北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (3): 460-466. doi: 10.19723/j.issn.1671-167X.2021.03.004
基于马尔可夫模型的社区人群心血管病筛查策略的效果评价
刘秋萍1,陈汐瑾2,王佳敏1,刘晓非2,司亚琴1,梁靖媛1,沈鹏3,林鸿波3,唐迅1,Δ( ),高培1,2,Δ()
),高培1,2,Δ()
- 1.北京大学公共卫生学院流行病与卫生统计学系,北京 100191
2.北京大学临床研究所真实世界证据评价中心,北京 100191
3.宁波市鄞州区疾病预防控制中心,浙江宁波 315101
Effectiveness of different screening strategies for cardiovascular diseases prevention in a community-based Chinese population: A decision-analytic Markov model
LIU Qiu-ping1,CHEN Xi-jin2,WANG Jia-min1,LIU Xiao-fei2,SI Ya-qin1,LIANG Jing-yuan1,SHEN Peng3,LIN Hong-bo3,TANG Xun1,Δ(),GAO Pei1,2,Δ()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Center for Real-world Evidence Evaluation, Peking University Clinical Research Institute, Beijing 100191, China
3. Yinzhou District Center for Disease Control and Prevention, Ningbo 315101, Zhejiang, China
摘要:
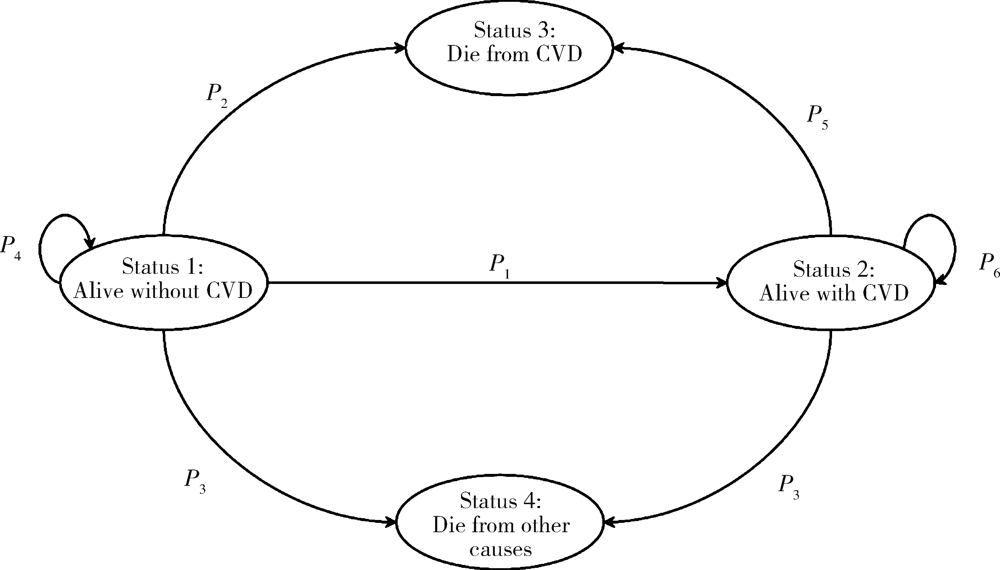
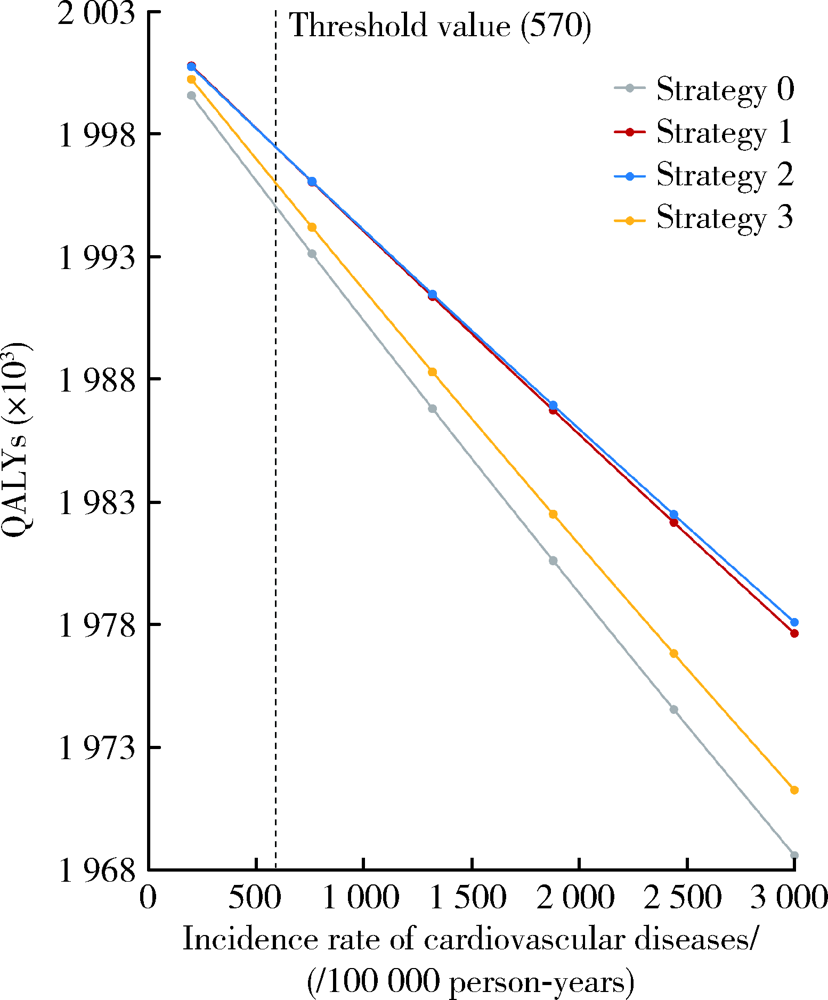
目的: 在中国鄞州电子健康档案研究(Chinese electronic health records research in Yinzhou, CHERRY)的队列人群中,评估我国不同指南最新推荐的心血管病筛查策略的效果。方法: 研究对象为2010年1月1日基线未患心血管病的40~74岁的202 179名我国沿海经济发达地区的社区人群。本研究比较的筛查策略包括:策略1,在40~74岁人群中采用2020年《中国心血管病一级预防指南》推荐的风险流程图的定性筛查策略;策略2,在40~74岁人群中采用2019年《中国心血管病风险评估和管理指南》推荐的中国动脉粥样硬化性心血管病风险预测研究(prediction for atherosclerotic cardiovascular disease risk in China, China-PAR)风险评估模型的定量筛查策略;策略3,在50~74岁人群中采用China-PAR模型的定量筛查策略。根据指南推荐,采用上述不同的筛查策略进行风险分层后,对中危及以上人群进行生活方式干预,对高危人群额外进行药物治疗干预。使用马尔可夫模型仿真,研究期限为10年,比较的效果指标包括获得的生命年、质量调整生命年(quality-adjusted life year, QALY)、可预防的心血管病发病数、心血管病死亡数与全因死亡数以及对应的需筛查人数。马尔可夫模型的参数主要来源于CHERRY队列人群、公开发表的中国人群研究数据、Meta分析及系统综述。采用单因素敏感性分析探讨一般人群心血管病发病率的不确定性对结果的影响,采用概率敏感性分析探讨风险比参数的不确定性。结果: 与不筛查相比,采用策略1、2、3获得的增量QALYs分别为1 433年[95%不确定性区间(uncertainty interval, UI): 969~1 831]、1 401年(95%UI: 936~1 807)和716年(95%UI: 265~1 111),每获得1个QALY的需筛查人数分别为141人(95%UI: 110~209)、144人(95%UI: 112~216)和198人(95%UI: 127~529)。在40~74岁人群采用风险流程图的定性筛查策略与China-PAR模型的定量筛查策略效果相似,采用China-PAR模型的定量筛查策略在40~74岁人群进行筛查比在50~74岁人群筛查能够获得更多的健康收益。单因素敏感性分析和概率敏感性分析的结果与主要分析结果一致。结论: 在我国沿海经济发达地区的40岁以上社区人群中开展心血管病筛查能够获得更多的健康收益,采用2020年《中国心血管病一级预防指南》推荐的风险流程图的定性筛查策略与2019年《中国心血管病风险评估和管理指南》推荐的China-PAR模型的定量筛查策略可获得相似的筛查效果。
中图分类号:
- R181.32

| [1] | Owen AJ, Reid CM. Systematic versus opportunistic risk assessment for the primary prevention of cardiovascular disease[J]. Cochrane Database Syst Rev, 2016,2016(1): CD010411. |
| [2] |
Brainin M, Sliwa K. WSO and WHF joint position statement on population-wide prevention strategies[J]. Lancet, 2020,396(10250):533-534.
doi: 10.1016/S0140-6736(20)31752-9 |
| [3] | 中国心血管病风险评估和管理指南编写联合委员会. 中国心血管病风险评估和管理指南[J]. 中华预防医学杂志, 2019,53(1):13-35. |
| [4] | 中华医学会心血管病学分会, 中国康复医学会心脏预防与康复专业委员会, 中国老年学和老年医学会心脏专业委员会, 等. 中国心血管病一级预防指南[J]. 中华心血管病杂志, 2020,48(12):1000-1038. |
| [5] |
Xu G, Ma M, Liu X, et al. Is there a stroke belt in China and why?[J]. Stroke, 2013,44(7):1775-1783.
doi: 10.1161/STROKEAHA.113.001238 |
| [6] | 司亚琴, 唐迅, 张杜丹, 等. 北方农村人群心血管病一级预防筛查策略的评价[J]. 北京大学学报(医学版), 2018,50(3):443-449. |
| [7] | 刘秋萍, 高培, 唐迅, 等. 马尔可夫模型在流行病学筛查成本效果分析中的应用[J]. 中华流行病学杂志, 2021,42(4):728-734. |
| [8] |
Gu D, He J, Coxson PG, et al. The cost-effectiveness of low-cost essential antihypertensive medicines for hypertension control in China: A modelling study[J]. PLoS Med, 2015,12(8):e1001860.
doi: 10.1371/journal.pmed.1001860 |
| [9] |
Lin H, Tang X, Shen P, et al. Using big data to improve cardiovascular care and outcomes in China: A protocol for the Chinese electronic health records research in Yinzhou (CHERRY) study[J]. BMJ Open, 2018,8(2):e019698.
doi: 10.1136/bmjopen-2017-019698 |
| [10] |
Zhang D, Tang X, Shen P, et al. Multimorbidity of cardiometabolic diseases: Prevalence and risk for mortality from one million Chinese adults in a longitudinal cohort study[J]. BMJ Open, 2019,9(3):e024476.
doi: 10.1136/bmjopen-2018-024476 |
| [11] | Ma C, Avenell A, Bolland M, et al. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: Systematic review and meta-analysis[J]. BMJ, 2017,359:j4849. |
| [12] |
Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases: A meta-analysis[J]. Circulation, 2012,126(18):2177-2183.
doi: 10.1161/CIRCULATIONAHA.112.121301 |
| [13] |
Lim SH, Tai BC, Yuan JM, et al. Smoking cessation and mortality among middle-aged and elderly Chinese in Singapore: the Singapore Chinese health study[J]. Tob Control, 2013,22(4):235-240.
doi: 10.1136/tobaccocontrol-2011-050106 pmid: 22170337 |
| [14] | Adler AJ, Taylor F, Martin N, et al. Reduced dietary salt for the prevention of cardiovascular disease[J]. Cochrane Database Syst Rev, 2014,2014(12): CD009217. |
| [15] |
Yusuf S, Lonn E, Pais P, et al. Blood-pressure and cholesterol lowering in persons without cardiovascular disease[J]. N Engl J Med, 2016,374(21):2032-2043.
doi: 10.1056/NEJMoa1600177 |
| [16] |
Shah AD, Langenberg C, Rapsomaniki E, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people[J]. Lancet Diabetes Endocrinol, 2015,3(2):105-113.
doi: 10.1016/S2213-8587(14)70219-0 |
| [17] |
Emerging Risk Factors Collaboration, Di Angelantonio E, Kaptoge S, et al. Association of cardiometabolic multimorbidity with mortality[J]. JAMA, 2015,314(1):52-60.
doi: 10.1001/jama.2015.7008 pmid: 26151266 |
| [18] | Kypridemos C, Allen K, Hickey G L, et al. Cardiovascular screening to reduce the burden from cardiovascular disease: Microsimulation study to quantify policy options[J]. BMJ, 2016,353:i2793. |
| [19] | 中国心血管病预防指南(2017)写作组, 中华心血管病杂志编辑委员会. 中国心血管病预防指南(2017)[J]. 中华心血管病杂志, 2018,46(1):10-25. |
| [20] |
Matsushita K, Coresh J, Sang Y, et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: A collaborative meta-analysis of individual participant data[J]. Lancet Diabetes Endocrinol, 2015,3(7):514-525.
doi: 10.1016/S2213-8587(15)00040-6 pmid: 26028594 |
| [21] |
Li X, Wu C, Lu J, et al. Cardiovascular risk factors in China: A nationwide population-based cohort study[J]. Lancet Public Health, 2020,5(12):e672-e681.
doi: 10.1016/S2468-2667(20)30191-2 |
| [22] |
Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines[J]. Circulation, 2019,140(11):e596-e646.
doi: 10.1161/CIR.0000000000000678 |
| [1] | 杨明佳, 吴姜雪, 王静, 刘扬, 李忠民, 李静静, 李宏田, 周玉博, 刘建蒙. 2019—2024年以行政辖区小学生人群为基础的近视情况调查[J]. 北京大学学报(医学版), 2026, 58(3): 513-519. |
| [2] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [3] | 陈楚云,孙蓬飞,赵静,贾佳,范芳芳,王春燕,李建平,姜一梦,霍勇,张岩. 北京社区人群促红细胞生成素相关因素及其与10年心血管疾病风险的关系[J]. 北京大学学报(医学版), 2023, 55(6): 1068-1073. |
| [4] | 张紫薇,花语蒙,刘爱萍. 中国中老年人群抑郁症状、缺血性心血管疾病10年风险对心血管疾病的联合影响[J]. 北京大学学报(医学版), 2023, 55(3): 465-470. |
| [5] | 张云静,乔丽颖,祁萌,严颖,亢伟伟,刘国臻,王明远,席云峰,王胜锋. 乳腺癌患者新发心血管疾病预测模型的建立与验证:基于内蒙古区域医疗数据[J]. 北京大学学报(医学版), 2023, 55(3): 471-479. |
| [6] | 张明露,刘秋萍,巩超,王佳敏,周恬静,刘晓非,沈鹏,林鸿波,唐迅,高培. 阿司匹林用于心血管病一级预防的不同策略比较:一项马尔可夫模型研究[J]. 北京大学学报(医学版), 2023, 55(3): 480-487. |
| [7] | 董尔丹. 心血管受体的信号转导与疾病[J]. 北京大学学报(医学版), 2022, 54(5): 796-802. |
| [8] | 巩超, 刘秋萍, 王佳敏, 刘晓非, 张明露, 杨瀚, 沈鹏, 林鸿波, 唐迅, 高培. 社区人群他汀干预策略预防心血管病效果的马尔可夫模型评价[J]. 北京大学学报(医学版), 2022, 54(3): 443-449. |
| [9] | 王佳敏,刘秋萍,张明露,巩超,刘舒丹,陈暐烨,沈鹏,林鸿波,高培,唐迅. 基于马尔可夫模型的社区人群糖尿病筛查预防心血管病的效果评价[J]. 北京大学学报(医学版), 2022, 54(3): 450-457. |
| [10] | 郭子宁, 梁志生, 周仪, 张娜, 黄捷. 基于国际疾病分类的心血管疾病亚型的基因组学研究[J]. 北京大学学报(医学版), 2021, 53(3): 453-459. |
| [11] | 陈家丽,金月波,王一帆,张晓盈,李静,姚海红,何菁,李春. 老年发病类风湿关节炎的临床特征及其心血管疾病危险因素分析:一项大样本横断面临床研究[J]. 北京大学学报(医学版), 2020, 52(6): 1040-1047. |
| [12] | 徐涛,韩敬丽,姚伟娟. 雄激素剥夺治疗相关心血管疾病的机制与临床对策[J]. 北京大学学报(医学版), 2020, 52(4): 607-609. |
| [13] | 刘欢,何映东,刘金波,黄薇,赵娜,赵红薇,周晓华,王宏宇. 血管健康指标对新发心脑血管事件的预测价值:北京血管健康分级标准的初步验证[J]. 北京大学学报(医学版), 2020, 52(3): 514-520. |
| [14] | 任川,吴晓月,赵威,陶立元,刘萍,高炜. 心肺适能对动脉粥样硬化性心血管疾病高危患者的保护作用[J]. 北京大学学报(医学版), 2020, 52(1): 152-157. |
| [15] | 王鹏,吴华,车颖,范东伟,刘珏,陶立元. 亚洲骨质疏松筛查工具在健康体检中的筛查准确性评价及适宜切点研究[J]. 北京大学学报(医学版), 2019, 51(6): 1085-1090. |
|
||
