北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (6): 1071-1077. doi: 10.19723/j.issn.1671-167X.2019.06.017
18F-FDG PET/CT联合多种肿瘤标志物在结直肠中分化腺癌术后复发及转移中的应用价值
张旭初,张建华,王荣福( ),范岩,付占立,闫平,赵光宇,白艳霞
),范岩,付占立,闫平,赵光宇,白艳霞
- 北京大学第一医院核医学科,北京 100034
Diagnostic value of 18F-FDG PET/CT and tumor markers (CEA, CA19-9, CA24-2) in recurrence and metastasis of postoperative colorectal moderately differentiated adenocarcinoma
Xu-chu ZHANG,Jian-hua ZHANG,Rong-fu WANG(),Yan FAN,Zhan-li FU,Ping YAN,Guang-yu ZHAO,Yan-xia BAI
- Department of Nuclear Medicine, Peking University First Hospital, Beijing 100034, China
摘要:
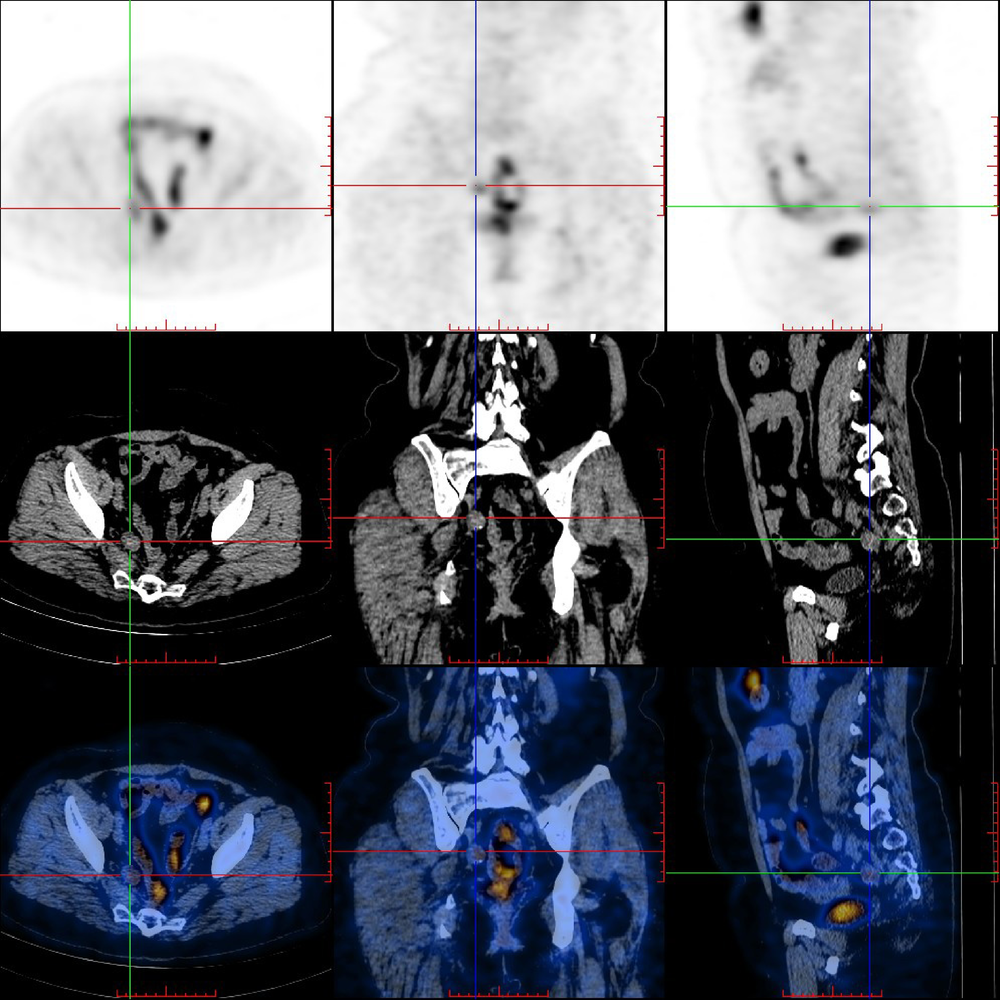
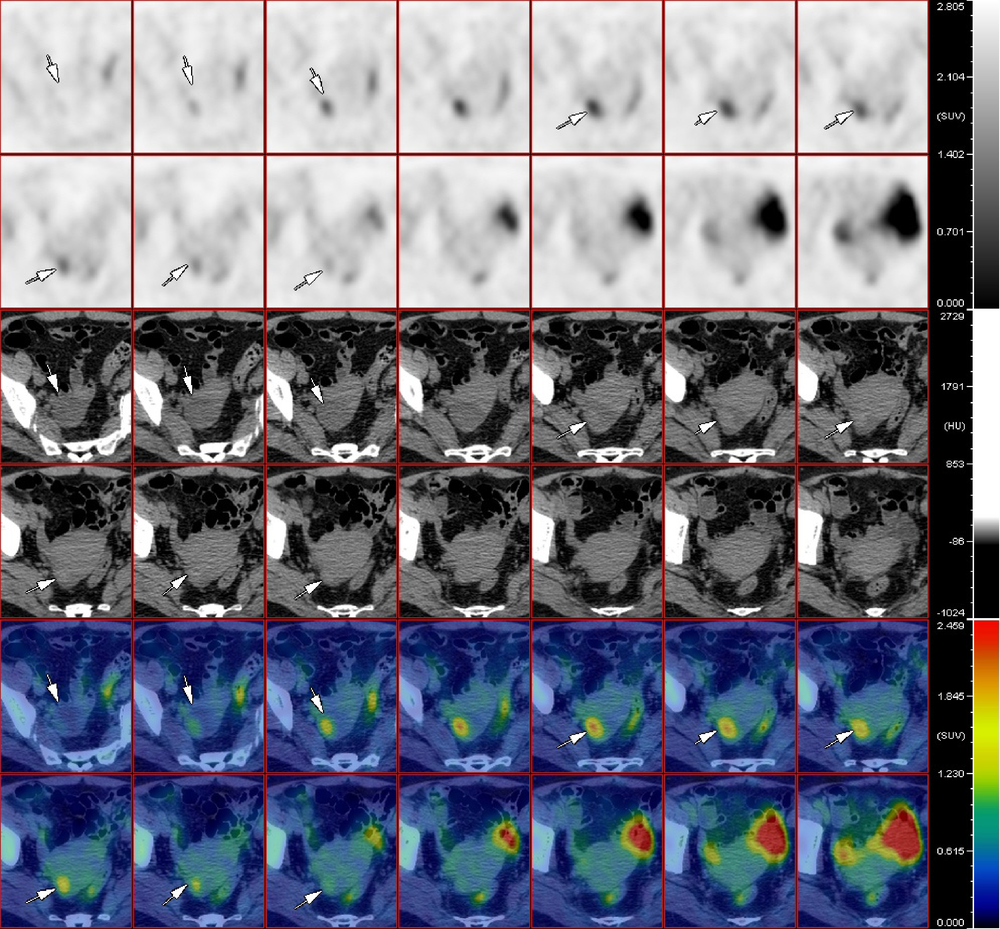
目的 探讨18F-FDG PET/CT与肿瘤标志物(CEA、CA19-9、CA24-2)在结直肠中分化腺癌患者术后探测及提示复发和转移灶中的应用。方法 对55例结直肠中分化腺癌患者进行 18F-FDG PET/CT显像及肿瘤标志物筛查,并与病理及临床随访结果进行比较。结果 对18F-FDG PET/CT对于结直肠中分化腺癌术后复发及转移灶的诊断效能为:灵敏度95.74%(45/47),特异性75.00%(6/8),阳性预测值95.74%(45/47),阴性预测值75.00%(6/8),准确率92.73%(51/55),其中假阳性2例,假阴性2例。CEA组、CA19-9组、CA24-2组及肿瘤标记物联合组灵敏度分别为68.09%(32/47)、28.57%(12/42)、40.00%(16/40)及74.47%(35/47),特异性为50.00%(4/8)、66.67%(4/6)、71.73%(5/7)及50.00%(4/8),阳性预测值为88.89%(32/36)、85.71%(12/14)、88.89%(16/18)及89.74%(35/39),阴性预测值为26.67%(4/19)、11.42%(4/34)、17.24%(5/29)及25.00%(4/16),准确率为65.45%(36/55)、32.65%(16/49)、44.68%(21/47)及70.91%(39/55)结论 18F-FDG PET/CT对于结直肠癌术后中分化腺癌患者复发及转移灶的探测具有较高的灵敏度及特异性,各项肿瘤标志物对病灶转移及复发均有一定的提示作用,多项肿瘤标志物联合应用更准确。
中图分类号:
- R735.5

| [1] | 吴菲, 林国桢, 张晋昕 . 我国恶性肿瘤发病现状及趋势[J]. 中国肿瘤, 2012,21(2):81-85. |
| [2] | 阮丽琴, 李太原, 周凤凤 . 不同年龄组的结直肠癌临床流行病学分析[J]. 实用临床医学, 2016,17(4):86-87. |
| [3] | 张小龙, 高枫, 陈利生 , 等. 结直肠癌病理组织学类型分析[J]. 广西医学, 2008,30(11):1671-1672. |
| [4] | 陈美玲 . 291例结直肠癌患者的临床病理分析[J]. 大家健康(学术版), 2015,9(8):66-67. |
| [5] | 邱大胜, 胡晓燕, 彭辽河 , 等. 18F-FDG-PET/CT对结直肠癌术后血清CEA升高患者的诊断价值 [J]. 临床放射学杂志, 2013,32(12):1739-1742. |
| [6] | 路晓雯, 刘林祥, 崔新建 , 等. 18F-FDG PET/CT对结直肠癌术后血清CEA升高病例的临床诊断价值 [J]. 泰山医学院学报, 2010,31(2):83-85. |
| [7] | 潘睿. 中国慢性病前瞻性研究队列恶性肿瘤发病与死亡分析[C], 2017. |
| [8] |
黄利娟, 陈继贵, 刘丽 , 等. 结直肠癌患者血清肿瘤标志物水平与预后关系[J]. 中国公共卫生, 2011,27(5):563-566.
doi: 10.11847/zgggws-2011-27-05-16 |
| [9] | Van Cutsem E, Cervantes A, Adam R , et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer[J]. Ann Oncol, 2016,27(8):1386-1422. |
| [10] | 王贵玉 . 结直肠癌NCCN、NICE及ESMO指南的对比分析和解读[J]. 中国癌症杂志, 2015,25(11):849-853. |
| [11] | Schmoll HJ, Van Cutsem E, Stein A , et al. ESMO Consensus Guidelines for management of patients with colon and rectal can-cer. A personalized approach to clinical decision making[J]. Ann Oncol, 2012,23(10):2479-2516. |
| [12] | Chan K, Welch S, Walker-Dilks C , et al. Evidence-based guideline recommendations on the use of positron emission tomography imaging in colorectal cancer[J]. Clin Oncol (R Coll Radiol), 2012,24(4):232-249. |
| [13] | 王晶晶, 陈康, 徐万菊 . 直肠癌患者手术前后血清CA199和CA242水平测定及预后评价[J]. 中华肿瘤防治杂志, 2009,14(21):1667-1668. |
| [14] | 刘传, 清水汪, 王宁 , 等. 结直肠癌术前血清CEA、CA199表达水平与临床病理关系的研究[J]. 医学研究杂志, 2012,41(3):27-30. |
| [15] | 周华胜, 梁光林 . 癌胚抗原测定在直肠癌手术前后及药物化疗过程中的追踪研究[J]. 河北医学, 2010,16(4):455-456. |
| [16] | Lim YK, Kam MH, Eu KW . Carcinoembryonic antigen screening: how far should we go?[J]. Singapore Med J, 2009,50(9):862-865. |
| [17] | 陈恺杰 . 3种血清肿瘤标志物在诊断大肠癌中的价值[J]. 广东医学院学报, 2005,23(4):384-385. |
| [18] | 高志海, 田志军, 安燚 . 五种肿瘤标志物联合检测在胃和结直肠癌诊断及随访中的临床意义[J]. 医学综述, 2012,18(10):1595-1597. |
| [1] | 季加孚, 韦静涛, 季科, 步召德. 胃癌诊疗的瓶颈与破局:迈向精准化与智能化融合的新纪元[J]. 北京大学学报(医学版), 2026, 58(2): 231-238. |
| [2] | 步召德, 冯梦宇, 季科. 早期胃癌行前哨淋巴结导航手术的实践与思考[J]. 北京大学学报(医学版), 2026, 58(2): 239-243. |
| [3] | 高加勒, 张忠涛. 局部进展期直肠癌精准治疗现状与展望[J]. 北京大学学报(医学版), 2026, 58(2): 247-250. |
| [4] | 王海, 江一舟. 靶向血管治疗在乳腺癌精准治疗中的分子机制与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 251-256. |
| [5] | 罗必显, 刘洪铭, 谢伟勋, 龚渭华. 产甲胎蛋白胃癌的新临床特征和前沿科学问题[J]. 北京大学学报(医学版), 2026, 58(2): 257-265. |
| [6] | 杜文, 章文博, 于尧, 刘硕, 苏惠裕, 胡耒豪, 唐祖南, 吴彬彰, 陈震, 李家琦, 王昊, 彭歆. 口腔颌面部肿瘤"数智化外科"诊疗流程探索与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 278-284. |
| [7] | 王楠楠, 袁大晋, 朱昱冰, 丁磊. 结直肠癌根治术后肝转移风险多中心列线图预测模型的构建与验证[J]. 北京大学学报(医学版), 2026, 58(2): 290-300. |
| [8] | 刘友东, 吕亚军, 陈杰, 臧明德, 潘宏达, 刘晓文, 陆俊, 刘凤林. 全腹腔镜保留贲门胃底胃次全切除术治疗中上部胃癌的疗效及安全性[J]. 北京大学学报(医学版), 2026, 58(2): 301-306. |
| [9] | 李嘉临, 陈力侨, 唐家天, 吴艳, 王安强. 胃肝样腺癌转化治疗1例[J]. 北京大学学报(医学版), 2026, 58(2): 399-404. |
| [10] | 李斌, 梁寒. 机器人胃癌根治术:研究进展与实践挑战[J]. 北京大学学报(医学版), 2026, 58(2): 416-422. |
| [11] | 董海峰, 陈恒星, 张常华. 恶性肿瘤中蛋白质乳酸化修饰的研究进展[J]. 北京大学学报(医学版), 2026, 58(2): 423-430. |
| [12] | 李宏杨, 黄涛, 王琳琳. 脂肪肌肉比率与卵巢良性肿瘤风险的关联性[J]. 北京大学学报(医学版), 2026, 58(1): 169-174. |
| [13] | 高若凡, 马天宇, 王润楷, 殷雨辰, 李芮迪, 王丹丹, 夏斌. 细胞膜囊泡递送靶向肿瘤坏死因子-α的小干扰RNA对牙髓干细胞的抗炎作用[J]. 北京大学学报(医学版), 2026, 58(1): 22-29. |
| [14] | 向钊, 杨莉, 杨静. 非靶向代谢组学揭示原发性干燥综合征血小板减少患者血清差异代谢物及代谢通路[J]. 北京大学学报(医学版), 2025, 57(6): 1042-1050. |
| [15] | 刘艳华, 陆敏, 赵旭阳, 张宽根, 武睿, 梅放, 戴志豪, 由江峰, 裴斐. 肿瘤转移抑制基因LASS2去磷酸化对液泡型ATP酶活性及前列腺癌侵袭性的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1113-1123. |
|
||
