北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (6): 1067-1070. doi: 10.19723/j.issn.1671-167X.2019.06.016
2017版美国放射学会甲状腺影像学报告与数据系统应用价值探索
付鹏,陈文( ),崔立刚,葛辉玉,王淑敏
),崔立刚,葛辉玉,王淑敏
- 北京大学第三医院超声诊断科,北京 100191
Applicational value of 2017 ACR TI-RADS stratification in diagnosing thyroid nodules
Peng FU,Wen CHEN(),Li-gang CUI,Hui-yu GE,Shu-min WANG
- Department of Ultrasound, Peking University Third Hospital, Beijing 100191, China
摘要:
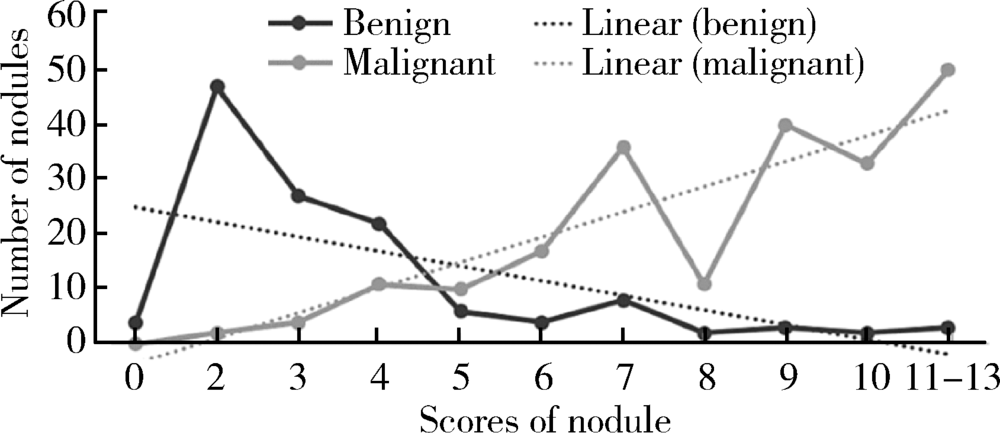
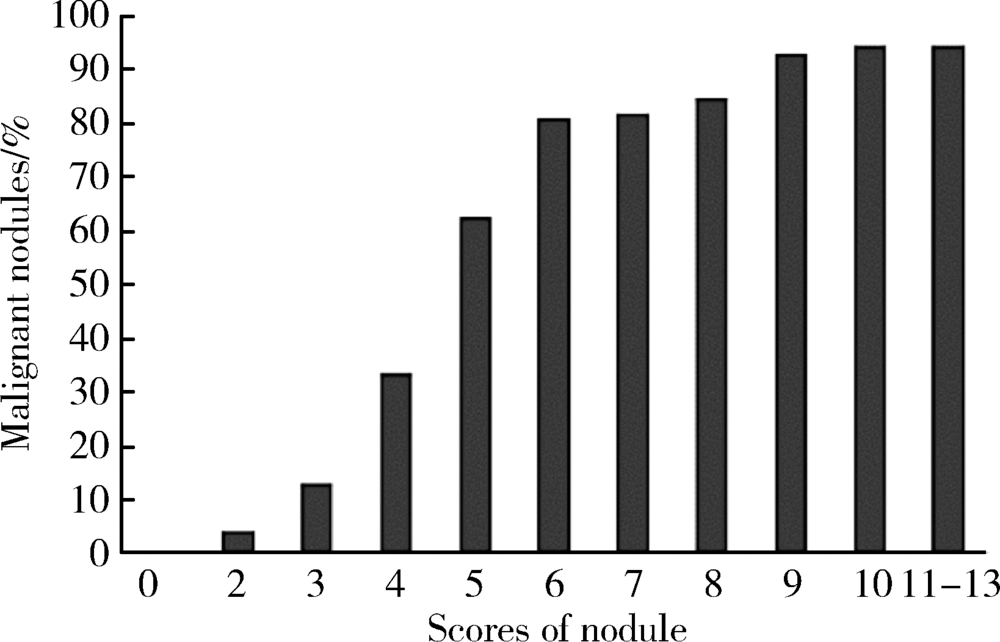
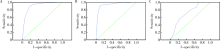
目的 评估应用2017年美国放射学会(American College of Radiology,ACR)发布的甲状腺影像学报告与数据系统(thyroid imaging reporting and data system,TI-RADS) 对甲状腺进行危险分层的价值,并依据结果提出优化分类的建议。方法 回顾性分析北京大学第三医院应用2017版ACR TI-RADS评估的342例影像资料完整的甲状腺结节,将评分结果与病理结果进行对比,获得不同分值区间恶性结节的比例,并分别对最大径>1 cm及最大径≤1 cm的结节使用ROC曲线评价诊断效能。结果 利用该评分系统对结节进行危险分层,全部结节、最大径>1 cm的结节、最大径≤1 cm的结节ROC曲线下面积分别为0.907、0.936、0.717。随着评分值的增加,良性结节比例逐渐下降,恶性结节所占比例逐渐增长,评分值4~6分区间恶性结节比例增长明显,以评分值为3的恶性结节比例为基准,4、5、6分结节恶性结节分别增长1.6倍、3.8倍、5.3倍,6~8分区间恶性结节稳定在81%~84%,而9分及以上恶性结节比例稳定在93%~94%,依据恶性结节的比例分布特点调整分类,TI-RADS 1类、TI-RADS 2类、TI-RADS 3类仍然分别对应0分、2分、3分,TI-RADS 4类细分为TI-RADS 4a类、TI-RADS 4b类、TI-RADS 4c类,分别对应4分、5分、6~8分,而≥9分的结节划分为TI-RADS 5类。结论 2017版ACR TI-RADS对最大径>1 cm的甲状腺结节具有较高的诊断价值,而对最大径≤1 cm的结节诊断价值欠佳。根据不同评分值区间恶性结节比例的分布特点,适当调整分类将能更详细、准确地预测结节的恶性风险。
中图分类号:
- R736.1




| [1] | Tessler FN, Middleton WD, Grant EG , et al. ACR thyroid imaging, reporting and data system (TI-RADS): White paper of the ACR TI-RADS Committee[J]. J Am Coll Radiol, 2017,14(5):587-595. |
| [2] | Grant EG, Tessler FN, Hoang JK , et al. Thyroid ultrasound reporting lexicon: white paper of the ACR Thyroid Imaging, Reporting and Data System (TIRADS) Committee[J]. J Am Coll Ra-diol, 2015,12(12):1272-1279. |
| [3] | Gharib H, Papini E, Garber JR , et al. AACE/AME Guidelines American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: 2016 update[J]. Endocr Pract, 2016,22(5):622-639. |
| [4] | Middleton WD, Teefey SA, Reading CC , et al. Multiinstitutional analysis of thyroid nodule risk stratification using the American College of Radiology Thyroid Imaging Reporting and Data System[J]. AJR Am J Roentgenol, 2017,208(6):1331-1341. |
| [5] | Kumbhar SS, O’Malley RB, Robinson TJ, et al. Why thyroid surgeons are frustrated with radiologists: Lessons learned from pre-and postoperative US[J]. Radiographics, 2016,36(7):150-250. |
| [6] | Gunderman RB, Mcneive LR . Is structured reporting the answer?[J]. Radiology, 2014,273(1):7-9. |
| [7] | Haugen BR, Alexander EK, Bible KC , et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer[J]. Thyroid, 2016,26(1):1-133. |
| [8] | Haddad RI, Lydiatt WM, Ball DW , et al. Anaplastic Thyroid Carcinoma, Version 2.2015[J]. J Natl Compr Canc Netw, 2015,13(9):1140-1150. |
| [9] | Wémeau JL, Sadoul JL, d’Herbomez M, et al. Guidelines of the French Society of Endocrinology for the management of thyroid nodules[J]. Ann Endocrinol (Paris), 2011,72(4):251-281. |
| [10] | Shin JH, Baek JH, Chung J , et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised Korean Society of Thyroid Radiology consensus statement and recommendations[J]. Korean J Radiol, 2016,17(3):370-395. |
| [11] | 刘红, 胡正明, 罗海愉 , 等. ACR TI-RADS分类在诊断甲状腺结节中的应用价值探究[J]. 中国超声医学杂志, 2018,34(8):673-675. |
| [12] | 钟敏莹, 石小红, 杨丽丽 , 等. TI-RADS分类系统对不同直径甲状腺结节的诊断价值[J]. 中国超声医学杂志, 2016,32(4):289-291. |
| [1] | 马豆豆, 马晓彩, 常天静, 王丽芳, 丁艳, 石连杰. 临床表现似系统性红斑狼疮的大B细胞淋巴瘤骨髓受累1例[J]. 北京大学学报(医学版), 2026, 58(3): 666-669. |
| [2] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [3] | 王月, 梁宇红. 繁茂型牙骨质-骨结构不良1例[J]. 北京大学学报(医学版), 2026, 58(1): 220-224. |
| [4] | 池彦廷, 蒋鸿杰, 陈艳, 徐志秀, 李斌斌. 直接免疫荧光在口腔黏膜寻常型天疱疮诊断中的价值: 基于多指标联合分析的回顾性研究[J]. 北京大学学报(医学版), 2026, 58(1): 68-73. |
| [5] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [6] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [7] | 肖晓笛, 夏有辰, 柳剑英, 付鹏. 左侧胸锁乳突肌间血管内乳头状内皮增生1例[J]. 北京大学学报(医学版), 2025, 57(5): 1002-1004. |
| [8] | 孙翔宇, 袁超, 周芯竹, 刁婧, 郑树国. 唾液微生态在口腔及全身疾病早期防治中的应用[J]. 北京大学学报(医学版), 2025, 57(5): 859-863. |
| [9] | 陈钊, 邱永康, 康磊. 经典型Sweet综合征 18F-FDG PET/CT多脏器异常显像1例[J]. 北京大学学报(医学版), 2025, 57(2): 403-407. |
| [10] | 方媛媛, 徐帆, 雷杰, 张昊, 张文宇, 孙宇, 吴宏新, 傅开元, 毛伟玉. 基于颞下颌关节紊乱病诊断标准的临床自动诊断系统的建立及验证[J]. 北京大学学报(医学版), 2025, 57(1): 192-201. |
| [11] | 车佳璐, 刘子臣, 李琨, 张晨, 车南颖. 全自动EasyNAT核酸快速检测系统检测石蜡包埋组织诊断结核病的临床价值[J]. 北京大学学报(医学版), 2024, 56(6): 1047-1051. |
| [12] | 原晋芳, 王新利, 崔蕴璞, 王雪梅. 尿促黄体生成素在女童中枢性性早熟预测中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 788-793. |
| [13] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [14] | 钟华, 李原, 徐丽玲, 白明欣, 苏茵. 18F-FDG PET/CT在风湿免疫病中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 853-859. |
| [15] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
|
||
