北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (2): 299-306. doi: 10.19723/j.issn.1671-167X.2024.02.015
胫距跟融合治疗终末期踝和后足病变的中短期临床结果
李文菁,张保宙,李恒,赖良鹏,杜辉,孙宁,龚晓峰,李莹*( ),王岩,武勇
),王岩,武勇
- 首都医科大学附属北京积水潭医院足踝外科, 北京 100035
Tibiotalocalcaneal arthrodesis for end-stage ankle and hindfoot arthropathy: Short- and mid-term clinical outcomes
Wenjing LI,Baozhou ZHANG,Heng LI,Liangpeng LAI,Hui DU,Ning SUN,Xiaofeng GONG,Ying LI*(),Yan WANG,Yong WU
- Department of Foot and Ankle Surgery, Beijing Jishuitan Hospital, Capital Medical University, Beijing 100035, China
摘要:
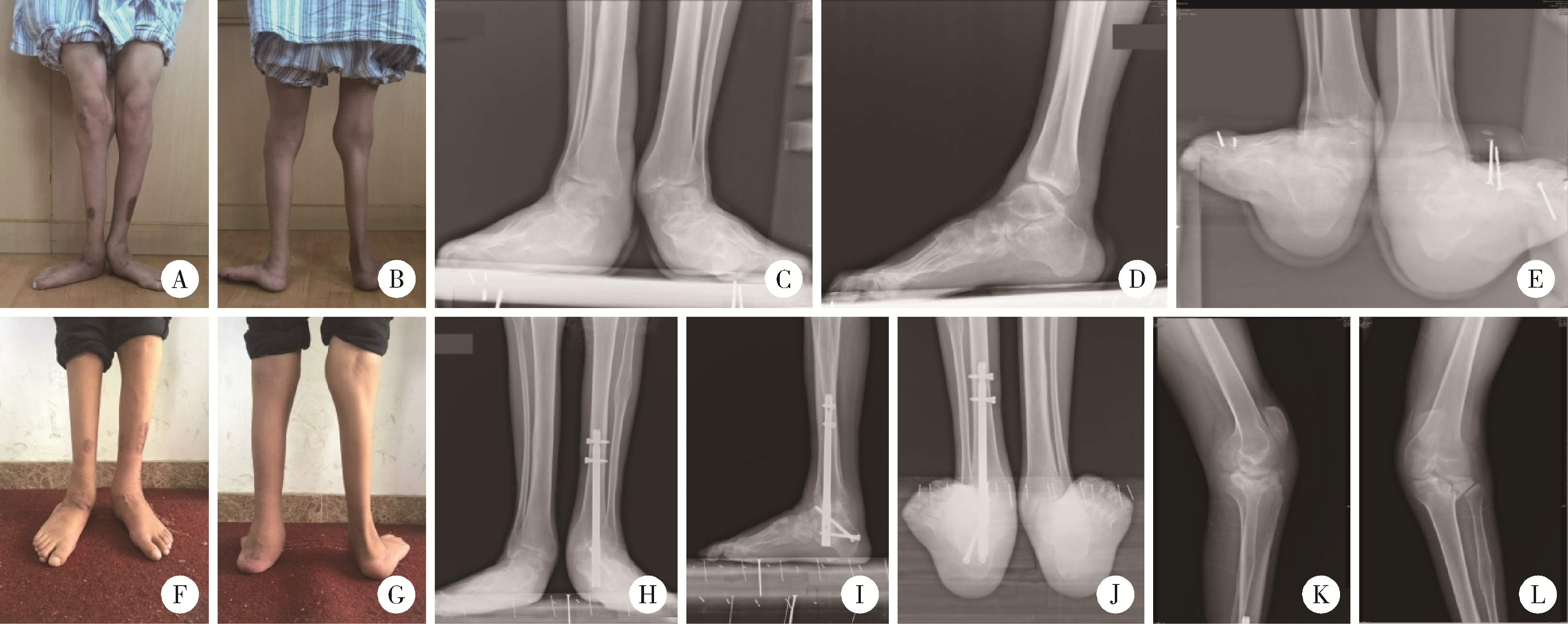
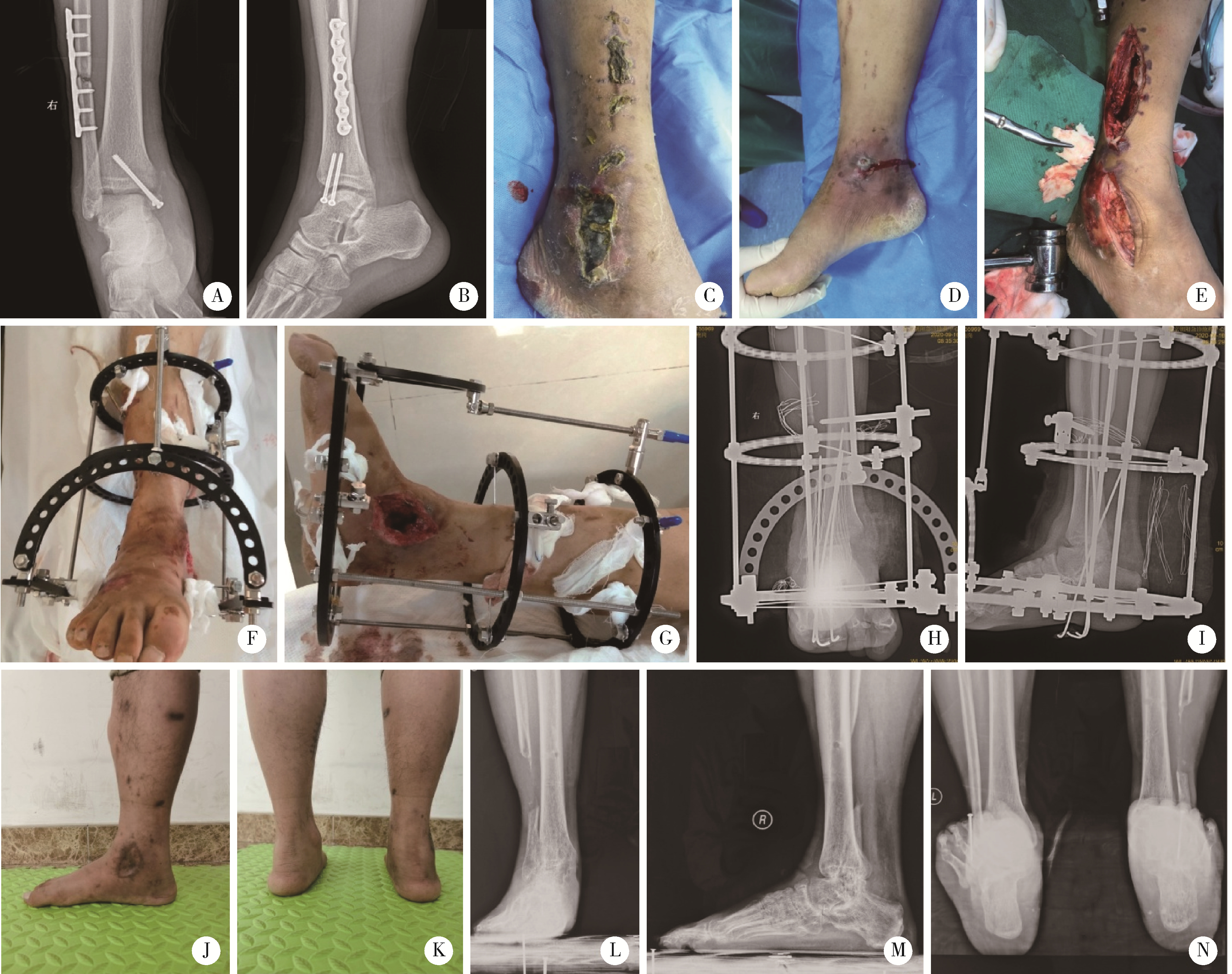
目的: 分析同一术者行胫距跟(tibiotalocalcaneal, TTC)融合手术的患者临床资料,探讨患者临床结果、并发症和功能改善情况,分析TTC融合手术的临床预后及注意事项。方法: 回顾性分析2011年3月至2020年12月由同一术者行TTC融合手术治疗的40例患者的临床资料,其中男23例,女17例,平均年龄(49.1±16.0)岁,均为单侧手术。记录患者一般临床特征、影像学表现、主要诊断、具体手术方式。对比术前及末次随访时患者的美国足踝外科协会(American Orthopaedic Foot and Ankle Society, AOFAS)踝-后足评分、疼痛视觉模拟评分(visual analogue scale,VAS),记录融合愈合时间、症状较术前改善情况(明显改善、部分改善、无改善或恶化)以及术后并发症的发生情况。结果: 患者的术后中位随访时间为38.0(26.3, 58.8)个月;术前中位VAS评分为6.0(4.0, 7.0)分,中位AOFAS评分为33.0(25.3, 47.3)分;末次随访时患者的中位VAS评分为0(0, 3.0)分,中位AOFAS评分为80.0(59.0, 84.0)分;均较术前明显改善(P < 0.05)。所有患者均无切口坏死及感染,1例发生距下关节不愈合,为梅毒夏科氏(Charcot)关节,其余患者中位骨愈合时间为15.0(12.0, 20.0)周。所有患者中,较术前有明显改善者25例,部分改善者8例,改善不明显者4例,症状较术前加重者3例。结论: TTC融合术是治疗后足终末期病变的可靠方法,多数患者术后功能有改善,日常生活影响不大,预后差的原因包括足趾僵硬、邻近膝关节应力集中、不愈合及不明原因疼痛等。
中图分类号:
- R687.4






| 1 |
Brage ME , Mathews CS . Ankle and tibiotalocalcaneal fusion[J]. Foot Ankle Clin, 2022, 27 (2): 343- 353.
doi: 10.1016/j.fcl.2021.11.020 |
| 2 |
Stołtny T , Dugiełło B , Pasek J , et al. Tibiotalocalcaneal arthrodesis in osteoarthritis deformation of ankle and subtalar joint: Evaluation of treatment results[J]. J Foot Ankle Surg, 2022, 61 (1): 205- 211.
doi: 10.1053/j.jfas.2021.09.005 |
| 3 |
Yao Y , Mo Z , Wu G , et al. A personalized 3D-printed plate for tibiotalocalcaneal arthrodesis: Design, fabrication, biomechanical evaluation and postoperative assessment[J]. Comput Biol Med, 2021, 133, 104368.
doi: 10.1016/j.compbiomed.2021.104368 |
| 4 |
Perez-Aznar A , Gonzalez-Navarro B , Bello-Tejeda LL , et al. Tibiotalocalcaneal arthrodesis with a retrograde intramedullary nail: A prospective cohort study at a minimum five year follow-up[J]. Int Orthop, 2021, 45 (9): 2299- 2305.
doi: 10.1007/s00264-020-04904-3 |
| 5 |
Pitts C , Alexander B , Washington J , et al. Factors affecting the outcomes of tibiotalocalcaneal fusion[J]. Bone Joint J, 2020, 102-B (3): 345- 351.
doi: 10.1302/0301-620X.102B3.BJJ-2019-1325.R1 |
| 6 |
Kitaoka HB , Alexander IJ , Adelaar RS , et al. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes[J]. Foot Ankle Int, 1994, 15 (7): 349- 353.
doi: 10.1177/107110079401500701 |
| 7 |
Reed MD , van Nostran W . Assessing pain intensity with the visual analog scale: A plea for uniformity[J]. J Clin Pharmacol, 2014, 54 (3): 241- 244.
doi: 10.1002/jcph.250 |
| 8 |
Martínez-de-Albornoz P , Monteagudo M . Tibiotalocalcaneal arthrodesis in severe hindfoot deformities[J]. Foot Ankle Clin, 2022, 27 (4): 847- 866.
doi: 10.1016/j.fcl.2022.08.008 |
| 9 |
Burns PR , Dunse A . Tibiotalocalcaneal arthrodesis for foot and ankle deformities[J]. Clin Podiatr Med Surg, 2017, 34 (3): 357- 380.
doi: 10.1016/j.cpm.2017.02.007 |
| 10 |
Monteagudo M , Martínez-de-Albornoz P . Deciding between ankle and tibiotalocalcaneal arthrodesis for isolated ankle arthritis[J]. Foot Ankle Clin, 2022, 27 (1): 217- 231.
doi: 10.1016/j.fcl.2021.11.012 |
| 11 |
Rana B , Patel S . Results of ankle and hind foot arthrodesis in diabetic Charcot neuroarthropathy: A retrospective analysis of 44 patients[J]. J Clin Orthop Trauma, 2021, 23, 101637.
doi: 10.1016/j.jcot.2021.101637 |
| 12 |
Chraim M , Krenn S , Alrabai HM , et al. Mid-term follow-up of patients with hindfoot arthrodesis with retrograde compression intramedullary nail in Charcot neuroarthropathy of the hindfoot[J]. Bone Joint J, 2018, 100-B (2): 190- 196.
doi: 10.1302/0301-620X.100B2.BJJ-2017-0374.R2 |
| 13 |
Kollig E , Esenwein SA , Muhr G , et al. Fusion of the septic ankle: Experience with 15 cases using hybrid external fixation[J]. J Trauma, 2003, 55 (4): 685- 691.
doi: 10.1097/01.TA.0000051933.83342.E4 |
| 14 |
Hartmann R , Grubhofer F , Waibel FWA , et al. Treatment of hindfoot and ankle infections with Ilizarov external fixator or spacer, followed by secondary arthrodesis[J]. J Orthop Res, 2021, 39 (10): 2151- 2158.
doi: 10.1002/jor.24938 |
| 15 |
Baumbach SF , Massen FK , Hörterer S , et al. Comparison of arthroscopic to open tibiotalocalcaneal arthrodesis in high-risk patients[J]. Foot Ankle Surg, 2019, 25 (6): 804- 811.
doi: 10.1016/j.fas.2018.10.006 |
| 16 |
Rausch S , Loracher C , Fröber R , et al. Anatomical evaluation of different approaches for tibiotalocalcaneal arthrodesis[J]. Foot Ankle Int, 2014, 35 (2): 163- 167.
doi: 10.1177/1071100713517095 |
| 17 |
Wu M , Scott D , Abar B , et al. Does a fibula-sparing approach improve outcomes in tibiotalocalcaneal arthrodesis?[J]. Foot Ankle Surg, 2023, 29 (1): 90- 96.
doi: 10.1016/j.fas.2022.11.001 |
| 18 |
Carranza-Bencano A , Tejero S , Del CG , et al. Minimal incision surgery for tibiotalocalcaneal arthrodesis[J]. Foot Ankle Int, 2014, 35 (3): 272- 284.
doi: 10.1177/1071100713515447 |
| 19 |
Pellegrini MJ , Schiff AP , Adams SJ , et al. Outcomes of tibiotalocalcaneal arthrodesis through a posterior Achilles tendon-splitting approach[J]. Foot Ankle Int, 2016, 37 (3): 312- 319.
doi: 10.1177/1071100715615398 |
| 20 |
Eckholt S , Garcia-Elvira R , Fontecilla N , et al. Role of extra-articular tibiotalocalcaneal arthrodesis and posterior approach in highly complex cases[J]. Foot Ankle Int, 2018, 39 (2): 219- 225.
doi: 10.1177/1071100717737973 |
| 21 |
Gong J , Zhou B , Tao X , et al. Tibiotalocalcaneal arthrodesis with headless compression screws[J]. J Orthop Surg Res, 2016, 11 (1): 91.
doi: 10.1186/s13018-016-0425-7 |
| 22 |
Gutteck N , Schilde S , Reichel M , et al. Posterolateral plate fixation with Pantalarlock® is more stable than nail fixation in tibiotalocalcaneal arthrodesis in a biomechanical cadaver study[J]. Foot Ankle Surg, 2020, 26 (3): 328- 333.
doi: 10.1016/j.fas.2019.04.006 |
| 23 |
Richman J , Cota A , Weinfeld S . Intramedullary nailing and external ring fixation for tibiotalocalcaneal arthrodesis in Charcot arthropathy[J]. Foot Ankle Int, 2017, 38 (2): 149- 152.
doi: 10.1177/1071100716671884 |
| [1] | 李伟浩, 张学民, 李伟, 张韬, 张小明. 胸主动脉腔内修复术左肱动脉穿刺点使用血管缝合器处理的临床效果[J]. 北京大学学报(医学版), 2026, 58(2): 388-392. |
| [2] | FarinEbrahimi, 冯志强, FarazEbrahimi, 韩玮华, 于子杨, 贾宽宽, 安金刚. 上颌药物相关性颌骨坏死的不同分期手术治疗效果[J]. 北京大学学报(医学版), 2026, 58(1): 107-114. |
| [3] | 潘莲菲, 李文静, 王瑞洋, 焦剑, 曹战强, 高丽, 释栋. 口服抗生素辅助牙周机械治疗对重度牙周炎的短期疗效及影响因素[J]. 北京大学学报(医学版), 2026, 58(1): 30-36. |
| [4] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [5] | 康一帆, 葛严军, 吕晓鸣, 谢尚, 单小峰, 蔡志刚. 即刻种植体支持式义齿修复的血管化髂骨瓣重建下颌骨缺损[J]. 北京大学学报(医学版), 2025, 57(1): 78-84. |
| [6] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
| [7] | 薛蔚,董樑,钱宏阳,费笑晨. 前列腺癌新辅助治疗与辅助治疗的现状及进展[J]. 北京大学学报(医学版), 2023, 55(5): 775-780. |
| [8] | 邱敏,宗有龙,王滨帅,杨斌,徐楚潇,孙争辉,陆敏,赵磊,卢剑,刘承,田晓军,马潞林. 腹腔镜肾部分切除术治疗中高复杂程度肾肿瘤的效果[J]. 北京大学学报(医学版), 2023, 55(5): 833-837. |
| [9] | 王磊,韩天栋,江卫星,李钧,张道新,田野. 主动迁移技术与原位碎石技术在输尿管软镜治疗1~2 cm输尿管上段结石中的安全性和有效性比较[J]. 北京大学学报(医学版), 2023, 55(3): 553-557. |
| [10] | 熊士凯,史尉利,王安鸿,谢兴,郭秦炜. 腓骨远端撕脱骨折的影像学诊断:踝关节X线与CT三维重建的比较[J]. 北京大学学报(医学版), 2023, 55(1): 156-159. |
| [11] | 李伟浩,李伟,张学民,李清乐,焦洋,张韬,蒋京军,张小明. 去分支杂交手术和传统手术治疗胸腹主动脉瘤的结果比较[J]. 北京大学学报(医学版), 2022, 54(1): 177-181. |
| [12] | 邓雪蓉,孙晓莹,张卓莉. 类风湿关节炎患者足踝部体征和超声下病变的一致性[J]. 北京大学学报(医学版), 2021, 53(6): 1037-1042. |
| [13] | 敖明昕,李学民,于媛媛,时会娟,黄红拾,敖英芳,王薇. 视觉重建对老年人行走动态足底压力的影响[J]. 北京大学学报(医学版), 2021, 53(5): 907-914. |
| [14] | 朱正达,高岩,何汶秀,方鑫,刘洋,魏攀,闫志敏,华红. 红色诺卡氏菌细胞壁骨架治疗糜烂型口腔扁平苔藓的疗效及安全性[J]. 北京大学学报(医学版), 2021, 53(5): 964-969. |
| [15] | 刘立立,刘志科,张良,李宁,方挺,张栋梁,许国章,詹思延. 2016—2019年宁波市5岁及以下儿童手足口病流行病学特征[J]. 北京大学学报(医学版), 2021, 53(3): 491-497. |
|
||
