北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (4): 582-588. doi: 10.19723/j.issn.1671-167X.2024.04.006
肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素
欧俊永1,倪坤明2,马潞林1,王国良1,颜野1,杨斌1,李庚午1,宋昊东1,陆敏2,叶剑飞1,*( ),张树栋1,*()
),张树栋1,*()
- 1. 北京大学第三医院泌尿外科,北京 100191
2. 北京大学第三医院病理科,北京 100191
Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer
Junyong OU1,Kunming NI2,Lulin MA1,Guoliang WANG1,Ye YAN1,Bin YANG1,Gengwu LI1,Haodong SONG1,Min LU2,Jianfei YE1,*(),Shudong ZHANG1,*()
- 1. Department of Urology, Peking University Third Hospital, Beijing 100191, China
2. Department of Pathology, Peking University Third Hospital, Beijing 100191, China
摘要:
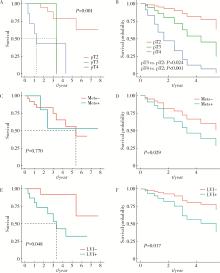
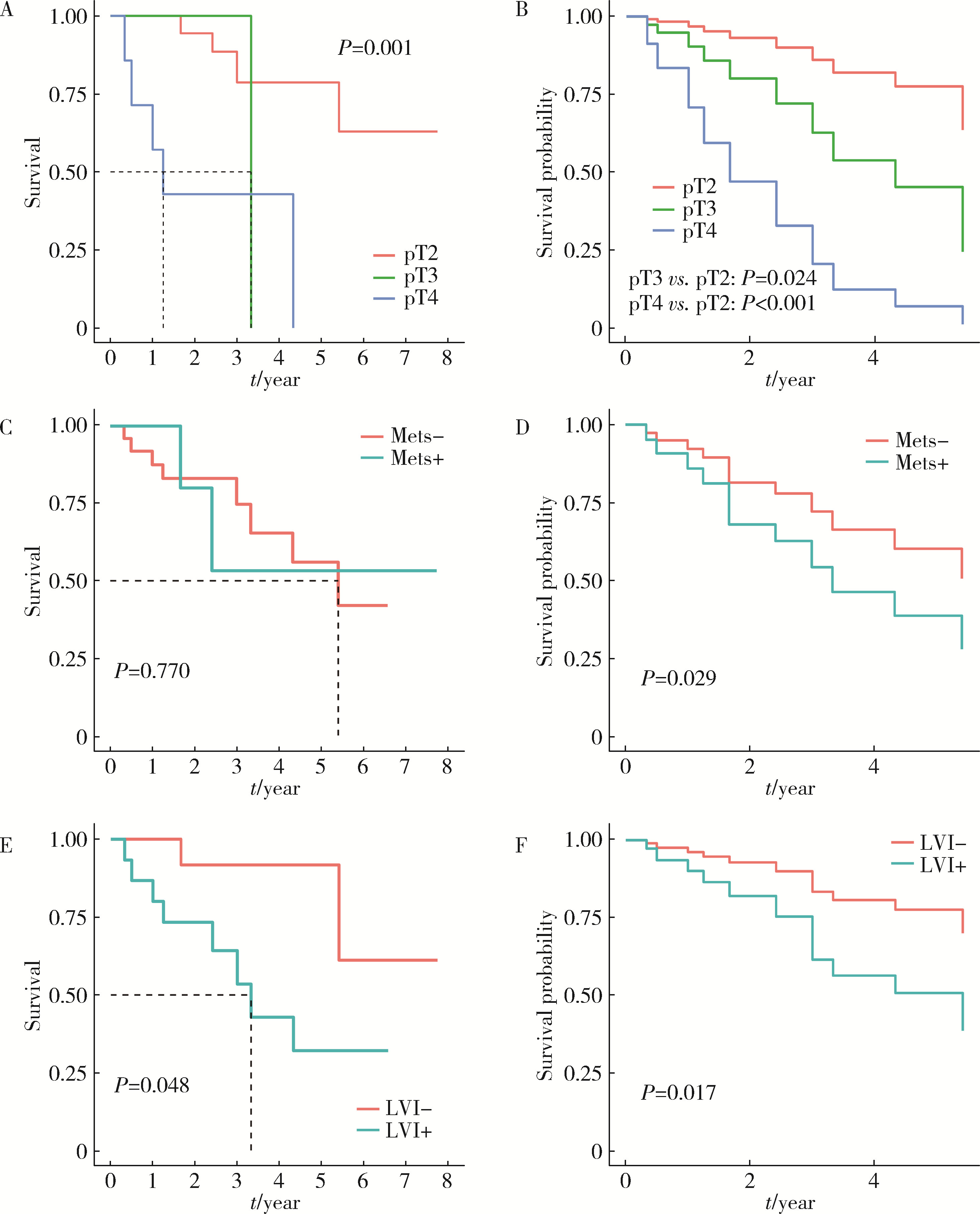
目的: 探究影响肌层浸润性膀胱癌(muscle-invasive bladder cancer, MIBC)合并中高危前列腺癌患者全因死亡结局的预后因素。方法: 回顾性分析2012年1月至2023年10月北京大学第三医院收治的MIBC合并中高危前列腺癌患者临床资料,随访并记录所有患者的全因死亡结局发生时间,并以其作为预后研究的结局事件。采用单因素及多因素Cox比例风险回归分析模型筛选MIBC合并中高危前列腺癌患者预后的独立影响因子,对于重要的影响因素(膀胱癌病理T分期、M分期、神经侵犯),绘制多因素Cox回归调整混杂因素前后的生存曲线。结果: 共纳入32例患者,平均年龄(72.5±6.6)岁,中位术前总前列腺特异性抗原(total prostate specific antigen,tPSA)6.68(2.47,6.84) μg/L,平均术前血肌酐(95±36) μmol/L,中位生存期为65个月。绝大多数(87.5%)患者膀胱癌病理分级为高级别,53.1%患者可见淋巴管侵犯,31.3%患者可见神经侵犯。25.0%的病例可见膀胱癌累及前列腺,手术软组织切缘阳性率为37. 5%。Cox多因素分析结果提示术前血肌酐水平(HR=1.02,95%CI:1.01~1.04)、膀胱癌病理分期T3(HR=11.58,95%CI:1.38~97.36)和T4(HR=19.53,95%CI:4.26~89.52)、膀胱癌转移(HR=9.44,95%CI:1.26~70.49)、膀胱癌神经侵犯(HR=6.26,95%CI:1.39~28.27)是影响患者预后的独立因素(P < 0.05)。调整混杂因素后的生存曲线与Log-rank检验结果提示膀胱癌病理分期T3、T4、M1和神经侵犯为影响患者生存预后的不良因素(P<0.05)。结论: MIBC合并中高危前列腺癌患者整体存在预后较差的趋势; 术前血肌酐高、膀胱癌病理分期T3或T4、膀胱癌转移、膀胱癌神经侵犯是MIBC合并中高危前列腺癌患者的不良预后因素。
中图分类号:
- R737.1
| 1 |
Alfred Witjes J , Max Bruins H , Carrión A , et al. European Association of Urology Guidelines on muscle-invasive and metastatic bladder cancer: Summary of the 2023 guidelines[J]. Eur Urol, 2024, 85 (1): 17- 31.
doi: 10.1016/j.eururo.2023.08.016 |
| 2 |
Siegel RL , Giaquinto AN , Jemal A . Cancer statistics, 2024[J]. CA Cancer J Clin, 2024, 74 (1): 12- 49.
doi: 10.3322/caac.21820 |
| 3 |
Dyrskjøt L , Hansel DE , Efstathiou JA , et al. Bladder cancer[J]. Nat Rev Dis Primers, 2023, 9 (1): 58.
doi: 10.1038/s41572-023-00468-9 |
| 4 |
Compérat E , Amin MB , Cathomas R , et al. Current best practice for bladder cancer: A narrative review of diagnostics and treatments[J]. Lancet, 2022, 400 (10364): 1712- 1721.
doi: 10.1016/S0140-6736(22)01188-6 |
| 5 |
Lopez-Beltran A , Cheng L , Montorsi F , et al. Concomitant bladder cancer and prostate cancer: Challenges and controversies[J]. Nat Rev Urol, 2017, 14 (10): 620- 629.
doi: 10.1038/nrurol.2017.124 |
| 6 |
Jing Y , Zhang R , Ma P , et al. Prevalence and clonality of synchronous primary carcinomas in the bladder and prostate[J]. J Pathol, 2018, 244 (1): 5- 10.
doi: 10.1002/path.4997 |
| 7 |
Aljabery F , Liedberg F , Häggström C , et al. Treatment and prognosis of patients with urinary bladder cancer with other primary cancers: A nationwide population-based study in the bladder can-cer data base Sweden (BladderBaSe)[J]. BJU Int, 2020, 126 (5): 625- 632.
doi: 10.1111/bju.15198 |
| 8 | Claps F , Pavan N , Umari P , et al. Incidence, predictive factors and survival outcomes of incidental prostate cancer in patients who underwent radical cystectomy for bladder cancer[J]. Minerva Urol Nephrol, 2021, 73 (3): 349- 356. |
| 9 |
Malte R , Kluth LA , Kaushik D , et al. Frequency and prognostic significance of incidental prostate cancer at radical cystectomy: Results from an international retrospective study[J]. Eur J Surg Oncol, 2017, 43 (11): 2193- 2199.
doi: 10.1016/j.ejso.2017.08.013 |
| 10 |
Fahmy O , Khairul-Asri MG , Schubert T , et al. Clinicopathological features and prognostic value of incidental prostatic adenocarcinoma in radical cystoprostatectomy specimens: A systematic review and meta-analysis of 13 140 patients[J]. J Urol, 2017, 197 (2): 385- 390.
doi: 10.1016/j.juro.2016.08.088 |
| 11 |
Kaelberer JB , O'donnell MA , Mitchell DL , et al. Incidental prostate cancer diagnosed at radical cystoprostatectomy for bladder cancer: Disease-specific outcomes and survival[J]. Prostate Int, 2016, 4 (3): 107- 112.
doi: 10.1016/j.prnil.2016.06.002 |
| 12 |
Wu S , Lin SX , Lu M , et al. Assessment of 5-year overall survival in bladder cancer patients with incidental prostate cancer identified at radical cystoprostatectomy[J]. Int Urol Nephrol, 2019, 51 (9): 1527- 1535.
doi: 10.1007/s11255-019-02181-7 |
| 13 |
Mazzucchelli R , Barbisan F , Scarpelli M , et al. Is incidentally detected prostate cancer in patients undergoing radical cystoprostatectomy clinically significant?[J]. Am J Clin Pathol, 2009, 131 (2): 279- 283.
doi: 10.1309/AJCP4OCYZBAN9TJU |
| 14 |
Moschini M , Shariat SF , Freschi M , et al. Impact of prostate involvement on outcomes in patients treated with radical cystoprostatectomy for bladder cancer[J]. Urol Int, 2017, 98 (3): 290- 297.
doi: 10.1159/000454736 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [4] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [5] | 刘艳华, 陆敏, 赵旭阳, 张宽根, 武睿, 梅放, 戴志豪, 由江峰, 裴斐. 肿瘤转移抑制基因LASS2去磷酸化对液泡型ATP酶活性及前列腺癌侵袭性的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1113-1123. |
| [6] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [7] | 宁家昕, 王浩然, 罗书航, 敬吉波, 王建业, 侯惠民, 刘明. 氧化应激相关基因与前列腺癌关系的多组学分析[J]. 北京大学学报(医学版), 2025, 57(4): 633-643. |
| [8] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [9] | 王泽远, 于栓宝, 郑浩轲, 陶金, 范雅峰, 张雪培. 基于临床特征和多参数MRI的前列腺癌盆腔淋巴结转移的术前预测模型[J]. 北京大学学报(医学版), 2025, 57(4): 684-691. |
| [10] | 缪祺, 洪保安, 张学舟, 孙志鹏, 王维, 王宇轩, 薄予轩, 赵佳晖, 张宁. 膀胱癌合并冠心病患者行经尿道膀胱肿瘤切除术围手术期抗血小板药物管理[J]. 北京大学学报(医学版), 2025, 57(4): 698-703. |
| [11] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [12] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [13] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [14] | 田宇轩,阮明健,刘毅,李德润,吴静云,沈棋,范宇,金杰. 双参数MRI改良PI-RADS评分4分和5分病灶的最大径对临床有意义前列腺癌的预测效果[J]. 北京大学学报(医学版), 2024, 56(4): 567-574. |
| [15] | 姚凯烽,阮明健,李德润,田宇轩,陈宇珂,范宇,刘毅. 靶向穿刺联合区域系统穿刺对PI-RADS 4~5分患者的前列腺癌诊断效能[J]. 北京大学学报(医学版), 2024, 56(4): 575-581. |
|
||
