北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (1): 167-174. doi: 10.19723/j.issn.1671-167X.2021.01.025
后路短节段跨伤椎椎弓根螺钉固定治疗胸腰段爆裂骨折术后再发后凸的危险因素
侯国进,周方( ),田耘,姬洪全,张志山,郭琰,吕扬,杨钟玮,张雅文
),田耘,姬洪全,张志山,郭琰,吕扬,杨钟玮,张雅文
- 北京大学第三医院骨科, 北京 100191
Risk factors of recurrent kyphosis in thoracolumbar burst fracture patients treated by short segmental pedicle screw fixation
HOU Guo-jin,ZHOU Fang(),TIAN Yun,JI Hong-quan,ZHANG Zhi-shan,GUO Yan,LV Yang,YANG Zhong-wei,ZHANG Ya-wen
- Department of Orthopaedic Surgery, Peking University Third Hospital, Beijing 100191, China
摘要:
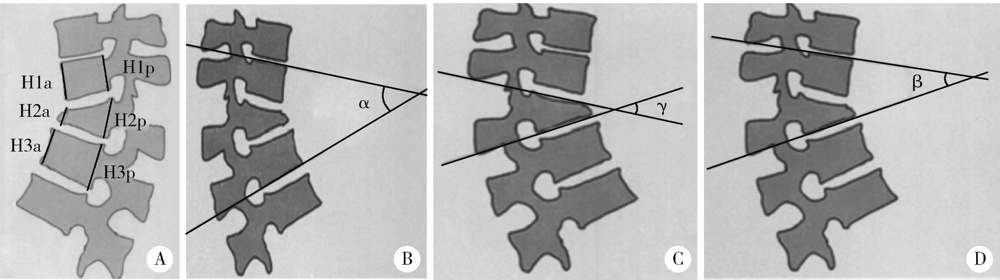
目的: 探索后路短节段跨伤椎椎弓根螺钉固定治疗胸腰段爆裂骨折内固定物取出术后再发后凸的危险因素。方法: 回顾性分析北京大学第三医院2010年1月至2017年12月诊治的无神经功能损害的单节段胸腰段爆裂骨折患者的临床资料,共有144例患者纳入该研究。所有患者均采用跨伤椎椎弓根螺钉固定,其中男性74例,女性70例;平均年龄(39.1±13.2)岁。伤椎分布在T12(42例)、L1(72例)和L2(30例),骨折类型为A3(90例)、B1(25例)和B2(29例)。根据取出内固定物后末次随访矫正度丢失是否>5°,将患者分为再发后凸组和无再发后凸组,再发后凸组共纳入92例,无再发后凸组共纳入52例。利用SPSS 26.0软件进行单因素组间比较及Logistic回归分析。结果: 平均随访时间28(20~113)个月,分别于术前、术后3 d、术后12个月及末次随访对患者影像学指标进行测量并对比分析。伤椎前缘高度、局部后凸角、伤椎楔形角、Gardner畸形等指标术后较术前均有明显改善(P<0.05),但在术后1年随访时均有不同程度的丢失;伤椎前缘高度和伤椎楔形角不再因取钉发生变化,而局部后凸角和Gardner畸形在取钉术后仍出现后凸加重(P<0.05);伤椎上、下椎间盘高度随访过程中出现不同程度的塌陷。单因素分析可见,再发后凸组和无再发后凸组患者的性别、年龄(36.9岁 vs. 43.0岁)、上位椎间盘损伤与否、CT值(174 vs. 160)、术前节段后凸角(16.6° vs. 13.3°)、术前伤椎楔形角(16.7° vs. 13.6°)、术前Gardner畸形(19.1° vs. 15.2°)及术前椎体前缘的高度比(0.65 vs. 0.71)差异具有统计学意义(P<0.05)。Logistics回归分析提示,男性(OR: 2.88,95%CI:1.196~6.933)、上位椎间盘损伤(OR: 2.962,95%CI:1.062~8.258)及术前伤椎楔形角是短节段跨伤椎椎弓根螺钉固定治疗胸腰段爆裂骨折取出内固定物后再发后凸的危险因素(P<0.05)。结论: 胸腰段骨折患者经后路短节段跨伤椎内固定能取得满意的术后即刻效果,但随访过程中可能会发生一定程度的矫正角度丢失,男性、上位椎间盘损伤及术前伤椎楔形角是内固定物取出后再发后凸的危险因素。
中图分类号:
- R683.2


| [1] |
Wood KB, Bohn D, Mehbod A. Anterior versus posterior treatment of stable thoracolumbar burst fractures without neurologic deficit: A prospective, randomized study[J]. J Spinal Disord Tech, 2005,18:S15-S23.
doi: 10.1097/01.bsd.0000132287.65702.8a pmid: 15699801 |
| [2] |
Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: An overview[J]. Indian J Orthop, 2015,49(1):72-82.
doi: 10.4103/0019-5413.143914 pmid: 25593358 |
| [3] | 伍骥, 郑超, 黄蓉蓉. 重新认识胸腰段脊柱骨折的诊断和治疗[J]. 中国骨与关节杂志, 2016,5(6):401-404. |
| [4] |
Pellise F, Barastegui D, Hernandez-Fernandez A, et al. Viability and long-term survival of short-segment posterior fixation in thoracolumbar burst fractures[J]. Spine J, 2015,15(8):1796-1803.
doi: 10.1016/j.spinee.2014.03.012 pmid: 24642054 |
| [5] |
Lee MC, Solomito M, Patel A. Supine magnetic resonance imaging Cobb measurements for idiopathic scoliosis are linearly related to measurements from standing plain radiographs[J]. Spine(Phila Pa 1976), 2013,38(11):E656-E661.
doi: 10.1097/BRS.0b013e31828d255d |
| [6] |
Wang XY, Dai LY, Xu HZ, et al. Kyphosis recurrence after posterior short-segment fixation in thoracolumbar burst fractures[J]. J Neurosurg Spine, 2008,8(3):246-254.
doi: 10.3171/SPI/2008/8/3/246 pmid: 18312076 |
| [7] |
Zou D, Li WS, Deng C, et al. The use of CT Hounsfield unit values to identify the undiagnosed spinal osteoporosis in patients with lumbar degenerative diseases[J]. Eur Spine J, 2019,28(8):1758-1766.
doi: 10.1007/s00586-018-5776-9 pmid: 30306332 |
| [8] |
Sander AL, Laurer H, Lehnert T, et al. A clinically useful classification of traumatic intervertebral disk lesions[J]. AJR Am J Roentgenol, 2013,200(3):618-623.
doi: 10.2214/AJR.12.8748 pmid: 23436852 |
| [9] |
McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures[J]. Spine, 1994,19(15):1741-1744.
doi: 10.1097/00007632-199408000-00014 pmid: 7973969 |
| [10] |
Roy-Camille R, Saillant G, Mazel C. Plating of thoracic, thoracolumbar, and lumbar injuries with pedicle screw plates[J]. Orthop Clin North Am, 1986,17(1):147-159.
pmid: 3945476 |
| [11] |
Cho DY, Lee WY, Sheu PC. Treatment of thoracolumbar burst fractures with polymethyl methacrylate vertebroplasty and short-segment pedicle screw fixation[J]. Neurosurgery, 2003,53(6):1354-1361.
doi: 10.1227/01.neu.0000093200.74828.2f pmid: 14633301 |
| [12] |
Kim JY, Ryu DS, Paik HK, et al. Paraspinal muscle, facet joint, and disc problems: Risk factors for adjacent segment degeneration after lumbar fusion[J]. Spine J, 2016,16(7):867-875.
doi: 10.1016/j.spinee.2016.03.010 pmid: 26970600 |
| [13] |
Furderer S, Wenda K, Thiem N, et al. Traumatic intervertebral disc lesion: Magnetic resonance imaging as a criterion for or against intervertebral fusion[J]. Eur Spine J, 2001,10(2):154-163.
doi: 10.1007/s005860000238 pmid: 11345638 |
| [14] |
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures: A five to seven years prospective randomized study[J]. J Bone Joint Surg Am, 2009,91(5):1033-1041.
doi: 10.2106/JBJS.H.00510 pmid: 19411450 |
| [15] |
Kerttula LI, Serlo WS, Tervonen OA, et al. Post-traumatic findings of the spine after earlier vertebral fracture in young patients: clinical and MRI study[J]. Spine, 2000,25(9):1104-1108.
doi: 10.1097/00007632-200005010-00011 pmid: 10788855 |
| [16] |
Chen JX, Xu DL, Sheng SR, et al. Risk factors of kyphosis recurrence after implant removal in thoracolumbar burst fractures following posterior short-segment fixation[J]. Int Orthop, 2016,40(6):1253-1260.
doi: 10.1007/s00264-016-3180-9 pmid: 27116190 |
| [17] |
Alanay A, Acaroglu E, Yazici M, et al. Short-segment pedicle instrumentation of thoracolumbar burst fractures: does transpedicular intracorporeal grafting prevent early failure?[J]. Spine, 2001,26(2):213-217.
doi: 10.1097/00007632-200101150-00017 pmid: 11154543 |
| [18] |
Jun DS, Shin WJ, An BK, et al. The relationship between the progression of kyphosis in stable thoracolumbar fractures and magnetic resonance imaging findings[J]. Asian Spine J, 2015,9(2):170-177.
doi: 10.4184/asj.2015.9.2.170 pmid: 25901226 |
| [19] |
Mahar A, Kim C, Wedemeyer M, et al. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture[J]. Spine, 2007,32(14):1503-1507.
doi: 10.1097/BRS.0b013e318067dd24 pmid: 17572619 |
| [20] | 魏富鑫, 刘少喻, 赵卫东, 等. 胸腰椎爆裂性骨折伤椎固定的生物力学研究[J]. 中华创伤骨科杂志, 2006,8(9):857-860. |
| [21] |
Li K, Zhang W, Liu D, et al. Pedicle screw fixation combined with intermediate screw at the fracture level for treatment of thoracolumbar fractures: A meta-analysis[J]. Medicine (Baltimore), 2016,95(33):e4574.
doi: 10.1097/MD.0000000000004574 |
| [22] |
Rajasekaran S, Maheswaran A, Aiyer SN, et al. Prediction of posterior ligamentous complex injury in thoracolumbar fractures using non-MRI imaging techniques[J]. Int Orthop, 2016,40(6):1075-1081.
doi: 10.1007/s00264-016-3151-1 pmid: 26983409 |
| [23] | 唐一村, 林本丹, 林慰光, 等. X线片和CT影像对胸腰椎后方韧带复合体损伤的诊断意义[J]. 中国脊柱脊髓杂志, 2016,26(9):801-806. |
| [24] |
Machino M, Yukawa Y, Ito K, et al. Posterior ligamentous complex injuries are related to fracture severity and neurological damage in patients with acute thoracic and lumbar burst fractures[J]. Yonsei Med J, 2013,54(4):1020-1025.
doi: 10.3349/ymj.2013.54.4.1020 pmid: 23709440 |
| [25] |
McLain RF. The biomechanics of long versus short fixation for thoracolumbar spine fractures[J]. Spine(Phila Pa 1976), 2006,31(11 Suppl):S70-S79.
doi: 10.1097/01.brs.0000218221.47230.dd |
| [26] | 张阳, 张志成, 李放, 等. 后方韧带复合体损伤在胸腰段骨折患者评估中的意义[J]. 中国骨与关节杂志, 2016,5(6):425-428. |
| [27] | 张亚军, 方礼明, 张军, 等. 经椎旁肌间隙短节段椎弓根钉固定治疗伴后方韧带复合体损伤的胸腰椎骨折[J]. 中华创伤骨科杂志, 2013,15(12):1049-1053. |
| [28] |
何海潮, 吕晓强, 张永进. 短节段经皮微创与传统椎弓根螺钉内固定治疗伴后方韧带复合体损伤的胸腰椎骨折的比较[J]. 中国骨伤, 2016,29(4):329-334.
doi: 10.3969/j.issn.1003-0034.2016.04.009 |
| [29] |
Parker JW, Lane JR, Karaikovic EE, et al. Successful shortsegment instrumentation and fusion for thoracolumbar spine fractures: A consecutive 41/ 2-year series[J]. Spine, 2000,25(9):1157-1170.
doi: 10.1097/00007632-200005010-00018 pmid: 10788862 |
| [30] |
Rihn JA, Anderson DT, Harris E, et al. A review of the TLICS system: A novel, user-friendly thoracolumbar trauma classification system[J]. Acta Orthop, 2008,79(4):461-466.
doi: 10.1080/17453670710015436 pmid: 18766477 |
| [31] |
Kaul R, Chhabra HS, Vaccaro AR, et al. Reliability assessment of AOSpine thoracolumbar spine injury classification system and thoracolumbar injury classification and severity score (TLICS) for thoracolumbar spine injuries: results of a multicentre study[J]. Eur Spine J, 2017,26(5):1470-1476.
doi: 10.1007/s00586-016-4663-5 pmid: 27334493 |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 魏竞尧, 叶菊香, 周美玲, 付伟伟, 刘鑫, 翟康乐, 石岩岩, 丁士刚, 张静. 原发性胃淋巴瘤的内镜特征分析及疗效预测[J]. 北京大学学报(医学版), 2026, 58(2): 342-350. |
| [3] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [4] | 李伟浩, 张学民, 李伟, 张韬, 张小明. 胸主动脉腔内修复术左肱动脉穿刺点使用血管缝合器处理的临床效果[J]. 北京大学学报(医学版), 2026, 58(2): 388-392. |
| [5] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [6] | 肖晓笛, 夏有辰, 柳剑英, 付鹏. 左侧胸锁乳突肌间血管内乳头状内皮增生1例[J]. 北京大学学报(医学版), 2025, 57(5): 1002-1004. |
| [7] | 侯卫华, 宋书杰, 石中月, 刘露, 金木兰. 食管胃结合部具有显著空泡状核特征的神经内分泌癌1例[J]. 北京大学学报(医学版), 2025, 57(5): 1005-1009. |
| [8] | 宋畅, 冯琦琛, 杨广鑫, 刘启佳, 王昌明, 李选. 液-固兼用曲张静脉栓塞技术联合专用支架在经颈内静脉肝内门体分流术中的应用[J]. 北京大学学报(医学版), 2025, 57(5): 1010-1013. |
| [9] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [10] | 胡枫艺, 孟庆阳, 陈拿云, 王佳宁, 刘振龙, 马勇, 杨渝平, 龚熹, 王成, 刘平, 史尉利. 镜下内侧髌股复合体重建治疗伴高级别滑车发育不良复发性髌骨脱位的临床疗效[J]. 北京大学学报(医学版), 2025, 57(5): 947-955. |
| [11] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [12] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [13] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [14] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [15] | 卞雯, 周文君, 吴天晨, 朱培静, 陈一诺, 原鹏波, 王学举, 王颖, 魏瑗, 赵扬玉. 单绒毛膜双羊膜囊双胎妊娠双胎之一胎死宫内对妊娠结局的影响[J]. 北京大学学报(医学版), 2025, 57(3): 592-598. |
|
||
