北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (3): 414-421. doi: 10.19723/j.issn.1671-167X.2019.03.007
体位性心动过速综合征儿童及青少年在直立试验中血流动力学变化
陶春燕1,李红霞1,李雪迎2,唐朝枢3,金红芳1,杜军保1△( )
)
- 1. 北京大学第一医院儿科, 北京 100034
2. 北京大学第一医院医学统计室, 北京 100034
3. 北京大学基础医学院生理与病理生理学系, 北京 100191
4. 教育部分子心血管学重点实验室, 北京 100191
Hemodynamic changes in standing-up test of children and adolescents with postural tachycardia syndrome
Chun-yan TAO1,Hong-xia LI1,Xue-ying LI2,Chao-shu TANG3,Hong-fang JIN1,Jun-bao DU1△()
- 1. Department of Pediatrics, Peking University First Hospital, Beijing 100034, China
2. Department of Statistics, Peking University First Hospital, Beijing 100034, China
3. Department of Physiology and Pathophysiology, Peking University School of Basic Medical Sciences, Beijing 100191, China
4. Key Laboratory of Molecular Cardiovascular Science, the Ministry of Education, Beijing 100191, China
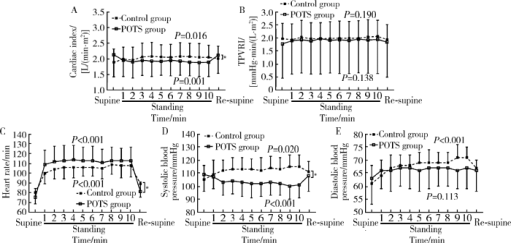
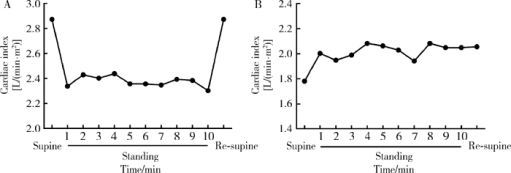
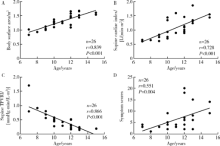
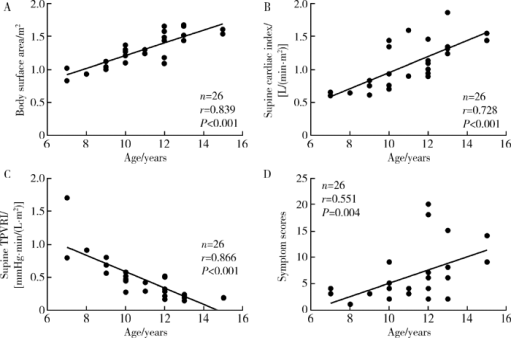
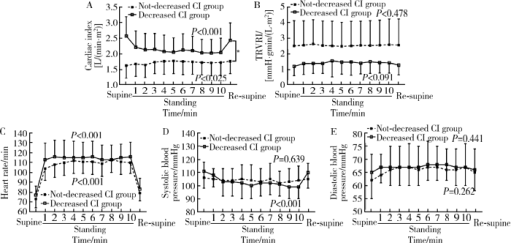
摘要: 目的 分析体位性心动过速综合征(postural tachycardia syndrome, POTS)儿童及青少年直立试验过程中血流动力学变化及不同心脏指数(cardiac index, CI)患者血流动力学指标的差异。方法 回顾性分析26例POTS患者与12例健康对照者间直立试验过程中总外周血管阻力指数(total peripheral vascular resistance index, TPVRI)、心率和血压的变化,并比较两组间各指标变化趋势。根据每位POTS患者直立试验过程中CI变化趋势将患者分为CI降低组(14例)与CI未降低组(12例), 分析两组患者在直立试验过程中CI、TPVRI、心率、血压变化,并比较两组间各指标变化趋势。结果 POTS患者在直立试验过程中CI显著下降(F=6.936, P=0.001), 心率明显增快(F=113.926, P <0.001),收缩压明显降低(F=6.049, P <0.001),而TPVRI (F=2.031, P=0.138)和舒张压(F=2.018, P=0.113)无明显变化。健康对照组CI在直立后显著升高(F=3.646, P=0.016),同时心率明显增快(F=43.970, P<0.001),收缩压(F=4.043, P=0.020)和舒张压(F=8.627, P<0.001)均明显升高,TPVRI (F=1.688, P=0.190)无明显变化。POTS患者与健康对照组比较,CI (F=6.221, P=0.001)、心率(F=6.203, P<0.001)和收缩压(F=7.946, P<0.001)随时间变化趋势显著不同,而TPVRI和舒张压在两组间的变化趋势差异无统计学意义(P>0.05)。CI降低组与CI未降低组POTS患者在直立试验中CI变化趋势差异有统计学意义(F=14.723, P<0.001), 前者直立后收缩压明显降低(F=8.010, P<0.001),而后者却无明显变化(F=0.612, P=0.639), TPVRI、心率和舒张压在CI降低组与CI未降低组间随时间变化趋势差异无统计学意义(P>0.05)。年龄是POTS患者直立后CI呈下降趋势的独立影响因素(P=0.013, OR=2.233; 95% CI:1.183~4.216)。结论 POTS患者在直立试验过程中存在明显的血流动力学变化,不同患者心输出量变化可能不同,年龄是心输出量下降的独立影响因素。
中图分类号:
- R725.4



| [1] |
Goodman BP . Evaluation of postural tachycardia syndrome (POTS)[J]. Auton Neurosci, 2018,215:12-19.
doi: 10.1016/j.autneu.2018.04.004 |
| [2] |
Johnson JN, Mack KJ, Kuntz NL , et al. Postural orthostatic tachycardia syndrome: a clinical review[J]. Pediatr Neurol, 2010,42(2):77-85.
doi: 10.1016/j.pediatrneurol.2009.07.002 |
| [3] | Stewart JM, Pianosi P, Shaban MA , et al. Postural hyperventilation as a cause of postural tachycardia syndrome: increased systemic vascular resistance and decreased cardiac output when upright in all postural tachycardia syndrome variants[J]. J Am Heart Assoc, 2018,7(13):e008854. |
| [4] |
Li H, Han Z, Chen S, et al. Total peripheral vascular resistance, cardiac output ,plasma C-type natriuretic peptide level in children with postural tachycardia syndrome[J]. J Pediatr, 2015, 166(6): 1385- 1389. e1-2.
doi: 10.1016/j.jpeds.2015.03.032 |
| [5] |
Zheng X, Chen Y, Du J . Recent advances in the understanding of the mechanisms underlying postural tachycardia syndrome in children: practical implications for treatment[J]. Cardiol Young, 2017,27(3):413-417.
doi: 10.1017/S1047951116002559 |
| [6] |
Medow MS, Stewart JM . The postural tachycardia syndrome[J]. Cardiol Rev, 2007,15(2):67-75.
doi: 10.1097/01.crd.0000233768.68421.40 |
| [7] | 中华医学会儿科学分会心血管学组, 《中华儿科杂志》编辑委员会, 北京医学会儿科学分会心血管学组, 等. 2016儿童晕厥诊断指南(2016年修订版)[J]. 中华儿科杂志, 2016,54(4):246-250. |
| [8] | 中华医学会儿科学分会心血管学组, 《中华儿科杂志》编辑委员会. 儿童晕厥诊断指南[J]. 中华儿科杂志, 2009,47(2):99-101. |
| [9] |
Garland EM, Celedonio JE, Raj SR . Postural tachycardia syndrome: beyond orthostatic intolerance[J]. Curr Neurol Neurosci Rep, 2015,15(9):60.
doi: 10.1007/s11910-015-0583-8 |
| [10] |
Stewart JM, Medow MS, Glover JL , et al. Persistent splanchnic hyperemia during upright tilt in postural tachycardia syndrome[J]. Am J Physiol Heart Circ Physiol, 2006,290(2):H665-H673.
doi: 10.1152/ajpheart.00784.2005 |
| [11] |
Fu Q, Vangundy TB, Galbreath MM , et al. Cardiac origins of the postural orthostatic tachycardia syndrome[J]. J Am Coll Cardiol, 2010,55(25):2858-2868.
doi: 10.1016/j.jacc.2010.02.043 |
| [12] | Jacob G, Biaggioni I, Mosqueda-Garcia R , et al. Relation of blood volume and blood pressure in orthostatic intolerance[J]. Am J Med Sci, 1998,315(2):95-100. |
| [13] |
Farquhar WB, Taylor JA, Darling SE , et al. Abnormal baroreflex responses in patients with idiopathic orthostatic intolerance[J]. Circulation, 2000,102(25):3086-3091.
doi: 10.1161/01.CIR.102.25.3086 |
| [14] |
Zhang Q, Liao Y, Tang C , et al. Twenty-four-hour urinary sodium excretion and postural orthostatic tachycardia syndrome[J]. J Pediatr, 2012,161(2):281-284.
doi: 10.1016/j.jpeds.2012.01.054 |
| [15] | 蔺婧, 刘平, 王瑜丽 , 等. 儿童体位性心动过速综合征治疗随访的单中心研究[J]. 中华实用儿科临床杂志, 2015,30(13):983-987. |
| [16] | 蔺婧, 刘平, 王瑜丽 , 等. 直立试验心率变化预测口服补液盐治疗体位性心动过速综合征的效果[J]. 中华儿科杂志, 2015,53(1):25-29. |
| [17] |
Li H, Wang Y, Liu P , et al. Body mass index (BMI) is associated with the therapeutic response to oral rehydration solution in children with postural tachycardia syndrome[J]. Pediatr Cardiol, 2016,37(7):1313-1318.
doi: 10.1007/s00246-016-1436-1 |
| [18] |
Lu W, Yan H, Wu S , et al. Hemocytometric measures predict the efficacy of oral rehydration for children with postural tachycardia syndrome[J]. J Pediatr, 2017,187:220-224.
doi: 10.1016/j.jpeds.2017.04.034 |
| [19] |
Raj SR, Robertson D . Blood volume perturbations in the postural tachycardia syndrome[J]. Am J Med Sci, 2007,334(1):57-60.
doi: 10.1097/MAJ.0b013e318063c6c0 |
| [20] | Karataş Z, Alp H, Sap F , et al. Usability of QTc dispersion for the prediction of orthostatic intolerance syndromes[J]. Eur J Paediatr Neurol, 2012,16(5):467-474. |
| [21] |
Wang Y, Zhang C, Chen S , et al. Frequency domain indices of heart rate variability are useful for differentiating vasovagal syncope and postural tachycardia syndrome in children[J]. J Pediatr, 2019,207:59-63.
doi: 10.1016/j.jpeds.2018.11.054 |
| [22] |
Lin J, Jin H, Du J . Assessment of therapeutic biomarkers in the treatment of children with postural tachycardia syndrome and vasovagal syncope[J]. Cardiol Young, 2014,24(5):792-796.
doi: 10.1017/S1047951114000316 |
| [23] |
Altun B, Arici M . Salt and blood pressure: time to challenge[J]. Cardiology, 2006,105(1):9-16.
doi: 10.1159/000088265 |
| [24] |
Hart EC, Joyner MJ, Wallin BG , et al. Sex, ageing and resting blood pressure: gaining insights from the integrated balance of neural and haemodynamic factors[J]. J Physiol, 2012,590(9):2069-2079.
doi: 10.1113/jphysiol.2011.224642 |
| [25] | Bevan JA . Control of peripheral vascular resistance: evidence based on the in vitro study of resistance arteries[J]. Clin Invest Med, 1987,10(6):568-572. |
| [1] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [2] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [3] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [4] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [5] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [6] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [7] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
| [8] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [9] | 程雅雯, 李德利, 赵彦, 夏斌, 刘云松. 青少年恒牙牙体缺损的修复难点及过渡修复的方式选择[J]. 北京大学学报(医学版), 2025, 57(1): 208-213. |
| [10] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [11] | 王敏, 李倩. 青少年抑郁症患者心理弹性影响因素的路径分析[J]. 北京大学学报(医学版), 2024, 56(5): 809-814. |
| [12] | 赵双云, 邹思雨, 李雪莹, 沈丽娟, 周虹. 中文版口腔健康素养量表简版(HeLD-14)在学龄前儿童家长中应用的信度和效度评价[J]. 北京大学学报(医学版), 2024, 56(5): 828-832. |
| [13] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [14] | 岳芷涵,韩娜,鲍筝,吕瑾莨,周天一,计岳龙,王辉,刘珏,王海俊. 儿童早期体重指数轨迹与超重风险关联的前瞻性队列研究[J]. 北京大学学报(医学版), 2024, 56(3): 390-396. |
| [15] | 费秀文,刘斯,汪波,董爱梅. 成人及儿童组织坏死性淋巴结炎临床特征及治疗[J]. 北京大学学报(医学版), 2024, 56(3): 533-540. |
|
||
