北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (5): 896-901. doi: 10.19723/j.issn.1671-167X.2024.05.022
穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建
李志存, 吴天俣, 梁磊, 范宇, 孟一森*( ), 张骞*()
), 张骞*()
- 北京大学第一医院泌尿外科,北京大学泌尿外科研究所,泌尿生殖系疾病(男)分子诊治北京市重点实验室,国家泌尿男生殖系肿瘤中心,北京 100034
Risk factors analysis and nomogram model construction of postoperative pathological upgrade of prostate cancer patients with single core positive biopsy
Zhicun LI, Tianyu WU, Lei LIANG, Yu FAN, Yisen MENG*(), Qian ZHANG*()
- Department of Urology, Peking University First Hospital; Institution of Urology, Peking University; Beijing Key Laboratory of Urogenital Diseases (Male) Molecular Diagnosis and Treatment Center; National Urological Cancer Center, Beijing 100034, China
摘要:
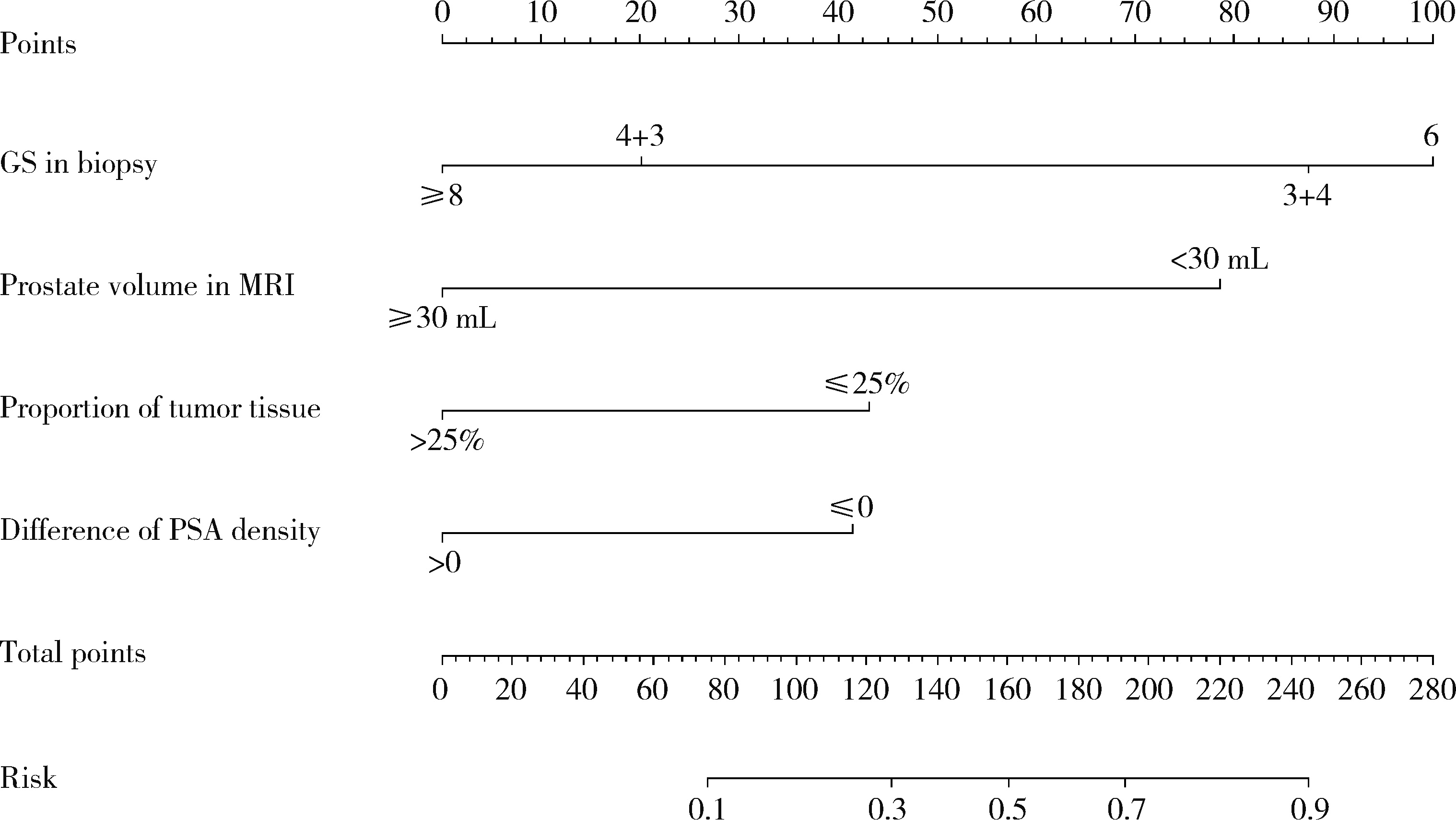
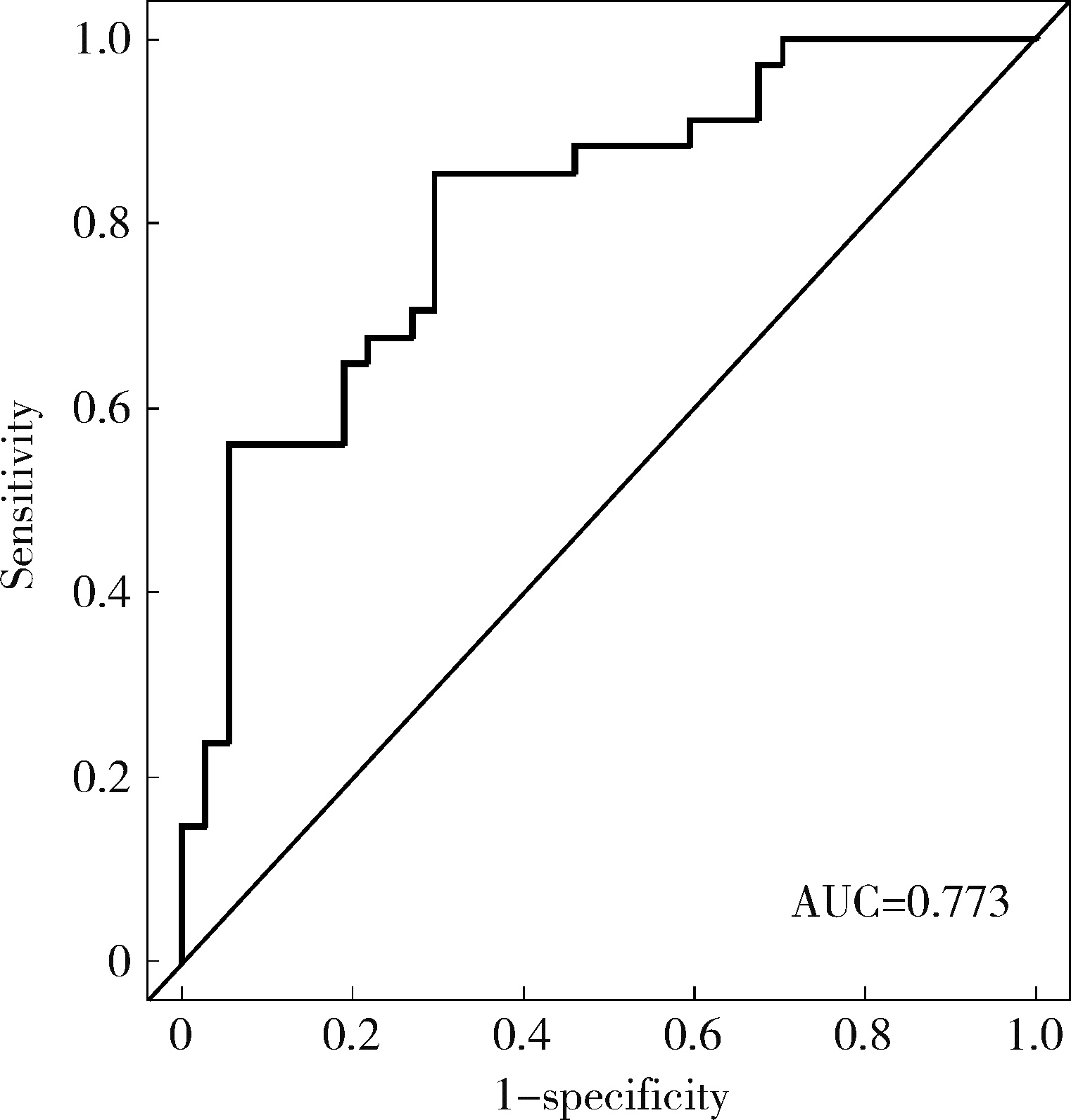
目的: 对穿刺活检单针阳性前列腺癌术后病理升级的危险因素进行分析,并尝试构建预测穿刺单针阳性前列腺癌患者术后病理升级的数学模型。方法: 回顾分析2015年1月至2020年8月期间于北京大学第一医院诊断为前列腺癌且接受根治性前列腺切除术的患者1 349例,选取其中穿刺活检单针阳性患者的临床资料,将其分为术后病理较穿刺病理升级组及未升级组,比较两组的年龄、体重指数、临床分期、前列腺影像报告和数据系统(prostate imaging reporting and data system,PI-RADS)评分、磁共振成像(magnetic resonance imaging,MRI)报告的前列腺体积、前列腺穿刺活检的Gleason评分、穿刺前及术前血清前列腺特异性抗原(prostate specific antigen,PSA)、手术方式、术后病理分期的差异,将单因素分析中P < 0.1的术前变量纳入多因素Logistic回归并绘制列线图,通过受试者工作特征曲线对模型进行评价。结果: 共有71例患者符合纳入排除标准,其中术后病理升级组34例,未升级组37例,两组患者的年龄(P=0.585)、体重指数(P=0.165)、手术方式(P=0.08)、MRI前列腺体积(P=0.067)、临床分期(P=0.678)、PI-RADS评分(P=0.203)、穿刺前PSA(P=0.359)、术前PSA(P=0.739)、PSA密度差(P=0.063)、穿刺Gleason评分(P=0.068)差异均无统计学意义,两组患者穿刺阳性针中肿瘤组织占比(P=0.007)、术后病理分期(P < 0.001)及术后Gleason评分(P < 0.001)差异有统计学意义。将单因素分析中P < 0.1的术前变量,即MRI前列腺体积、PSA密度差、穿刺阳性针中的肿瘤组织占比、穿刺Gleason评分纳入多因素Logistic回归分析,只有MRI前列腺体积组间差异有统计学意义。进一步根据多因素Logistic回归结果绘制列线图,受试者工作特征曲线的曲线下面积为0.773。结论: 对于穿刺病理单针阳性的前列腺癌患者,若前列腺体积较小或穿刺阳性针中肿瘤组织占比较少,需警惕术后病理较穿刺病理升级的可能;对于可能出现病理升级的患者,需谨慎考虑术前的危险分层。本模型可初步用于预测穿刺活检单针阳性前列腺癌患者术后病理升级的可能性。
中图分类号:
- R737.25


| 1 | 郑荣寿, 陈茹, 韩冰峰, 等. 2022年中国恶性肿瘤流行情况分析[J]. 中华肿瘤杂志, 2024, 46 (3): 221- 231. |
| 2 |
Siegel RL , Miller KD , Jemal A . Cancer statistics, 2020[J]. CA Cancer J Clin, 2020, 70 (1): 7- 30.
doi: 10.3322/caac.21590 |
| 3 | 徐毅, 毛祺琦, 刘犇, 等. 穿刺单针阳性前列腺癌的术后病理特征分析[J]. 中华泌尿外科杂志, 2018, 39 (10): 757- 760. |
| 4 | 陈小豹, 张潮鸿, 江玮, 等. 前列腺穿刺单针阳性的临床特点[J]. 中国男科学杂志, 2019, 33 (3): 30- 33. |
| 5 | 唐超来, 唐贤富, 郑兴明. 前列腺穿刺活检单针阳性患者行前列腺根治性切除术后的病理特征[J]. 国际泌尿系统杂志, 2020, 40 (4): 587- 590. |
| 6 |
Goldstein NS , Bégin LR , Grody WW , et al. Minimal or no cancer in radical prostatectomy specimens. Report of 13 cases of the "vanishing cancer phenomenon"[J]. Am J Surg Pathol, 1995, 19 (9): 1002- 1009.
doi: 10.1097/00000478-199509000-00003 |
| 7 |
Ricardo Kupka da S , Dall'Oglio MF , Sant'Ana AC , et al. Can single positive core prostate cancer at biopsy be considered a low-risk disease after radical prostatectomy?[J]. Int Braz J Urol, 2013, 39 (6): 800- 807.
doi: 10.1590/S1677-5538.IBJU.2013.06.05 |
| 8 | 刘希高, 谌诚, 李健, 等. 前列腺穿刺活检单针阳性患者前列腺内癌灶分布特点[J]. 中华男科学杂志, 2012, 18 (2): 155- 159. |
| 9 | 杜少静, 贺慧颖. 穿刺单针阳性前列腺癌患者根治术后62例临床病理分析[J]. 中华病理学杂志, 2016, 45 (7): 446- 450. |
| 10 |
郝一昌, 颜野, 张帆, 等. 穿刺活检单针阳性的前列腺癌手术策略选择及经验总结[J]. 北京大学学报(医学版), 2020, 52 (4): 625- 631.
doi: 10.19723/j.issn.1671-167X.2020.04.005 |
| 11 | Dong F , Jones JS , Stephenson AJ , et al. Prostate cancer volume at biopsy predicts clinically significant upgrading[J]. J Urol, 2008, 179 (3): 896- 900. |
| 12 | Hwang I , Lim D , Jeong YB , et al. Upgrading and upstaging of low-risk prostate cancer among Korean patients: A multicenter study[J]. Asian J Androl, 2015, 17 (5): 811- 814. |
| [1] | 王楠楠, 袁大晋, 朱昱冰, 丁磊. 结直肠癌根治术后肝转移风险多中心列线图预测模型的构建与验证[J]. 北京大学学报(医学版), 2026, 58(2): 290-300. |
| [2] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [3] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [4] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [5] | 刘艳华, 陆敏, 赵旭阳, 张宽根, 武睿, 梅放, 戴志豪, 由江峰, 裴斐. 肿瘤转移抑制基因LASS2去磷酸化对液泡型ATP酶活性及前列腺癌侵袭性的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1113-1123. |
| [6] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [7] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [8] | 宁家昕, 王浩然, 罗书航, 敬吉波, 王建业, 侯惠民, 刘明. 氧化应激相关基因与前列腺癌关系的多组学分析[J]. 北京大学学报(医学版), 2025, 57(4): 633-643. |
| [9] | 王泽远, 于栓宝, 郑浩轲, 陶金, 范雅峰, 张雪培. 基于临床特征和多参数MRI的前列腺癌盆腔淋巴结转移的术前预测模型[J]. 北京大学学报(医学版), 2025, 57(4): 684-691. |
| [10] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [11] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [12] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [13] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [14] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [15] | 李钰锴, 王红彦, 罗靓, 李云, 李春. 抗磷脂抗体在白塞病合并血栓中的临床意义[J]. 北京大学学报(医学版), 2024, 56(6): 1036-1040. |
|
||
