北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (1): 220-224. doi: 10.19723/j.issn.1671-167X.2026.01.030
繁茂型牙骨质-骨结构不良1例
王月1, 梁宇红2,*( )
)
- 1. 北京大学国际医院口腔科, 北京 102206
2. 北京大学口腔医学院·口腔医院急诊科, 国家口腔医学中心, 国家口腔疾病临床医学研究中心, 口腔生物材料和数字诊疗装备国家工程研究中心, 口腔数字医学北京市重点实验室, 国家卫生健康委员会口腔数字医学重点实验室, 国家药品监督管理局口腔材料重点实验室, 北京 100081
Florid cemento-osseous dysplasia: A case report
Yue WANG1, Yuhong LIANG2,*()
- 1. Department of Stomatology, Peking University International Hospital, Beijing 102206, China
2. Department of Oral Emergency, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology & NHC Key Laboratory of Digital Stomatology & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
摘要:
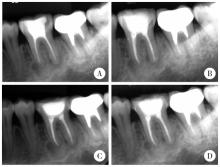
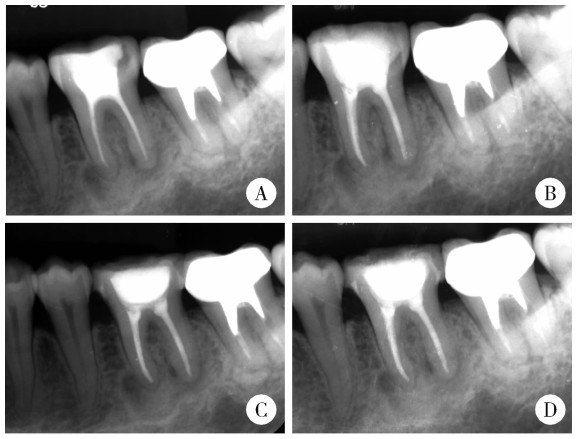
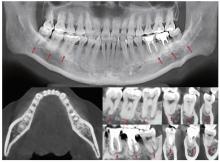
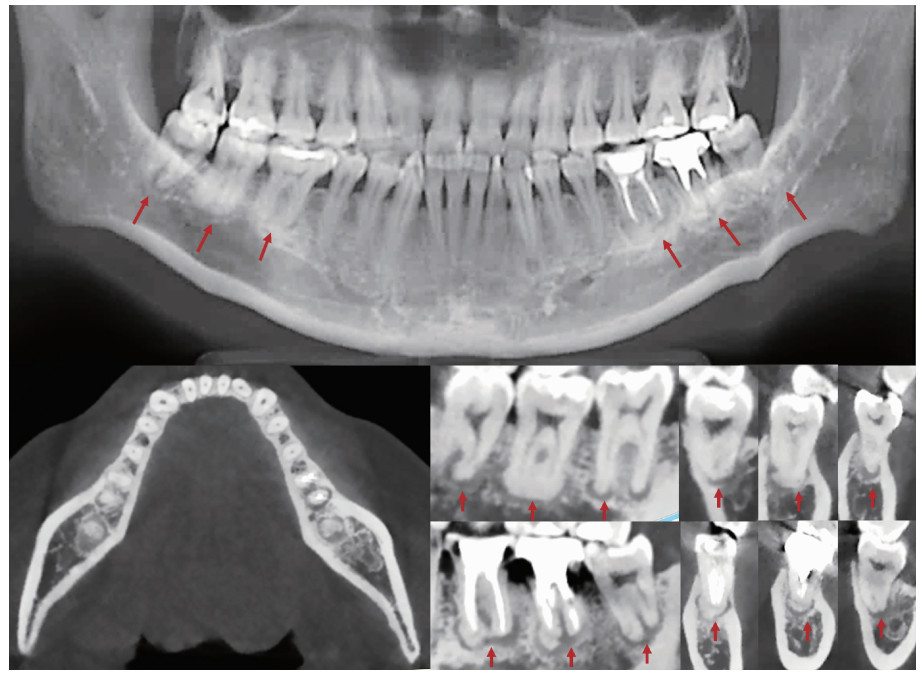
牙骨质-骨结构不良(cemento-osseous dysplasia, COD)属于临床少见的一种纤维-骨肿瘤及结构不良, 病变通常无症状, 多通过X线检查偶然发现。本文报道1例就诊于北京大学国际医院口腔科的45岁女性繁茂型牙骨质-骨结构不良(florid cemento-osseous dysplasia, FLCOD)病例, 患者因左下后牙充填体脱落3周就诊, 临床检查发现左下颌第一磨牙(36)存在继发龋坏达髓腔, 但无牙髓炎或根尖周病症状。邻近牙齿(左下颌第三磨牙)及对侧磨牙(右下颌第一、二、三磨牙)牙髓活力测试反应正常, 无肿胀、窦道或牙齿松动。锥形束CT(cone beam computed tomography, CBCT)检查显示, 双侧下颌磨牙根尖周区域存在多灶性混合密度病变, 符合世界卫生组织制定的FLCOD诊断标准。病变累及的6颗牙齿(36、37、38、46、47和48)根尖周影像学表现多样, 呈现骨质溶解破坏期、类牙骨质小体形成期与钙化成熟期三期并存的特征。本病例为临床少见的FLCOD病例, 诊断主要依据其无临床症状的病程、牙髓状态及典型的影像学表现。CBCT在清晰显示病变、提供诊断依据方面发挥了关键作用。治疗策略上应着重处理患者的继发龋等伴发病变, 控制局部与全身风险因素, 而非针对COD病变本身进行干预, 预后还需长期随访。
中图分类号:
- R782.1




| 1 |
doi: 10.1016/j.oooo.2016.04.013 |
| 2 |
|
| 3 |
史册, 李志民, 孙宏晨. 纤维-骨肿瘤及结构不良的临床病理特征与鉴别诊断[J]. 中华口腔医学杂志, 2023, 58 (2): 124- 130.
|
| 4 |
doi: 10.3390/diagnostics12020238 |
| 5 |
doi: 10.1016/j.cden.2009.12.007 |
| 6 |
doi: 10.1016/j.jds.2021.03.009 |
| 7 |
doi: 10.1007/s10006-025-01394-8 |
| 8 |
doi: 10.1016/j.pathol.2022.10.006 |
| 9 |
|
| 10 |
doi: 10.1016/j.jormas.2020.06.002 |
| 11 |
doi: 10.3390/dj11050138 |
| 12 |
doi: 10.1016/j.oooo.2024.06.011 |
| 13 |
doi: 10.1111/acel.13726 |
| 14 |
doi: 10.1902/jop.2015.140533 |
| 15 |
doi: 10.1007/s10006-012-0314-0 |
| 16 |
|
| 17 |
|
| [1] | 肖晓笛, 夏有辰, 柳剑英, 付鹏. 左侧胸锁乳突肌间血管内乳头状内皮增生1例[J]. 北京大学学报(医学版), 2025, 57(5): 1002-1004. |
| [2] | 刘杰, 马茗微, 王庆安, 石明, 尹金鹏, 王占平, 申静涛, 高献书. 基于锥形束CT的前列腺癌放射治疗两种体位固定方式摆位误差比较[J]. 北京大学学报(医学版), 2025, 57(4): 692-697. |
| [3] | 石宇彤, 危伊萍, 胡文杰, 徐涛, 张浩筠. 罹患重度牙周炎下颌磨牙拔牙微翻瓣牙槽嵴保存效果评价[J]. 北京大学学报(医学版), 2025, 57(1): 33-41. |
| [4] | 钟华, 李原, 徐丽玲, 白明欣, 苏茵. 18F-FDG PET/CT在风湿免疫病中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 853-859. |
| [5] | 薄士仕,高承志. 基于卷积神经网络实现锥形束CT牙齿分割及牙位标定[J]. 北京大学学报(医学版), 2024, 56(4): 735-740. |
| [6] | 哈雪梅,姚永正,孙莉华,辛春杨,熊焰. 实性肺胎盘样变形1例及文献复习[J]. 北京大学学报(医学版), 2023, 55(2): 357-361. |
| [7] | 章锦花,潘洁,孙志鹏,王霄. 不同根管内容物对口腔颌面锥形束CT诊断牙根纵裂准确性的影响[J]. 北京大学学报(医学版), 2023, 55(2): 333-338. |
| [8] | 潘孟乔,刘建,徐莉,徐筱,侯建霞,李小彤,王晓霞. 牙周-正畸-正颌联合治疗骨性安氏Ⅲ类错 |
| [9] | 叶佳学,梁宇红. 牙髓专科医师应用锥形束CT的现况调查[J]. 北京大学学报(医学版), 2023, 55(1): 114-119. |
| [10] | 高娟,吕航苗,马慧敏,赵一姣,李小彤. 锥形束CT三维体积测量评估骨性Ⅲ类错 |
| [11] | 刘伟涛,王怡然,王雪东,周彦恒. 锥形束CT研究上颌反复扩缩前方牵引后上颌骨缝的三维变化[J]. 北京大学学报(医学版), 2022, 54(2): 346-355. |
| [12] | 孟圆,张丽琪,赵雅宁,柳登高,张祖燕,高岩. 67例上颌根尖周囊肿的三维影像特点分析[J]. 北京大学学报(医学版), 2021, 53(2): 396-401. |
| [13] | 曹畅,王菲,王恩博,刘宇. β-磷酸三钙用于下颌第三磨牙拔除术后骨缺损修复的自身对照研究[J]. 北京大学学报(医学版), 2020, 52(1): 97-102. |
| [14] | 谢晓艳,贾淑梅,孙志辉,张祖燕. 分辨率设置与锥形束CT检测牙根外吸收的可靠性[J]. 北京大学学报(医学版), 2019, 51(1): 75-79. |
| [15] | 卢昕,张立宁. 肌活检在特发性炎性肌病诊断和临床分型中的价值[J]. 北京大学学报(医学版), 2018, 50(6): 949-951. |
|
||
