体积为35.4 (26.2, 51.1) mL,前列腺上下径与左右径的比值为0.91 (0.77, 1.07),膜性尿道长度为15 (11, 16) mm,IPPL为2 (0, 6) mm,前列腺尖部形态分型A~D型分别为67例(33.2%)、80例(39.6%)、24例(11.9%)和31例(15.3%),训练集和验证集分别为141例和61例。所有患者手术均顺利完成,随访3个月患者的控尿率为59.4%(120/202例)。训练集多因素分析结果显示,膜性尿道长度(P < 0.001)、IPPL(P=0.017)和临床分期(P=0.022)是术后早期(3个月)尿失禁发生的独立危险因素。根据多因素分析结果制作列线图和临床决策曲线,计算训练集ROC曲线下面积为0.885 (0.826, 0.944),计算验证集ROC曲线下面积为0.854 (0.757, 0.950)。在验证集里对模型进行Hosmer-Lemeshow拟合优度检验,卡方值为5.426 (P=0.711)。结论: 术前膜性尿道长度、IPPL、临床分期是LRP术后早期尿失禁发生的独立危险因素,基于MRI前列腺腺体相关参数构建的列线图可有效预测LRP术后早期控尿功能恢复,但此结果还需更大规模的临床研究证实。
中图分类号:
- R737.25

| 1 |
Mottet N , van den Bergh RCN , Briers E , et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. Part 1: Screening, diagnosis, and local treatment with curative intent[J]. Eur Urol, 2021, 79 (2): 243- 262.
doi: 10.1016/j.eururo.2020.09.042 |
| 2 |
Ficarra V , Novara G , Rosen RC , et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy[J]. Eur Urol, 2012, 62 (3): 405- 417.
doi: 10.1016/j.eururo.2012.05.045 |
| 3 |
Adam M , Tennstedt P , Lanwehr D , et al. Functional outcomes and quality of life after radical prostatectomy only versus a combination of prostatectomy with radiation and hormonal therapy[J]. Eur Urol, 2017, 71 (3): 330- 336.
doi: 10.1016/j.eururo.2016.11.015 |
| 4 |
Heesakkers J , Farag F , Bauer RM , et al. Pathophysiology and contributing factors in postprostatectomy incontinence: A review[J]. Eur Urol, 2017, 71 (6): 936- 944.
doi: 10.1016/j.eururo.2016.09.031 |
| 5 |
Lamberg H , Shankar PR , Singh K , et al. Preoperative prostate MRI predictors of urinary continence following radical prostatectomy[J]. Radiology, 2022, 303 (1): 99- 109.
doi: 10.1148/radiol.210500 |
| 6 |
van Dijk-de Haan MC , Boellaard TN , Tissier R , et al. Value of different magnetic resonance imaging-based measurements of anatomical structures on preoperative prostate imaging in predicting urinary continence after radical prostatectomy in men with prostate cancer: A systematic review and meta-analysis[J]. Eur Urol Focus, 2022, 8 (5): 1211- 1225.
doi: 10.1016/j.euf.2022.01.015 |
| 7 |
Mungovan SF , Sandhu JS , Akin O , et al. Preoperative membranous urethral length measurement and continence recovery following radical prostatectomy: A systematic review and meta-analysis[J]. Eur Urol, 2017, 71 (3): 368- 378.
doi: 10.1016/j.eururo.2016.06.023 |
| 8 |
Manfredi M , Checcucci E , Fiori C , et al. Total anatomical reconstruction during robot-assisted radical prostatectomy: Focus on urinary continence recovery and related complications after 1 000 procedures[J]. BJU Int, 2019, 124 (3): 477- 486.
doi: 10.1111/bju.14716 |
| 9 |
Matsushita K , Kent MT , Vickers AJ , et al. Preoperative predictive model of recovery of urinary continence after radical prostatectomy[J]. BJU Int, 2015, 116 (4): 577- 583.
doi: 10.1111/bju.13087 |
| 10 |
Tutolo M , Bruyneel L , van der Aa F , et al. A novel tool to predict functional outcomes after robot-assisted radical prostatectomy and the value of additional surgery for incontinence[J]. BJU Int, 2021, 127 (5): 575- 584.
doi: 10.1111/bju.15242 |
| 11 |
Lee SE , Byun SS , Lee HJ , et al. Impact of variations in prostatic apex shape on early recovery of urinary continence after radical retropubic prostatectomy[J]. Urology, 2006, 68 (1): 137- 141.
doi: 10.1016/j.urology.2006.01.021 |
| 12 |
Walz J , Epstein JI , Ganzer R , et al. A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy: An update[J]. Eur Urol, 2016, 70 (2): 301- 311.
doi: 10.1016/j.eururo.2016.01.026 |
| 13 | Zhang F , Chu H , Hao Y , et al. Preoperative predictive model of early urinary continence recovery after laparoscopic radical prostatectomy[J]. World J Urol, 2023, 41 (1): 59- 65. |
| 14 |
Kadono Y , Nohara T , Kawaguchi S , et al. Investigating the me-chanism underlying urinary continence recovery after radical prostatectomy: Effectiveness of a longer urethral stump to prevent urinary incontinence[J]. BJU Int, 2018, 122 (3): 456- 462.
doi: 10.1111/bju.14181 |
| 15 |
Nunez Bragayrac LA , Hussein AA , Attwood K , et al. Feasibility and continence outcomes of extended prostatic urethral preservation during robot-assisted radical prostatectomy[J]. Prostate Cancer Prostatic Dis, 2020, 23 (2): 286- 294.
doi: 10.1038/s41391-019-0173-y |
| 16 |
Huang AC , Kowalczyk KJ , Hevelone ND , et al. The impact of prostate size, median lobe, and prior benign prostatic hyperplasia intervention on robot-assisted laparoscopic prostatectomy: Technique and outcomes[J]. Eur Urol, 2011, 59 (4): 595- 603.
doi: 10.1016/j.eururo.2011.01.033 |
| 17 |
Jo JK , Hong SK , Byun SS , et al. Urinary Continence after robot-assisted laparoscopic radical prostatectomy: The impact of intrave-sical prostatic protrusion[J]. Yonsei Med J, 2016, 57 (5): 1145- 1151.
doi: 10.3349/ymj.2016.57.5.1145 |
| 18 |
Hoeh B , Wenzel M , Müller M , et al. Urethral sphincter length but not prostatic apex shape in preoperative MRI is associated with mid-term continence rates after radical prostatectomy[J]. Diagnostics (Basel), 2022, 12 (3): 701.
doi: 10.3390/diagnostics12030701 |
| [1] | 王楠楠, 袁大晋, 朱昱冰, 丁磊. 结直肠癌根治术后肝转移风险多中心列线图预测模型的构建与验证[J]. 北京大学学报(医学版), 2026, 58(2): 290-300. |
| [2] | 刘艳华, 陆敏, 赵旭阳, 张宽根, 武睿, 梅放, 戴志豪, 由江峰, 裴斐. 肿瘤转移抑制基因LASS2去磷酸化对液泡型ATP酶活性及前列腺癌侵袭性的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1113-1123. |
| [3] | 李浙民, 季加孚, 李国新, 李子禹, 步召德, 高翔宇, 董迪, 唐磊, 邢晓芳, 贾淑芹, 郭婷, 张连海, 陕飞, 季鑫, 王安强. 胃癌精准诊疗技术的创建与推广[J]. 北京大学学报(医学版), 2025, 57(5): 864-867. |
| [4] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [5] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [6] | 宁家昕, 王浩然, 罗书航, 敬吉波, 王建业, 侯惠民, 刘明. 氧化应激相关基因与前列腺癌关系的多组学分析[J]. 北京大学学报(医学版), 2025, 57(4): 633-643. |
| [7] | 王泽远, 于栓宝, 郑浩轲, 陶金, 范雅峰, 张雪培. 基于临床特征和多参数MRI的前列腺癌盆腔淋巴结转移的术前预测模型[J]. 北京大学学报(医学版), 2025, 57(4): 684-691. |
| [8] | 张铃福, 王港, 侯纯升, 崔龙, 王立新, 凌晓锋, 徐智. 腹腔镜下改良经胆囊管胆管引流术在胆石症治疗及胆道疾病诊断中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 748-752. |
| [9] | 黄万伟, 沙显燊, 张艺宝, 伍国豪, 骆峰, 陈智慧, 叶东明, 李学松, 赖彩永. 完全3D腹腔镜回肠代双侧输尿管联合膀胱扩大术修复放射治疗后双侧输尿管狭窄并膀胱挛缩[J]. 北京大学学报(医学版), 2025, 57(4): 789-795. |
| [10] | 刘园梅, 傅义程, 郝靖欣, 张福春, 刘慧琳. 老年髋部骨折患者住院期间发生术后心力衰竭的列线图预测模型的构建及验证[J]. 北京大学学报(医学版), 2024, 56(5): 874-883. |
| [11] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [12] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [13] | 田宇轩,阮明健,刘毅,李德润,吴静云,沈棋,范宇,金杰. 双参数MRI改良PI-RADS评分4分和5分病灶的最大径对临床有意义前列腺癌的预测效果[J]. 北京大学学报(医学版), 2024, 56(4): 567-574. |
| [14] | 姚凯烽,阮明健,李德润,田宇轩,陈宇珂,范宇,刘毅. 靶向穿刺联合区域系统穿刺对PI-RADS 4~5分患者的前列腺癌诊断效能[J]. 北京大学学报(医学版), 2024, 56(4): 575-581. |
| [15] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
|
||
