北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (6): 1086-1093. doi: 10.19723/j.issn.1671-167X.2022.06.005
类风湿关节炎患者生活质量与疾病活动度的横断面研究
张警丰,金银姬,魏慧,姚中强,赵金霞*( )
)
- 北京大学第三医院风湿免疫科, 北京 100191
Cross-sectional study on quality of life and disease activity of rheumatoid arthritis patients
Jing-feng ZHANG,Yin-ji JIN,Hui WEI,Zhong-qiang YAO,Jin-xia ZHAO*()
- Department of Rheumatology and Immunology, Peking University Third Hospital, Beijing 100191, China
摘要:
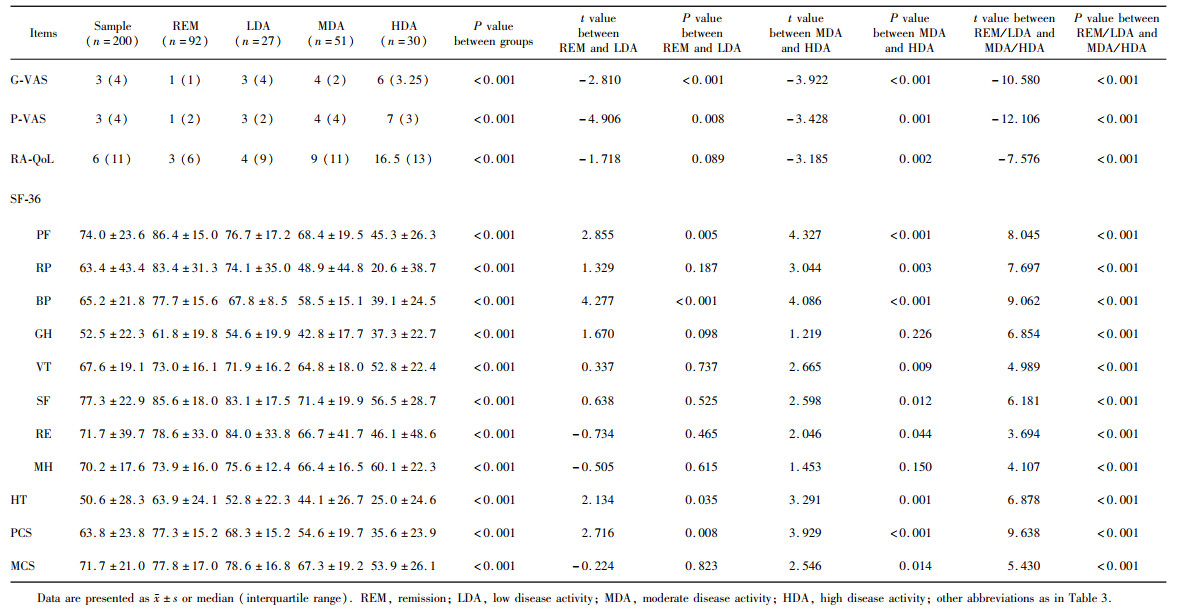
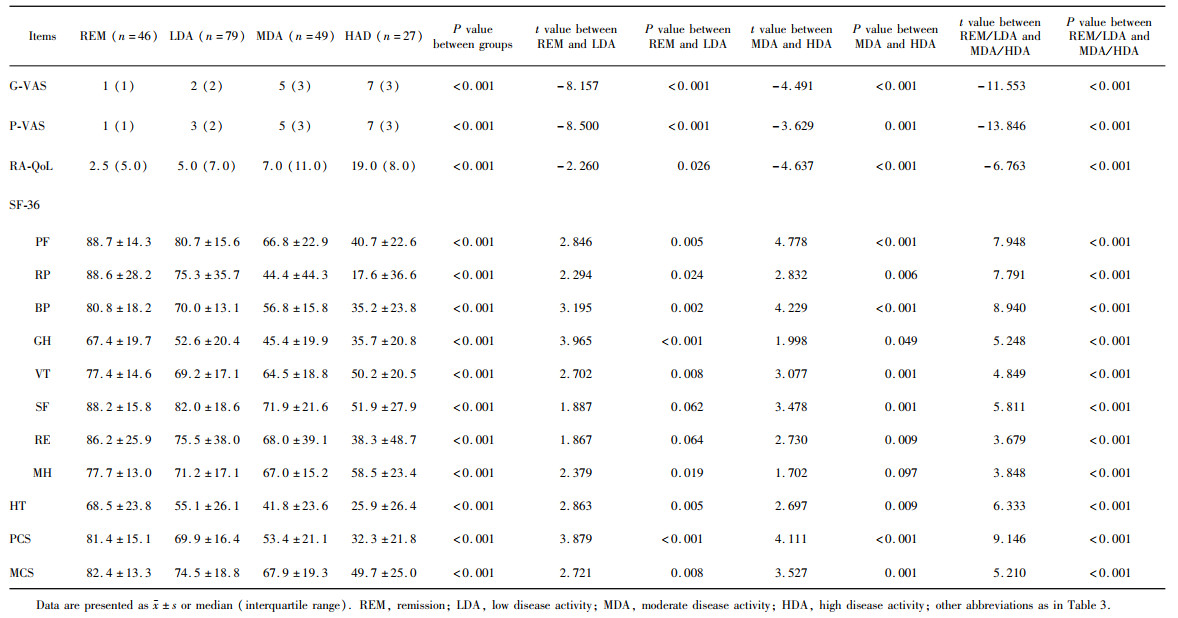
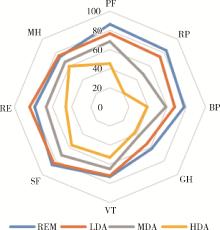
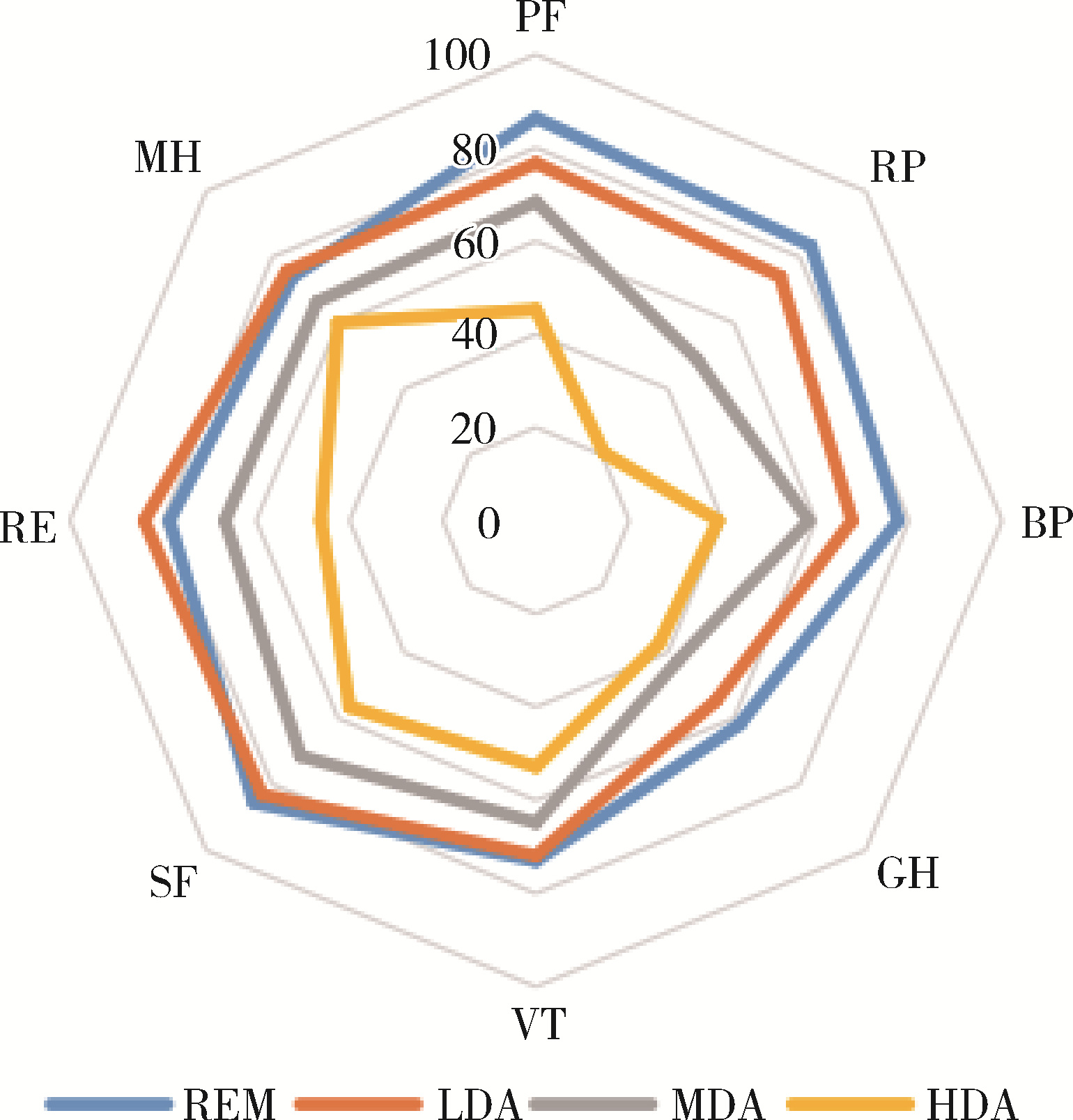
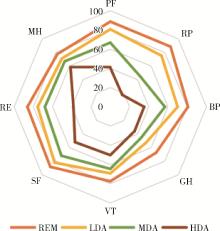
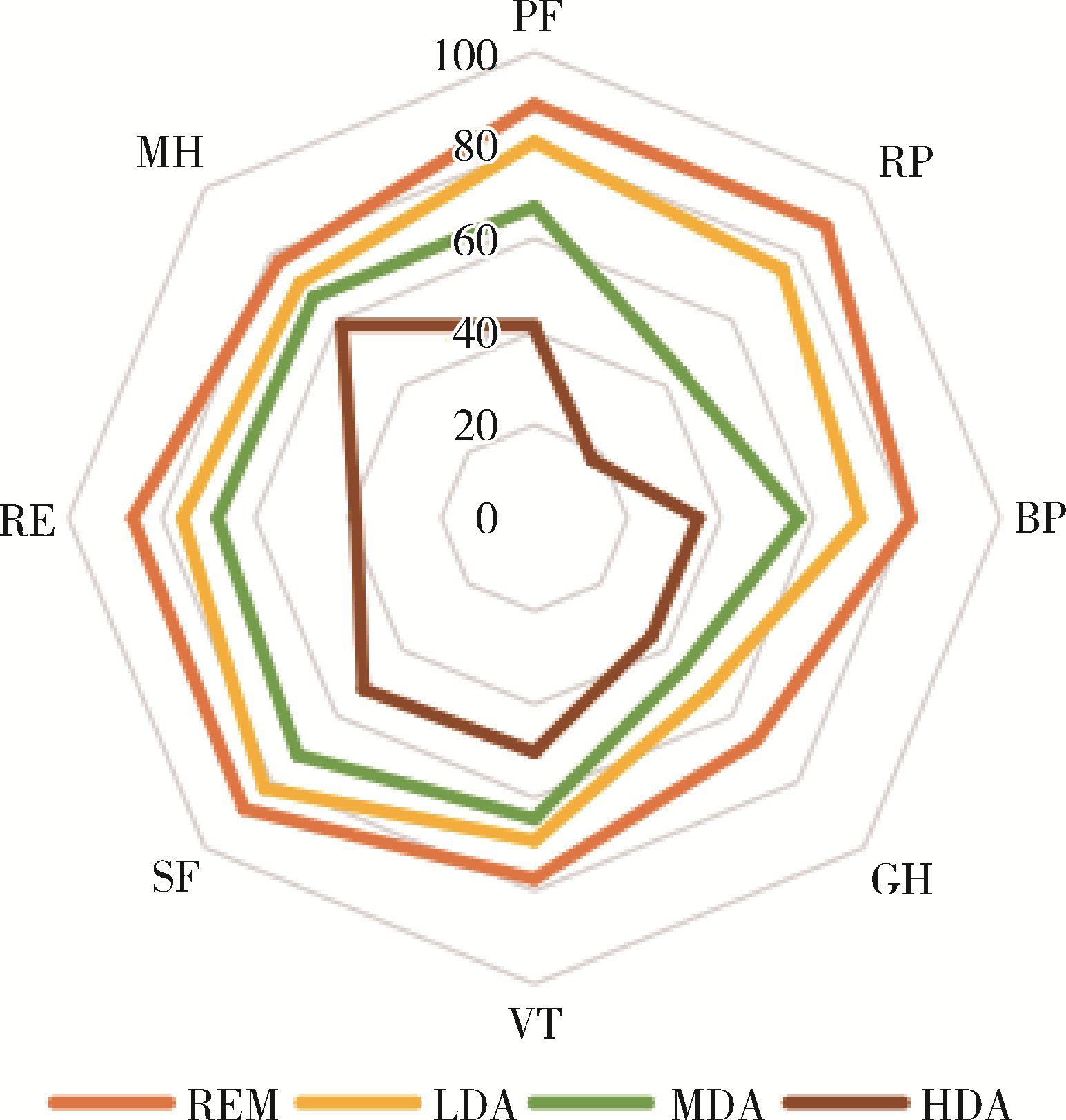
目的: 调查类风湿关节炎(rheumatoid arthritis,RA)患者健康相关生活质量(health related quality of life,HR-QoL)以及身体机能情况,分析疾病活动度对于HR-QoL以及各个维度身体机能的影响,并比较不同疾病活动判断标准下患者生活质量的差异。方法: 选择2021年1—7月于北京大学第三医院风湿免疫科门诊规律随诊的RA患者进行横断面调查,收集患者人口学资料、类风湿关节炎特异性生活质量(RA-specific quality of life,RA-QoL)评分以及36项简明健康调查问卷(the medical outcome 36-item short form health survey,SF-36)评分。符合正态分布的定量资料以${\bar x}$±s表示,两组间差异的比较采用t检验。结果: 共纳入RA患者207例,RA-QoL评分7.8±7.1,躯体功能汇总(physical component summary,PCS)评分63.8±23.8,心理功能汇总(mental component summary,MCS)评分71.7±21.0。以基于红细胞沉降率(erythrocyte sedimentation rate, ESR)的28个关节疾病活动度(disease activity score 28,DAS28)评分(DAS28-ESR)为标准,病情缓解、低疾病活动度的患者共119例(59.5%),以简明类风湿关节炎疾病活动指数(simplified disease activity index, SDAI)为标准,上述患者共125例(62.5%)。病情缓解或低疾病活动度的患者各个维度HR-QoL均显著优于治疗未达标的患者。以DAS28-ESR为评估标准,低疾病活动度组的生理功能评分(76.7±17.2 vs. 86.4±15.0, t=2.855, P < 0.01)、身体疼痛评分(67.8±8.5 vs. 77.7±15.6, t=4.277, P < 0.01)均低于完全缓解组,健康变化得分低于缓解组(52.8±22.3 vs. 63.9±24.1, t=2.134, P < 0.05),其他各个维度生活质量评分两组间差异无统计学意义。低疾病活动组PCS评分低于缓解组(68.3±15.2 vs. 77.3±15.2, t=2.716, P < 0.01),两组间MCS评分、RA-QoL评分差异无统计学意义。以SDAI为评估标准,低疾病活动度组RA-QoL评分显著高于缓解组(9.4±7.1 vs. 6.0±4.8, t=-2.260, P < 0.05),SF-36评分中躯体功能的各个维度以及PCS评分(69.9±16.4 vs. 81.4±15.1, t=3.879, P < 0.05)均低于缓解组,MCS评分低于缓解组(67.9±19.3 vs. 74.5±18.8, t=2.721, P < 0.01)。结论: 门诊就诊RA患者的RA-QoL以及SF-36评分情况较好,心理健康汇总评分高于躯体健康汇总评分,达标治疗对于提高HR-QoL至关重要。SDAI标准在缓解及低疾病活动度的RA患者中可以更好提示各个维度HR-QoL情况。
中图分类号:
- R593.22
| 1 |
Lee DM , Weinblatt ME . Rheumatoid arthritis[J]. Lancet, 2001, 358 (9285): 903- 911.
doi: 10.1016/S0140-6736(01)06075-5 |
| 2 | Lundkvist J , Kastäng F , Kobelt G , et al. The burden of rheumatoid arthritis and access to treatment: Health burden and costs[J]. Eur J Health Econ, 2008, 8 (Suppl 2): S49- S60. |
| 3 |
Li R , Sun J , Ren LM , et al. Epidemiology of eight common rheumatic diseases in China: A large-scale cross-sectional survey in Beijing[J]. Rheumatology (Oxford), 2012, 51 (4): 721- 729.
doi: 10.1093/rheumatology/ker370 |
| 4 | 中华人民共和国国家统计局第二次全国残疾人抽样调查领导小组. 第二次全国残疾人抽样调查主要数据公报[M]. 北京: 中国统计出版社, 2007. |
| 5 | Cunha-Miranda L , Santos H , Ferreira J , et al. Finding rheumatoid arthritis impact on life (FRAIL study): Economic burden[J]. Acta Reumatol Port, 2012, 37 (2): 134- 142. |
| 6 |
de Jong Z , van der Heijde D , McKenna SP , et al. The reliability and construct validity of the RAQoL: A rheumatoid arthritis-specific quality of life instrument[J]. Br J Rheumatol, 1997, 36 (8): 878- 883.
doi: 10.1093/rheumatology/36.8.878 |
| 7 |
Heimans L , Wevers-de Boer KV , Koudijs KK , et al. Health-related quality of life and functional ability in patients with early arthritis during remission steered treatment: Results of the IMPROVED study[J]. Arthritis Res Ther, 2013, 15 (5): R173.
doi: 10.1186/ar4361 |
| 8 |
Marshall S , Haywood K , Fitzpatrick R . Impact of patient-reported outcome measures on routine practice: A structured review[J]. J Eval Clin Pract, 2006, 12 (5): 559- 568.
doi: 10.1111/j.1365-2753.2006.00650.x |
| 9 |
Skevington SM , Day R , Chisholm A , et al. How much do doctors use quality of life information in primary care? Testing the trans-theoretical model of behaviour change[J]. Qual Life Res, 2005, 14 (4): 911- 922.
doi: 10.1007/s11136-004-3710-6 |
| 10 |
Rosa-Goncalves D , Bernardes M , Costa L . Quality of life and functional capacity in patients with rheumatoid arthritis: Cross-sectional study[J]. Reumatol Clin (Engl Ed), 2018, 14 (6): 360- 366.
doi: 10.1016/j.reuma.2017.03.002 |
| 11 |
Gerhold K , Richter A , Schneider M , et al. Health-related quality of life in patients with long-standing rheumatoid arthritis in the era of biologics: Data from the German biologics register RABBIT[J]. Rheumatology, 2015, 54 (10): 1858- 1866.
doi: 10.1093/rheumatology/kev194 |
| 12 |
Zhou YS , Wang XR , An Y , et al. Disability and health-related quality of life in Chinese patients with rheumatoid arthritis: A cross-sectional study[J]. Int J Rheum Dis, 2018, 21 (9): 1709- 1715.
doi: 10.1111/1756-185X.13345 |
| 13 |
Matcham F , Scott IC , Rayner L , et al. The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: A systematic review and meta-analysis[J]. Semin Arthritis Rheum, 2014, 44 (2): 123- 130.
doi: 10.1016/j.semarthrit.2014.05.001 |
| 14 |
Pencheva DT , Heaney A , McKenna SP , et al. Adaptation and validation of the rheumatoid arthritis quality of life (RAQoL) questionnaire for use in Bulgaria[J]. Rheumatol Int, 2020, 40 (12): 2077- 2083.
doi: 10.1007/s00296-020-04686-2 |
| 15 |
Rupp I , Boshuizen HC , Jacobi CE , et al. Impact of fatigue on health-related quality of life in rheumatoid arthritis[J]. Arthritis Rheum, 2004, 51 (4): 578- 585.
doi: 10.1002/art.20539 |
| 16 |
Bedi GS , Gupta N , Handa R , et al. Quality of life in Indian patients with rheumatoid arthritis[J]. Qual Life Res, 2005, 14 (8): 1953- 1958.
doi: 10.1007/s11136-005-4540-x |
| 17 |
Walker GJ , Littlejohn GO . Measuring quality of life in rheumatic conditions[J]. Clin Rheumatol, 2007, 26 (5): 671- 673.
doi: 10.1007/s10067-006-0450-8 |
| 18 |
Tander B , Cengiz K , Alayli G , et al. A comparative evaluation of health related quality of life and depression in patients with Wbromyalgia syndrome and rheumatoid arthritis[J]. Rheumatol Int, 2008, 28 (9): 859- 865.
doi: 10.1007/s00296-008-0551-6 |
| 19 |
Smolen JS , Aletaha D , Barton A , et al. Rheumatoid arthritis[J]. Nat Rev Dis Primers, 2018, 4, 18001.
doi: 10.1038/nrdp.2018.1 |
| 20 |
Waimann CA , Dal Pra FM , Marengo MF , et al. Quality of life of patients with rheumatoid arthritis in Argentina: Rliability, validity, and sensitivity to change of a Spanish version of the rheumatoid arthritis quality of life questionnaire[J]. Clin Rheumatol, 2012, 31 (7): 1065- 1071.
doi: 10.1007/s10067-012-1976-6 |
| 21 | Chiu YM , Lai MS , Lin HY , et al. Disease activity affects all domains of quality of life in patients with rheumatoid arthritis and is modified by disease duration[J]. Clin Exp Rheumatol, 2014, 32 (6): 898- 903. |
| 22 |
Schmalz G , Noack S , Patschan S , et al. Disease activity, morning stiffness and missing teeth are associated with oral health-related quality of life in individuals with rheumatoid arthritis[J]. Clin Oral Investig, 2020, 24 (10): 3559- 3566.
doi: 10.1007/s00784-020-03226-3 |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 郭睿霖, 张蕾, 王宇, 王晓庆, 王潇潇, 年凇汶, 张丽慧, 肖冰冰, 陆叶. 经闭孔尿道中段无张力悬吊改良术治疗女性压力性尿失禁的疗效[J]. 北京大学学报(医学版), 2026, 58(2): 337-341. |
| [3] | 吴滔, 林建子, 朱亚锋, 马剑达, 贾霈雯, 杨莉娟, 潘婕, 邹耀威, 杨迎, 卢烨, 戴冽. 血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物[J]. 北京大学学报(医学版), 2025, 57(6): 1024-1031. |
| [4] | 李岩岩, 刘香君, 李公明, 李春, 贾园. 抗磷脂综合征患者就医行为及治疗现状调查[J]. 北京大学学报(医学版), 2025, 57(6): 1107-1112. |
| [5] | 丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰. 利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1203-1207. |
| [6] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [7] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [8] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [9] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
| [10] | 王明瑞, 赖金惠, 姬家祥, 唐鑫伟, 胡浩浦, 王起, 许克新, 徐涛, 胡浩. 使用中文版威斯康星结石生活质量问卷预测肾结石患者生活质量降低的危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1069-1074. |
| [11] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [12] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [13] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [14] | 翟佳羽, 赵金霞, 安卓, 刘蕊. 低疾病活动度的中轴型脊柱关节炎患者残留症状评估及其相关因素分析[J]. 北京大学学报(医学版), 2024, 56(6): 987-993. |
| [15] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
|
||
