北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (1): 177-181. doi: 10.19723/j.issn.1671-167X.2022.01.028
去分支杂交手术和传统手术治疗胸腹主动脉瘤的结果比较
李伟浩,李伟( ),张学民,李清乐,焦洋,张韬,蒋京军,张小明
),张学民,李清乐,焦洋,张韬,蒋京军,张小明
- 北京大学人民医院血管外科,北京 100044
Comparison of the outcomes between open and hybrid approaches in the treatment of thoracoabdominal aortic aneurysms repair
LI Wei-hao,LI Wei(),ZHANG Xue-min,LI Qing-le,JIAO Yang,ZHANG Tao,JIANG Jing-jun,ZHANG Xiao-ming
- Department of Vascular Surgery, Peking University People’s Hospital, Beijing 100044, China
摘要:
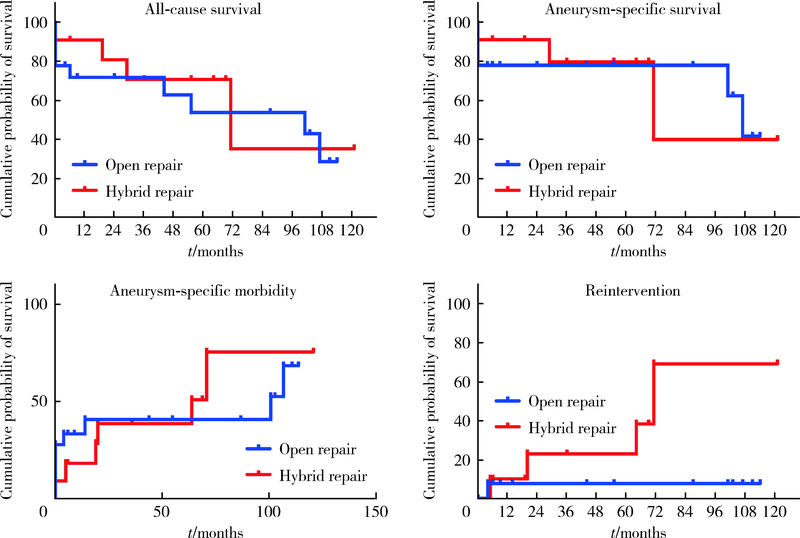
目的: 总结和对比去分支杂交手术和传统手术治疗胸腹主动脉瘤的近远期结果。方法: 回顾性分析2008年1月至2019年12月采用传统手术治疗胸腹主动脉瘤的18例患者和采用杂交手术治疗的11例患者的临床资料。杂交手术组中,夹层动脉瘤、术前合并肾功能不全以及美国麻醉医师协会(American Society of Anesthesiologists,ASA)评分≥3分的患者比例明显高于传统手术组。结果: 去分支杂交手术患者的手术时间为(445±85) min,术中出血量为(955±599) mL,术后30 d发生并发症2例,没有截瘫,死亡1例,术后30 d并发症发生率为18.2%,死亡率为9.1%。传统手术患者的手术时间为(560±245) min,术中出血量为(6 100±4 536) mL,术后30 d发生并发症12例,其中截瘫1例,死亡4例,术后30 d并发症发生率为66.7%,死亡率为22.2%。去分支杂交手术的术中出血量明显低于传统手术(P<0.001),30 d内并发症发生率显著降低(P=0.011)。随访期内,杂交手术组二次手术4例,死亡3例,1年、5年和10年的全因生存率分别为72%、54%和29%;传统手术组二次手术1例,死亡5例,1年、5年和10年的全因生存率分别为81%、71%和35%。杂交手术和传统手术在全因生存率和动脉瘤生存率上差异没有统计学意义。结论: 去分支杂交手术是一种治疗高危胸腹主动脉瘤患者安全、有效的手术方式,术后早期并发症发生率明显低于传统手术,但中远期疗效仍需要进一步提高。
中图分类号:
- R654.3
| [1] | 张小明, 张永保, 李清乐, 等. 胸腹主动脉瘤的治疗[J]. 中国血管外科杂志: 电子版, 2014, 6(3):137-142. |
| [2] | 来志超, 孙晓宁, 古丽丹娜·沙艳, 等. 胸腹主动脉瘤的手术方式与外科治疗选择[J]. 中国血管外科杂志: 电子版, 2018, 10(4):233-236. |
| [3] | 赵纪春, 陈熹阳. 胸腹主动脉瘤: 杂交手术现状[J]. 中华血管外科杂志, 2016, 1(2):78-81. |
| [4] |
Di Marco L, Murana G, Leone A, et al. Hybrid repair of thoracoabdominal aneurysm: An alternative strategy for preventing major complications in high risk patients[J]. Int J Cardiol, 2018, 271:31-35.
doi: S0167-5273(18)31046-5 pmid: 30223362 |
| [5] |
Jain A, Flohr TF, Johnston WF, et al. Staged hybrid repair of extensive thoracoabdominal aortic aneurysms secondary to chronic aortic dissection[J]. J Vasc Surg, 2016, 63(1):62-69.
doi: 10.1016/j.jvs.2015.08.060 |
| [6] | Coselli JS, Amarasekara HS, Zhang Q, et al. The impact of preoperative chronic kidney disease on outcomes after Crawford extent Ⅱ thoracoabdominal aortic aneurysm repairs[J]. J Thorac Cardiovasc Surg, 2018, 156(6): 2053-2064. e1. |
| [7] |
Girardi LN, Ohmes LB, Lau C, et al. Open repair of descending thoracic and thoracoabdominal aortic aneurysms in patients with preoperative renal failure[J]. Eur J Cardiothorac Surg, 2017, 51(5):971-977.
doi: 10.1093/ejcts/ezx007 |
| [8] |
Cina CS, Clase CM. Coagulation disorders and blood product use in patients undergoing thoracoabdominal aortic aneurysm repair[J]. Transfus Med Rev, 2005, 19(2):143-154.
doi: 10.1016/j.tmrv.2004.11.003 |
| [9] | 闫兵, 张雷, 黄骏咏, 等. 去分支技术治疗胸腹主动脉瘤[J]. 中华外科杂志, 2014, 52(7):536-538. |
| [10] |
Moulakakis KG, Mylonas SN, Avgerinos ED, et al. Hybrid open endovascular technique for aortic thoracoabdominal pathologies[J]. Circulation, 2011, 124(24):2670-2680.
doi: 10.1161/CIRCULATIONAHA.111.041582 |
| [11] | 张宏鹏, 郭伟, 刘小平, 等. 杂交技术治疗胸腹主动脉瘤[J]. 中华外科杂志, 2009, 47(9):657-660. |
| [1] | 李文菁,张保宙,李恒,赖良鹏,杜辉,孙宁,龚晓峰,李莹,王岩,武勇. 胫距跟融合治疗终末期踝和后足病变的中短期临床结果[J]. 北京大学学报(医学版), 2024, 56(2): 299-306. |
| [2] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
| [3] | 薛蔚,董樑,钱宏阳,费笑晨. 前列腺癌新辅助治疗与辅助治疗的现状及进展[J]. 北京大学学报(医学版), 2023, 55(5): 775-780. |
| [4] | 邱敏,宗有龙,王滨帅,杨斌,徐楚潇,孙争辉,陆敏,赵磊,卢剑,刘承,田晓军,马潞林. 腹腔镜肾部分切除术治疗中高复杂程度肾肿瘤的效果[J]. 北京大学学报(医学版), 2023, 55(5): 833-837. |
| [5] | 许素环,王蓓蓓,庞秋颖,钟丽君,丁炎明,黄燕波,车新艳. 等体温膀胱冲洗对经尿道前列腺电切术患者干预效果的meta分析[J]. 北京大学学报(医学版), 2023, 55(4): 676-683. |
| [6] | 王磊,韩天栋,江卫星,李钧,张道新,田野. 主动迁移技术与原位碎石技术在输尿管软镜治疗1~2 cm输尿管上段结石中的安全性和有效性比较[J]. 北京大学学报(医学版), 2023, 55(3): 553-557. |
| [7] | 李辉,高阳旭,王书磊,姚红新. 恶性肿瘤患儿完全植入式静脉输液港手术并发症[J]. 北京大学学报(医学版), 2022, 54(6): 1167-1171. |
| [8] | 朱正达,高岩,何汶秀,方鑫,刘洋,魏攀,闫志敏,华红. 红色诺卡氏菌细胞壁骨架治疗糜烂型口腔扁平苔藓的疗效及安全性[J]. 北京大学学报(医学版), 2021, 53(5): 964-969. |
| [9] | 董文敏,王明瑞,胡浩,王起,许克新,徐涛. Allium覆膜金属输尿管支架长期留置治疗输尿管-回肠吻合口狭窄的初期临床经验及随访结果[J]. 北京大学学报(医学版), 2020, 52(4): 637-641. |
| [10] | 高健,胡立宝,陈尘,郅新,徐涛. 经皮肾镜去石术后出血的介入治疗[J]. 北京大学学报(医学版), 2020, 52(4): 667-671. |
| [11] | 李潇,苏家增,张严妍,张丽琪,张亚琼,柳登高,俞光岩. 131I相关唾液腺炎的炎症分级及内镜治疗[J]. 北京大学学报(医学版), 2020, 52(3): 586-590. |
| [12] | 马凯,曲星珂,许清泉,熊六林,叶雄俊,安立哲,陈伟男,黄晓波. 肾移植术后移植肾输尿管膀胱吻合口狭窄的腔内治疗:13例报道[J]. 北京大学学报(医学版), 2019, 51(6): 1155-1158. |
| [13] | 詹颖,杜祎甜,仰浈臻,张春丽,齐宪荣. 紫杉醇微球-原位凝胶的制备及其局部注射的抗肿瘤药效[J]. 北京大学学报(医学版), 2019, 51(3): 477-486. |
| [14] | 杨泽川,刘朝旭,林阳,胡伟华,陈文坚,李锋,曾恒. 颈后路单开门椎管扩大成形术全钛板与交替钛板、缝线固定治疗颈椎病的对比研究[J]. 北京大学学报(医学版), 2019, 51(1): 187-193. |
| [15] | 游文喆,窦桂丽,夏斌. 乳牙间接牙髓治疗两年疗效观察及影响因素分析[J]. 北京大学学报(医学版), 2019, 51(1): 65-69. |
|
||
