北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (1): 145-150. doi: 10.19723/j.issn.1671-167X.2019.01.025
hUTP14a在非小细胞肺癌组织中的表达
张春凤1,刘云2,陆敏3,杜晓娟4,△( )
)
- 1. 北京大学基础医学院医学遗传学系,北京 100191
2. 北京大学医药卫生分析中心,北京 100191
3. 北京大学基础医学院病理学系,北京 100191
4. 北京大学基础医学院细胞生物学系,北京 100191
Expression of hUTP14a in non-small cell lung cancer
Chun-feng ZHANG1,Yun LIU2,Min LU3,Xiao-juan DU4,△()
- 1. Department of Medical Genetics, Peking University School of Basic Medical Sciences, Beijing 100191, China
2. Peking University Centre of Medical and Health Analysis, Beijing 100191, China
3. Department of Pathology, Peking University School of Basic Medical Sciences, Beijing 100191, China
4. Department of Cell Biology, Peking University School of Basic Medical Sciences, Beijing 100191, China
摘要:
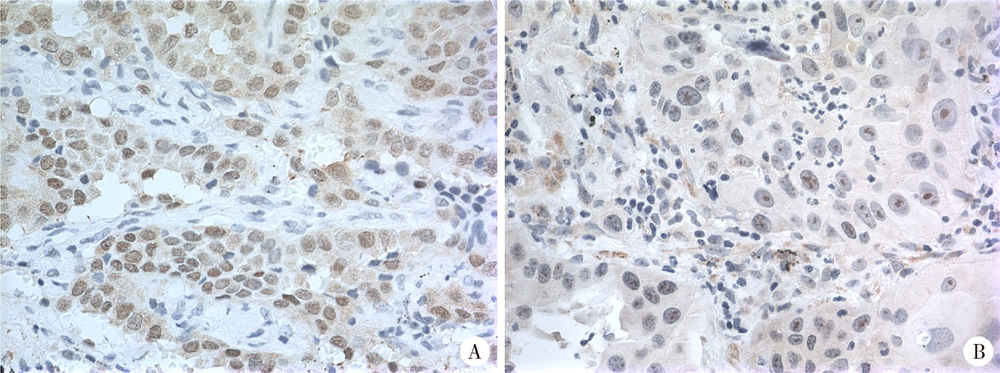
目的:hUTP14a通过促进p53和Rb降解以及增强c-Myc致癌活性促进肿瘤的发生,且在人肝癌和结直肠癌组织中表达升高。本研究检测hUTP14a在非小细胞肺癌(non-small cell lung cancer, NSCLC)组织中的表达,并分析hUTP14a的表达水平与NSCLC患者临床特征的关系。方法:收集2003年5月至2006年4月在北京大学第三医院接受手术治疗并经过组织病理学确诊的123例NSCLC患者的组织蜡块标本(鳞状细胞癌53例,腺癌70例),采用免疫组织化学染色方法分析癌组织及其邻近癌旁非肿瘤组织中hUTP14a的表达水平,应用SPSS 17.0软件的χ 2检验,以患者的性别、年龄、组织类型、肿瘤大小、分化程度以及临床分期等临床病理特征进行分组,对组间肺癌组织中hUTP14a的表达率进行比较。结果:hUTP14a在肺癌组织中的阳性表达率为37.4%(46/123),在癌旁组织中的阳性表达率为0(0/123),在肺癌组织中的表达率显著高于癌旁非肿瘤组织(P<0.001);hUTP14a在肺腺癌中的表达率为48.6%(34/70),在鳞状细胞癌中的表达率为22.6%(12/53),均显著高于相应的癌旁组织[0 (0/70),0 (0/53)]; hUTP14a在肺腺癌中的表达率显著高于在鳞状细胞癌中的表达率(48.6% vs. 22.6%,χ 2=8.66,P=0.03)。进一步分析肺鳞状细胞癌、腺癌与各临床病理特征之间的关系发现,hUTP14a在病理分期(pTNM)晚期的肺鳞状细胞癌患者肿瘤组织中的表达率显著高于pTNM早期的鳞状细胞癌患者,而与肺腺癌的pTNM分期没有显著关联性,未见hUTP14a表达与肺癌的其他临床病理特征存在关联。结论:hUTP14a在肺癌组织中特异性表达升高,而且与肺鳞状细胞癌的pTNM分期具有关联性,提示hUTP14a有可能成为早期筛查诊断NSCLC的候选标志物。
中图分类号:
- R734.2

| [1] |
Zhang L, Li M, Wu N , et al. Time trends in epidemiologic cha-racteristics and imaging features of lung adenocarcinoma: a population study of 21,113 cases in China[J]. PLoS One, 2015,10(8):e0136727.
doi: 10.1371/journal.pone.0136727 pmid: 4552856 |
| [2] | 王媛媛, 毕玉, 王在翔 , 等. 山东省肺癌患者生存分析[J]. 中国卫生统计, 2018,35(1):111-116. |
| [3] |
黄文彦, 刘凯珊 . 以新视角观察p53家族在肺癌发生及治疗中的独特作用[J]. 中国肺癌杂志, 2013,16(8):422-425.
doi: 10.3779/j.issn.1009-3419.2013.08.06 |
| [4] |
李相国, 齐景宪, 易明福 . P16、Rb和PCNA在非小细胞肺癌的表达及临床意义[J]. 临床肺科杂志, 2008,13(8):1002-1004.
doi: 10.3969/j.issn.1009-6663.2008.08.023 |
| [5] |
Scheffner M, Huibregtse JM, Vierstra RD , et al. The HPV-16 E6 and E6-AP complex functions as a ubiquitin-protein ligase in the ubiquitination of p53[J]. Cell, 1993,75(3):495-505.
doi: 10.1016/0092-8674(93)90384-3 pmid: 8221889 |
| [6] |
Uchida C, Miwa S, Kitagawa K , et al. Enhanced Mdm2 activity inhibits pRB function via ubiquitin-dependent degradation[J]. EMBO J, 2005,24(1):160-169.
doi: 10.1038/sj.emboj.7600486 pmid: 15577944 |
| [7] |
Sdek P, Ying H, Chang DL , et al. MDM2 promotes proteasome-dependent ubiquitin-independent degradation of retinoblastoma protein[J]. Mol Cell, 2005,20(5):699-708.
doi: 10.1016/j.molcel.2005.10.017 pmid: 16337594 |
| [8] |
Hu LL, Wang JN, Liu Y , et al. A small ribosomal subunit (SSU) processome component, the human U3 protein 14A (hUTP14A) binds p53 and promotes p53 degradation[J]. J Biol Chem, 2011,286(4):3119-3128.
doi: 10.1074/jbc.M110.157842 pmid: 21078665 |
| [9] |
Liu HJ, Wang JN, Liu Y , et al. Human U3 protein14a is a novel type ubiquitin ligase that binds RB and promotes RB degradation depending on a leucine-rich region[J]. Biochim Biophys Acta Mol Cell Res, 2018,1865(11 Pt A):1611-1620.
doi: 10.1016/j.bbamcr.2018.08.016 |
| [10] |
Zhang JY, Ren PW, Xu D , et al. Human UTP14a promotes colorectal cancer progression by forming a positive regulation loop with c-Myc [J]. Cancer Letters, 2018, 440- 441:106-115.
doi: 10.1016/j.canlet.2018.10.010 |
| [11] |
Zhang JY, Xu D, Liu ZZ , et al. Human U three protein 14a expression is increased in hepatocellular carcinoma and associated with poor prognosis[J]. Chin Med J (Engl), 2017,130(4):470-476.
doi: 10.4103/0366-6999.199839 pmid: 5324385 |
| [12] | Ma T, Lu CX, Guo YF , et al. Human U3 protein 14a plays an anti-apoptotic role in cancer cells[J]. Bio Chem, 2017,398(11):1247-1257. |
| [13] |
Groome PA, Bolejack V, Crowley JJ , et al. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours[J]. J Thorac Oncol, 2007,2(8):694-705.
doi: 10.1097/JTO.0b013e31812d05d5 pmid: 17762335 |
| [14] |
Zhang Y, Xiong Y, Yarbrough WG . ARF promotes MDM2 degradation and stabilizes p53: ARF-INK4a locus deletion impairs both the Rb and p53 tumor suppression pathways[J]. Cell, 1998,92(6):725-734.
doi: 10.1016/S0092-8674(00)81401-4 |
| [15] |
Leduc C, Claverie P, Eymin B , et al. p14ARF promotes RB accumulation through inhibition of its Tip60-dependent acetylation[J]. Oncogene, 2006,25(30):4147-4154.
doi: 10.1038/sj.onc.1209446 pmid: 16501607 |
| [16] |
Bozcuk H, Gumus A, Ozbilim G , et al. Cluster analysis of p-glycoprotein, c-erb-B2 and P53 in relation to tumor histology strongly indicates prognosis in patients with operable non-small cell lung cancer[J]. Med Sci Monit, 2005,11(6):11-20.
doi: 10.1051/medsci/2005216-7669 pmid: 15917726 |
| [17] |
张丽华, 侯振江 . p53在肺癌研究中的进展[J]. 临床肺科杂志, 2006,11(1):59-60.
doi: 10.3969/j.issn.1009-6663.2006.01.030 |
| [1] | 王海, 江一舟. 靶向血管治疗在乳腺癌精准治疗中的分子机制与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 251-256. |
| [2] | 付浩, 申潞艳, 黄冰洋, 马少华. 免疫治疗背景下食管鳞状细胞癌围手术期治疗的临床思考[J]. 北京大学学报(医学版), 2026, 58(2): 266-271. |
| [3] | 李嘉临, 陈力侨, 唐家天, 吴艳, 王安强. 胃肝样腺癌转化治疗1例[J]. 北京大学学报(医学版), 2026, 58(2): 399-404. |
| [4] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [5] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [6] | 侯卫华, 宋书杰, 石中月, 刘露, 金木兰. 食管胃结合部具有显著空泡状核特征的神经内分泌癌1例[J]. 北京大学学报(医学版), 2025, 57(5): 1005-1009. |
| [7] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [8] | 张展奕, 陆敏, 孙悦皓, 董靖晗, 侯小飞, 肖春雷, 王国良, 田晓军, 马潞林, 张洪宪, 张树栋. TFE3重排肾细胞癌合并静脉癌栓患者的临床病理特征及生存分析[J]. 北京大学学报(医学版), 2025, 57(4): 650-661. |
| [9] | 刘杰, 马茗微, 王庆安, 石明, 尹金鹏, 王占平, 申静涛, 高献书. 基于锥形束CT的前列腺癌放射治疗两种体位固定方式摆位误差比较[J]. 北京大学学报(医学版), 2025, 57(4): 692-697. |
| [10] | 许秋实, 刘彤, 王俊杰. 铁死亡相关长链非编码核糖核酸预测放射治疗后非小细胞肺癌患者的临床结局[J]. 北京大学学报(医学版), 2025, 57(3): 569-577. |
| [11] | 朱慧, 闵赛南, 苏家增, 陈艳, 彭歆, 于尧, 俞光岩. 口腔黏膜嗜酸性溃疡的临床病理分析[J]. 北京大学学报(医学版), 2025, 57(3): 620-625. |
| [12] | 刘苗雨, 王思源, 裴林, 王殊. 同步应用戈舍瑞林对年轻乳腺癌患者新辅助化疗疗效的影响[J]. 北京大学学报(医学版), 2025, 57(2): 291-297. |
| [13] | 徐励, 史闻, 李月华, 沈亚俊, 谢尚, 单小峰, 蔡志刚. 含LIM调宁蛋白同源域蛋白1可能作为辅助口腔鳞状细胞癌预后判断的生物学标志物[J]. 北京大学学报(医学版), 2025, 57(1): 19-25. |
| [14] | 马民英, 晁晓芹, 赵扬, 赵国廷. LncRNA SNHG20靶向调控miR-520c-3p/RAB22A通路对人口腔鳞状细胞癌细胞上皮间质转化及微管形成的影响[J]. 北京大学学报(医学版), 2025, 57(1): 26-32. |
| [15] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
|
||
