北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (6): 1173-1177. doi: 10.19723/j.issn.1671-167X.2019.06.035
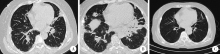
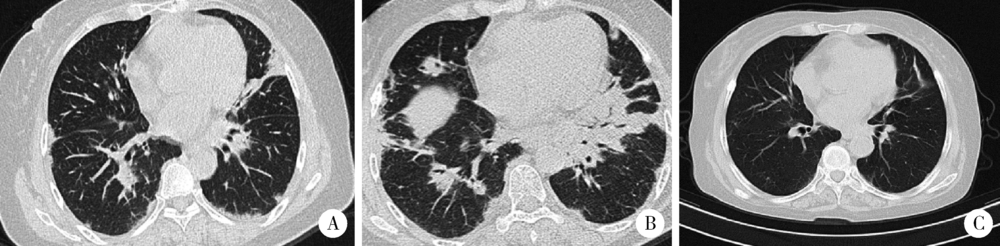
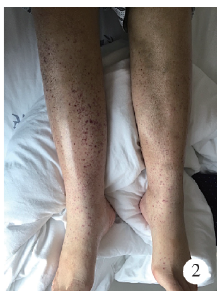
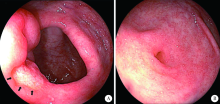
皮肌炎合并IgA血管炎1例
徐婧1,徐静2,李鹤3,唐杰4,舒建龙4,张婧1,石连杰1,李胜光1,△( )
)
- 1. 北京大学国际医院 风湿免疫科,北京 102206
2. 北京大学国际医院 肾内科, 北京 102206
3. 北京大学国际医院 呼吸与危重症医学科,北京 102206
4. 广西国际壮医医院风湿免疫科,南宁 530201
Dermatomyositis combined with IgA vasculitis: A case report
Jing XU1,Jing XU2,He LI3,Jie TANG4,Jian-long SHU4,Jing ZHANG1,Lian-jie SHI1,Sheng-guang LI1,△()
- 1. Department of Rheumatology and Immunology, Peking University International Hospital, Beijing 102206, China
2. Department of Nephrology, Peking University International Hospital, Beijing 102206, China
3. Department of Respiratory and Critical Care Medicine, Peking University International Hospital, Beijing 102206, China
4. Department of Rheumatology and Immunology, Guangxi International Zhuang Medicine Hospital, Nanning 530201, China
中图分类号:
- R593.26






| [1] | Russo RAG, Katsicas MM, Dávila M , et al. Cholestasis in juve-nile dermatomyositis: report of three cases[J]. Arthritis Rheum, 2001,44(5):1139-1142. |
| [2] | Ueda H, Miyazaki Y, Tsuboi N , et al. Clinical and pathological characteristics of elderly Japanese patients with IgA Vasculitis with nephritis: a case series[J]. Intern Med, 2019,58(1):31-38. |
| [3] | Tan J, Tang Y, Xu Y , et al. The clinicopathological characteristics of Henoch-Schonlein purpura nephritis with presentation of nephrotic syndrome [J]. Kidney Blood Press Res, 2019,44(4):754-764. |
| [4] | Chua JS, Zandbergen M, Wolterbeek R , et al. Complement-mediated microangiopathy in IgA nephropathy and IgA vasculitis with nephritis[J]. Mod Pathol, 2019,32(8):1147-1157. |
| [5] | Lin Q, Li X . Children with Henoch-Schonlein purpura with low complement levels: follow-up for >6 years[J]. Pediatr Nephrol, 2017,32(7):1279. |
| [6] | Yu JH, Lee KB, Lee JE , et al. A case of elderly-onset crescentic Henoch-Schonlein purpura nephritis with hypocomplementemia and positive MPO-ANCA[J]. J Korean Med Sci, 2012,27(8):957-960. |
| [7] | Lin Q, Min Y, Li Y , et al. Henoch-Schonlein purpura with hypocomplementemia[J]. Pediatr Nephrol, 2012,27(5):801-806. |
| [8] | Motoyama O, Iitaka K . Henoch-Schonlein purpura with hypocomplementemia in children[J]. Pediatr Int, 2005,47(1):39-42. |
| [9] | Garcia-Fuentes M, Martin A, Chantler C , et al. Serum complement components in Henoch-Schonlein purpura[J]. Arch Dis Child, 1978,53(5):417-419. |
| [10] | Zhang Y, Huang X . Gastrointestinal involvement in Henoch-Schonlein purpura[J]. Scand J Gastroenterol, 2008,43(9):1038-1043. |
| [11] | Sasaki K, Nukuda Y, Masuda T , et al. Endoscopically and histologically documented gastrointestinal lesions in an adult patient with Henoch-Schonlein purpura[J]. Endoscopy, 1994,26(7):629-630. |
| [12] | Basu R . Perforation of the bowel in Henoch-Schonlein purpura[J]. Arch Dis Child, 1959,34:342-343. |
| [13] | Emanuel B, Lieberman AD, Rosen S . Intussusception due to Henoch-Schonlein purpura. Case reports and review of the literature[J]. Ill Med J, 1962,122:162-167. |
| [14] | Nakamura A, Fuchigami T, Inamo Y . Protein-losing enteropathy associated with Henoch-Schonlein purpura[J]. Pediatr Rep, 2010,2(2):e20. |
| [15] | Louie CY, Gomez AJ, Sibley RK , et al. Histologic features of gastrointestinal tract biopsies in IgA vasculitis (Henoch-Schonlein purpura)[J]. Am J Surg Pathol, 2018,42(4):529-533. |
| [16] | Han Y, Jin SY, Kim DW , et al. Endoscopic and microscopic findings of gastrointestinal tract in Henoch-Schonlein purpura: Single institute experience with review of literature[J]. Medicine (Baltimore), 2019,98(20):e15643. |
| [17] | Akkari I, Mrabet S, Ben Jazia E . Gastrointestinal biopsy in Henoch-Schonlein purpura: A great diagnostic contribution[J]. Eur J Case Rep Intern Med, 2017,4(9):000662. |
| [18] | Yen T, Huang J, Chen C . Unexpected IgA nephropathy during the treatment of a young woman with idiopathic dermatomyositis: case report and review of the literature[J]. J Nephrol, 2003,16(1):148-153. |
| [19] | 舒晓明, 卢昕, 王国春 . 中国人多发性肌炎/皮肌炎合并肾脏损害的临床特点(附文献复习)[J]. 中日友好医院学报, 2017,31(2):67-70. |
| [20] |
钱莹, 任红, 陈晓农 , 等. 多发性肌炎和皮肌炎的肾脏损害分析[J]. 上海交通大学学报(医学版), 2011,31(4):451-454.
doi: 10.3969/j.issn.1674-8115.2011.04.015 |
| [21] | Georgaki-Angelaki E, Kostaridou S, Lourida A , et al. Abrupt and durable remission of Henoch-Schonlein purpura nephritis with cyclosporine A[J]. NDT Plus, 2008,1(5):300-302. |
| [1] | 赵亚云, 倪梦凡, 李雪, 王蓓, 程功, 何菁, 金月波. 利妥昔单抗治疗原发性干燥综合征肾损害的临床疗效和安全性[J]. 北京大学学报(医学版), 2025, 57(6): 1051-1060. |
| [2] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [3] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
| [4] | 丁艳, 李超然, 黄文生, 朱林忠, 王丽芳, 马豆豆, 张娟, 石连杰. 有肾脏意义单克隆免疫球蛋白血症继发lgA血管炎并导致小肠坏死1例[J]. 北京大学学报(医学版), 2024, 56(6): 1101-1105. |
| [5] | 魏慧,次旦央宗,益西拉姆,白玛央金. 高原地区不同类型过敏性紫癜藏族患者发病的相关危险因素[J]. 北京大学学报(医学版), 2023, 55(5): 923-928. |
| [6] | 时云飞,王豪杰,刘卫平,米岚,龙孟平,刘雁飞,赖玉梅,周立新,刁新婷,李向红. 血管免疫母细胞性T细胞淋巴瘤临床与分子病理学特征分析[J]. 北京大学学报(医学版), 2023, 55(3): 521-529. |
| [7] | 李挺. 建设当代临床病理学科[J]. 北京大学学报(医学版), 2023, 55(2): 197-200. |
| [8] | 周桥. 肿瘤病理学研究的进展和展望[J]. 北京大学学报(医学版), 2023, 55(2): 201-209. |
| [9] | 沈棋,刘亿骁,何群. 肾黏液样小管状和梭形细胞癌的临床病理特点及预后[J]. 北京大学学报(医学版), 2023, 55(2): 276-282. |
| [10] | 侯卫华,宋书杰,石中月,金木兰. 幽门螺杆菌阴性早期胃癌的临床病理特征[J]. 北京大学学报(医学版), 2023, 55(2): 292-298. |
| [11] | 刘菊梅,梁丽,张继新,戎龙,张梓怡,吴悠,赵旭东,李挺. 411例早期胃癌及癌前病变内镜黏膜下剥离术标本的病理学评估[J]. 北京大学学报(医学版), 2023, 55(2): 299-307. |
| [12] | 农琳,王微,梁丽,李东,李鑫,李挺. 母细胞性浆样树突细胞肿瘤13例临床病理学特征[J]. 北京大学学报(医学版), 2023, 55(2): 308-314. |
| [13] | 熊焰,张波,聂立功,吴世凯,赵虎,李东,邸吉廷. 胸部SMARCA4缺失性未分化肿瘤的病理诊断与联合免疫检测点抑制剂治疗[J]. 北京大学学报(医学版), 2023, 55(2): 351-356. |
| [14] | 哈雪梅,姚永正,孙莉华,辛春杨,熊焰. 实性肺胎盘样变形1例及文献复习[J]. 北京大学学报(医学版), 2023, 55(2): 357-361. |
| [15] | 宁博涵,张青霞,杨慧,董颖. 伴间质细胞增生、玻璃样变性及索状结构的子宫内膜样腺癌1例[J]. 北京大学学报(医学版), 2023, 55(2): 366-369. |
|
||
