北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (1): 204-209. doi: 10.19723/j.issn.1671-167X.2021.01.031
十二指肠乳头息肉良、恶性病变比较及活检准确性
王迎春,黄永辉( ),常虹,姚炜,闫秀娥,李柯,张耀鹏,郑炜
),常虹,姚炜,闫秀娥,李柯,张耀鹏,郑炜
- 北京大学第三医院消化科,北京 100191
Characteristics of benign and malignant lesions of ampullary polyps and the accuracy of forceps biopsy
WANG Ying-chun,HUANG Yong-hui(),CHANG Hong,YAO Wei,YAN Xiu-e,LI Ke,ZHANG Yao-peng,ZHENG Wei
- Department of Gastroenterology, Peking University Third Hospital, Beijing 100191, China
摘要:
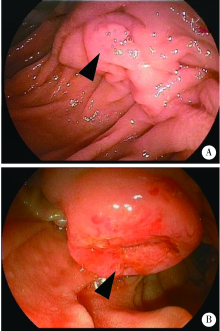
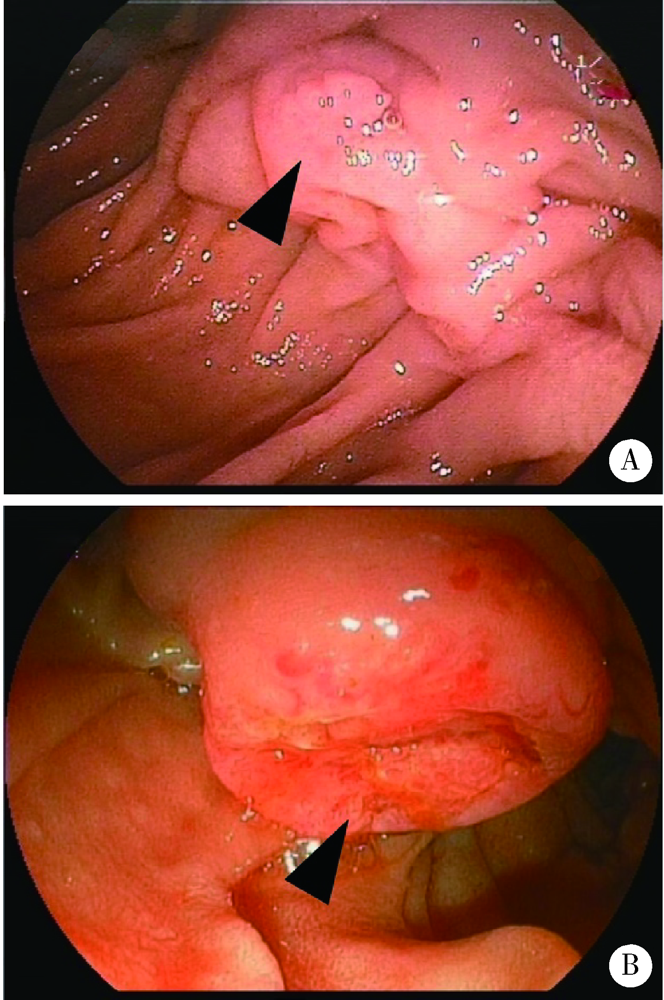
目的: 比较十二指肠乳头息肉良、恶性病变的内镜下及临床特点,探究内镜下预判十二指肠乳头腺瘤癌变的可行性,并评估内镜下乳头活检组织病理学诊断的准确性。方法: 选择2009年1月至2019年5月在北京大学第三医院内镜中心接受内镜下十二指肠乳头切除术(endoscopic papillectomy,EP)患者的临床资料及内镜图片,分为良性病变及癌两组,进行对比分析。结果: 研究共纳入42例患者,年龄35~83岁,50岁以上患者占83.3%(35/42)。42例患者中,炎性息肉2例(4.8%),神经内分泌瘤1例(2.4%),增生性息肉1例(2.4%),Ⅰ级腺瘤5例(11.9%),Ⅱ级腺瘤10例(23.8%),Ⅲ级腺瘤4例(9.5%),癌19例(45.2%),腺瘤和癌共占90.5%。良性病变(炎性息肉及腺瘤)组平均年龄(56.7±9.2) 岁,癌组(66.0±9.8) 岁,两组间差异有统计学意义(P=0.004)。癌[(2.3±0.8) cm]的直径显著大于良性病变[(1.6±0.6) cm, P=0.002]。良性病变均为山田(Yamada)Ⅰ型(57.1%)或Ⅱ型(42.9%)病变,而癌组山田Ⅰ型(36.8%)、Ⅱ型(31.6%)比例较低,31.5%为山田Ⅲ型病变。两组间山田分型差异有统计学意义,癌组带蒂倾向明显(P=0.046)。良性病变多与周围分界清楚(18/21,85.7%),而癌组分界多不明显,仅2例(10.5%)具有清晰的界限,两组间差异具有统计学意义(P<0.001)。息肉表面颜色(P=0.353)、表面形态(P=0.324)两组间差异无统计学意义。将差异有统计学意义的年龄、病变大小、山田分型、与周围界限是否清晰纳入Logistic回归分析,结果显示年龄(OR=1.186,95%CI: 1.025~1.373,P=0.022)、与周围是否有清晰界限(OR=66.218,95%CI: 3.421~1 281.840,P=0.006)为乳头癌变风险的独立预判因素。19例癌患者中,术前仅2例(10.5%)活检诊断提示癌。17例癌(17/19,89.5%)、4例Ⅱ级腺瘤(4/10,40%)术前病理均低于实际病理分级,占病例总数的55.3%(21/38)。结论: 十二指肠乳头息肉以腺瘤及癌为主,高龄、与周围黏膜界限不清为十二指肠乳头肿瘤癌变的独立预判危险因素,单纯活检组织病理诊断对乳头肿瘤良、恶性的鉴别意义有限。
中图分类号:
- R574.51


| [1] |
Ridtitid W, Tan D, Schmidt SE, et al. Endoscopic papillectomy: risk factors for incomplete resection and recurrence during long-term follow-up[J]. Gastrointest Endosc, 2014,79(2):289-296.
pmid: 24094466 |
| [2] |
Ridtitid W, Schmidt SE, Al-Haddad MA, et al. Performance characteristics of EUS for locoregional evaluation of ampullary lesions[J]. Gastrointest Endosc, 2015,81(2):380-388.
doi: 10.1016/j.gie.2014.08.005 pmid: 25293823 |
| [3] |
Kang SH, Kim KH, Kim TN, et al. Therapeutic outcomes of endoscopic papillectomy for ampullary neoplasms: retrospective analysis of a multicenter study[J]. BMC Gastroenterol, 2017,17(1):69.
doi: 10.1186/s12876-017-0626-5 pmid: 28558658 |
| [4] |
El H, Coté GA. Endoscopic diagnosis and management of ampullary lesions[J]. Gastrointest Endosc Clin N Am, 2013,23(1):95-109.
doi: 10.1016/j.giec.2012.10.004 pmid: 23168121 |
| [5] | 顾宗廷, 张永杰. 十二指肠乳头肿瘤的诊断与外科治疗[J]. 国际消化病杂志, 2015,35(6):428-435. |
| [6] |
Chathadi KV, Khashab MA, Acosta RD, et al. The role of endoscopy in ampullary and duodenal adenomas[J]. Gastrointest Endosc, 2015,82(5):773-781.
doi: 10.1016/j.gie.2015.06.027 pmid: 26260385 |
| [7] | 陆鉴, 陆文洁, 吴育连. 十二指肠乳头肿瘤的临床特点及诊治分析[J]. 中华外科杂志, 2016,54(3):187-190. |
| [8] |
Attila T, Parlak E, Alper E, et al. Endoscopic papillectomy of benign ampullary lesions: Outcomes from a multicenter study[J]. Turk J Gastroenterol, 2018,29(3):325-334.
doi: 10.5152/tjg.2018.17378 pmid: 29755017 |
| [9] |
Wanders LK, East JE, Uitentuis SE, et al. Diagnostic performance of narrowed spectrum endoscopy, autofluorescence imaging, and confocal laser endomicroscopy for optical diagnosis of colonic polyps: a meta-analysis[J]. Lancet Oncol, 2013,14(13):1337-1347.
doi: 10.1016/S1470-2045(13)70509-6 pmid: 24239209 |
| [10] |
Kim HN, Kim KM, Shin JU, et al. Prediction of carcinoma after resection in subjects with ampullary adenomas on endoscopic biopsy[J]. J Clin Gastroenterol, 2013,47(4):346-351.
doi: 10.1097/MCG.0b013e318272f2ef pmid: 23442830 |
| [11] | 郝璐, 王伟, 施新岗, 等. 十二指肠乳头肿瘤内镜切除术的临床应用进展[J]. 中华消化内镜杂志, 2017,34(6):451-454. |
| [12] |
Wee E, Lakhtakia S, Gupta R, et al. The diagnostic accuracy and strength of agreement between endoscopic ultrasound and histopathology in the staging of ampullary tumors[J]. Indian J Gastroenterol, 2012,31(6):324-332.
doi: 10.1007/s12664-012-0248-3 pmid: 22996048 |
| [13] | 张荣春, 陈杰, 于卫华, 等. 十二指肠乳头肿瘤内镜切除术[J]. 中华消化内镜杂志, 2014,31(4):231-235. |
| [14] |
Bourgeois N, Dunham F, Verhest A, et al. Endoscopic biopsies of the papilla of Vater at the time of endoscopic sphincterotomy: difficulties in interpretation[J]. Gastrointest Endosc, 1984,30(3):163-166.
doi: 10.1016/s0016-5107(84)72357-1 pmid: 6735092 |
| [1] | 王海, 江一舟. 靶向血管治疗在乳腺癌精准治疗中的分子机制与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 251-256. |
| [2] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [3] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [4] | 李嘉临, 陈力侨, 唐家天, 吴艳, 王安强. 胃肝样腺癌转化治疗1例[J]. 北京大学学报(医学版), 2026, 58(2): 399-404. |
| [5] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [6] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [7] | 侯卫华, 宋书杰, 石中月, 刘露, 金木兰. 食管胃结合部具有显著空泡状核特征的神经内分泌癌1例[J]. 北京大学学报(医学版), 2025, 57(5): 1005-1009. |
| [8] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [9] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [10] | 刘杰, 马茗微, 王庆安, 石明, 尹金鹏, 王占平, 申静涛, 高献书. 基于锥形束CT的前列腺癌放射治疗两种体位固定方式摆位误差比较[J]. 北京大学学报(医学版), 2025, 57(4): 692-697. |
| [11] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [12] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [13] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [14] | 韩丹, 次仁央金, 李秋红, 李军. 高海拔地区结直肠良恶性肿瘤患者肠道菌群差异及其与低海拔地区正常人群的比较[J]. 北京大学学报(医学版), 2025, 57(3): 578-583. |
| [15] | 刘苗雨, 王思源, 裴林, 王殊. 同步应用戈舍瑞林对年轻乳腺癌患者新辅助化疗疗效的影响[J]. 北京大学学报(医学版), 2025, 57(2): 291-297. |
|
||
