北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 543-550. doi: 10.19723/j.issn.1671-167X.2026.03.014
生物学年龄在社区人群队列中预测心血管病风险的应用
陆梦溪1, 王炳翰1, 康佳丽1, 刘秋萍1, 周逸帆1, 孙烨祥2, 沈鹏2, 林鸿波2, 唐迅1,3,4,*( ), 高培1,3,4,*()
), 高培1,3,4,*()
- 1. 北京大学公共卫生学院流行病与卫生统计学系,北京 100191
2. 宁波市鄞州区疾病预防控制中心,浙江宁波 315101
3. 重大疾病流行病学教育部重点实验室(北京大学),北京 100191
4. 北京大学临床研究所真实世界证据评价中心,北京 100191
Application of biological age for cardiovascular risk prediction in a community-based Chinese cohort
Mengxi LU1, Binghan WANG1, Jiali KANG1, Qiuping LIU1, Yifan ZHOU1, Yexiang SUN2, Peng SHEN2, Hongbo LIN2, Xun TANG1,3,4,*(), Pei GAO1,3,4,*()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Yinzhou District Center for Disease Control and Prevention, Ningbo 315101, Zhejiang, China
3. Key Laboratory of Epidemiology of Major Disease (Peking University), Ministry of Education, Beijing 100191, China
4. Center for Real-world Evidence Evaluation, Peking University Clinical Research Institute, Beijing 100191, China
摘要:
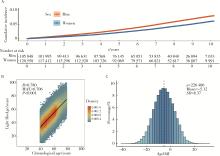
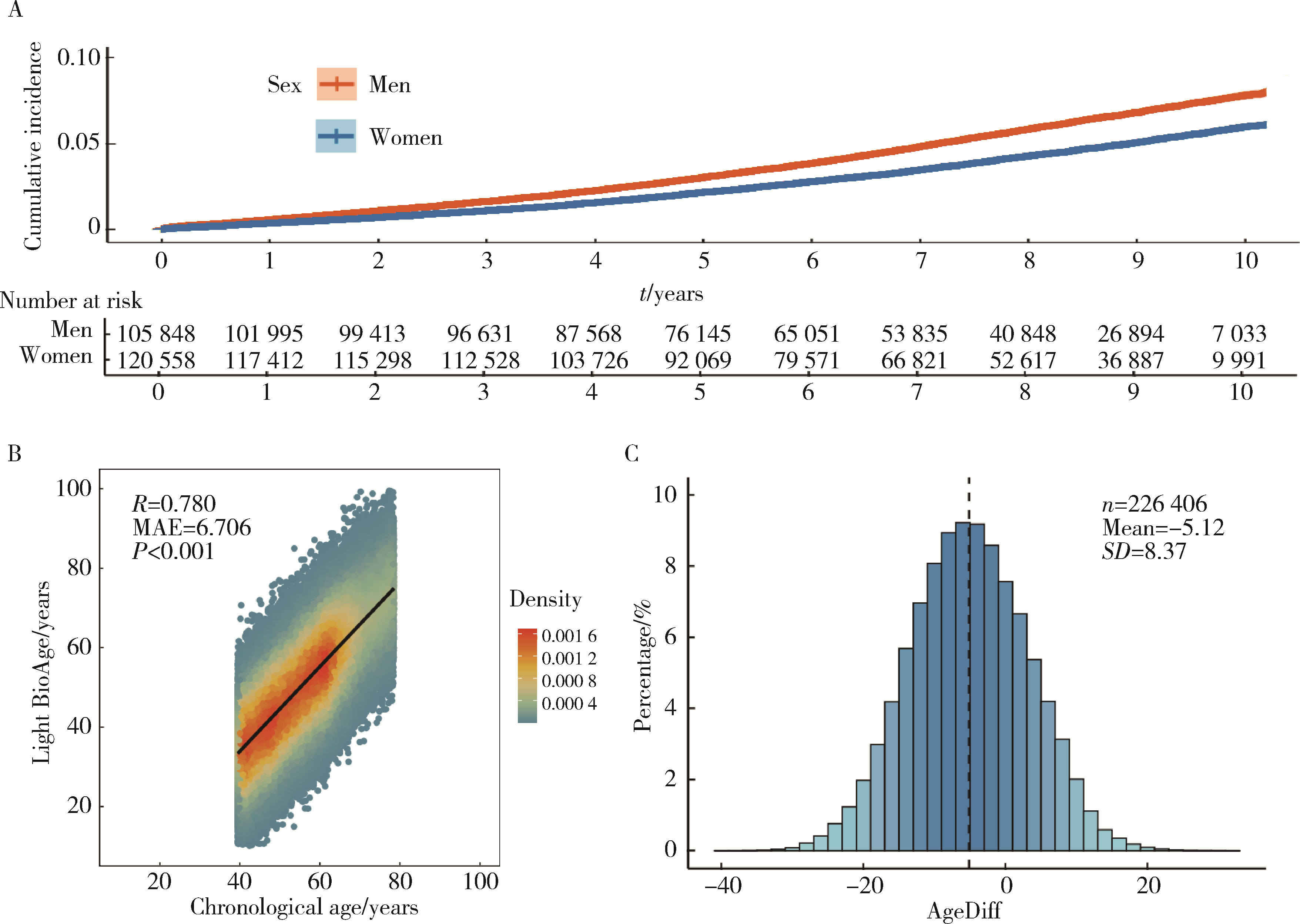
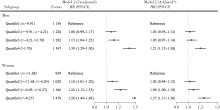
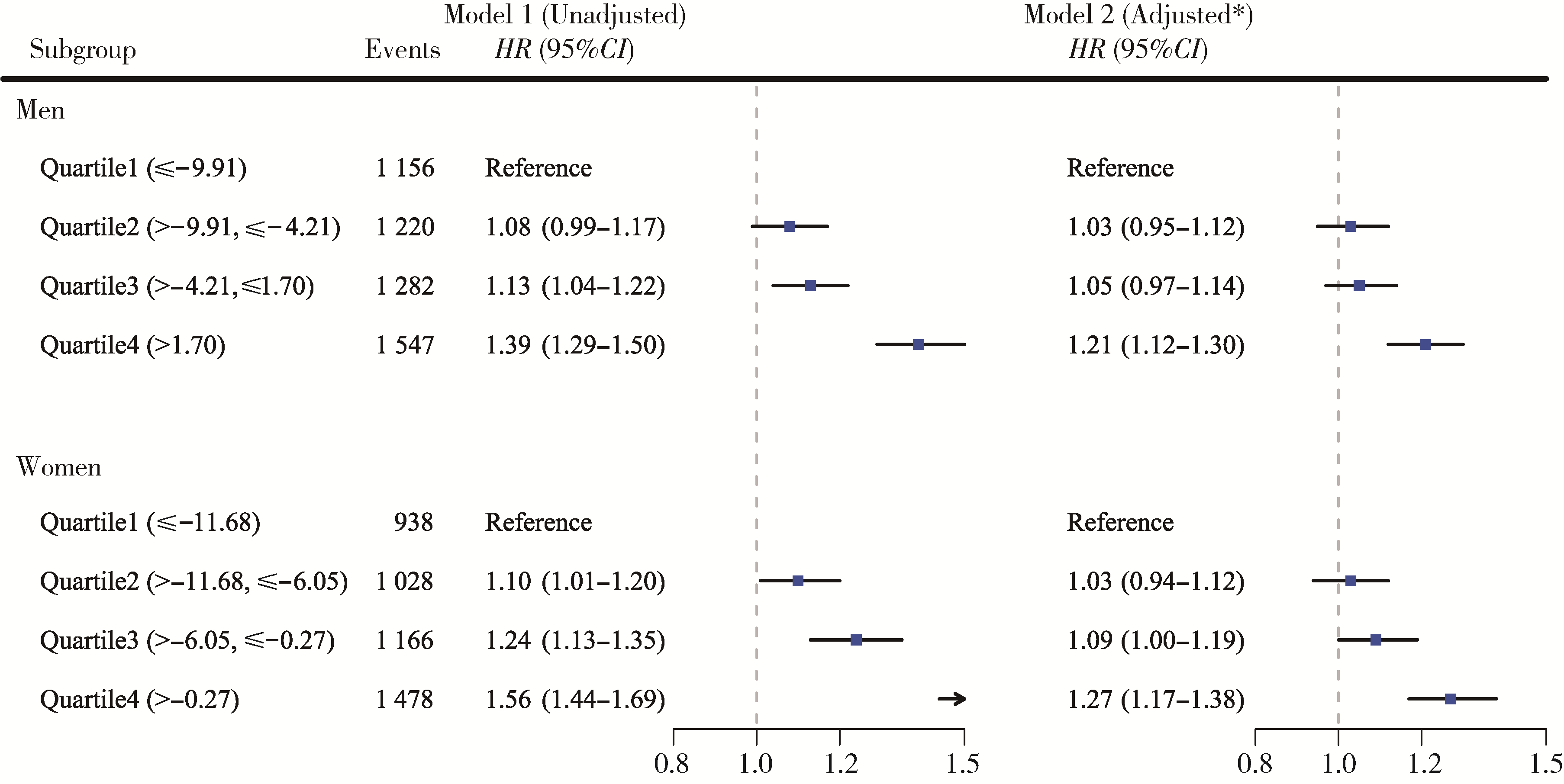
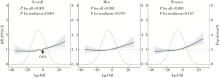
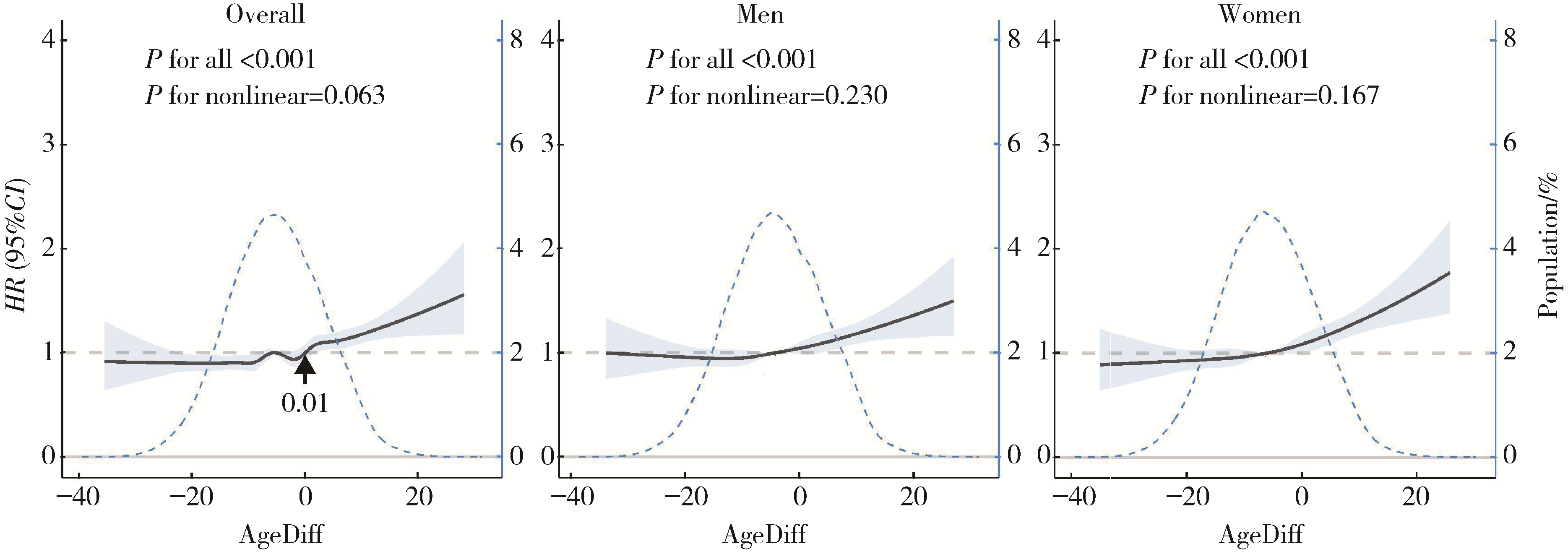
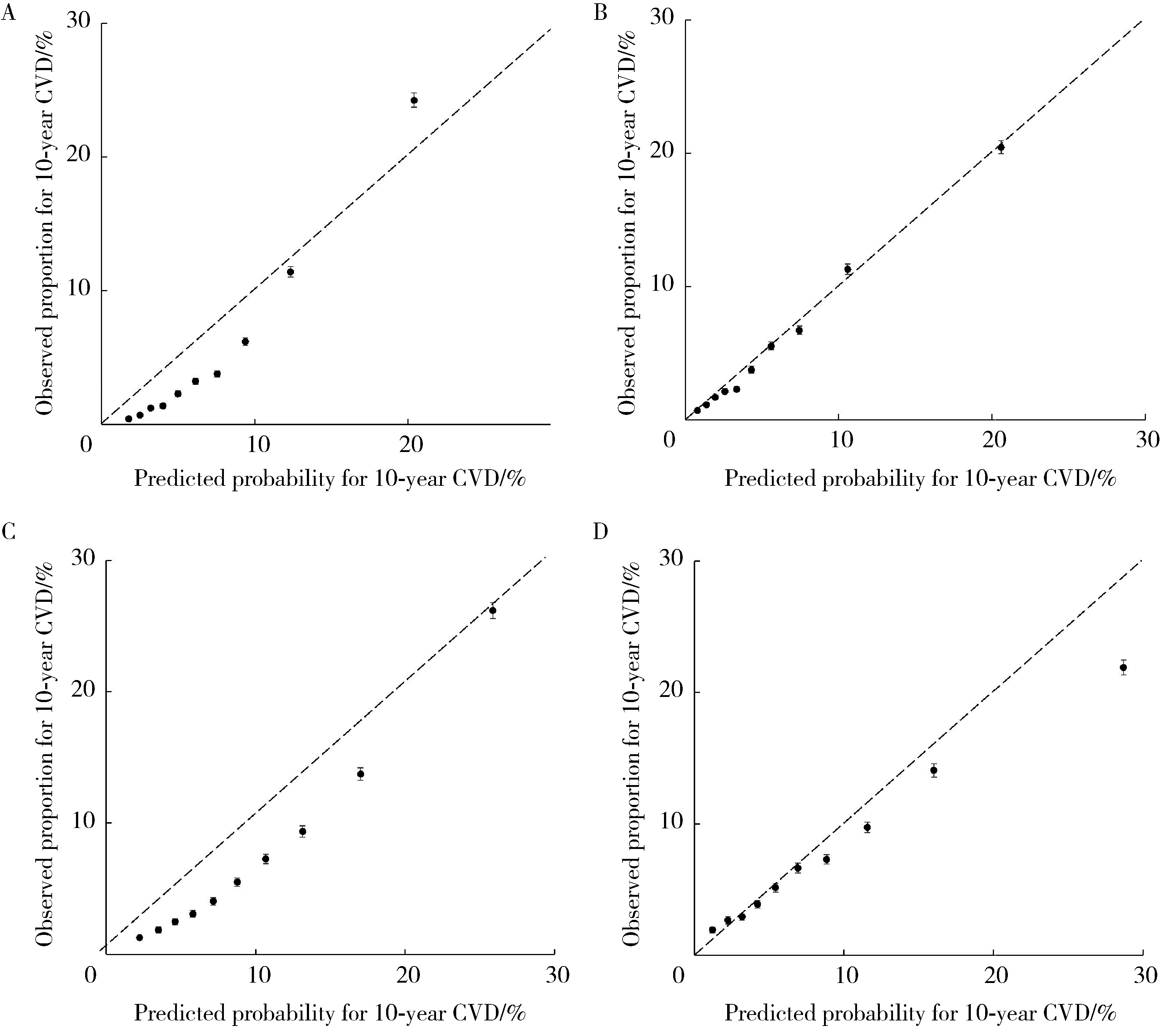
目的: 在大样本社区人群队列中独立验证Light BioAge模型计算的简易生物学年龄预测全因死亡的区分度,并探索其与时序年龄的差值和心血管病发病及死亡结局事件的关联,以及生物学年龄对心血管病风险预测的实际应用价值。方法: 研究对象为中国鄞州电子健康档案研究(CHinese Electronic health Records Research in Yinzhou,CHERRY)队列中40~79岁基线无心血管病史的人群,利用C统计量(Harrell’s concordance index,C-index) 评估仅通过空腹血糖、血清肌酐和超敏C反应蛋白三个临床常用指标构建的Light BioAge模型在全人群及不同性别亚组中预测全因死亡的外部验证区分度,采用Cox比例风险模型分析年龄差值与首次发生的心血管病发病和心血管病死亡复合终点的关联,调整时序年龄、性别、教育水平、居住地、吸烟状态、体重指数、收缩压、总胆固醇及高密度脂蛋白胆固醇等影响因素后计算风险比(hazard ratio,HR)及其95%置信区间(confidence interval,CI)。采用限制性立方样条回归方法进一步分析年龄差值与心血管病结局事件的潜在非线性关联。在2019年世界卫生组织(World Health Organization,WHO)开发的心血管病风险预测简易模型中采用生物学年龄替换时序年龄,评估对10年心血管病风险预测区分度和校准度的影响。结果: 共纳入226 406名研究对象,人群的基线平均年龄为55.0岁,53.2%为女性。在中位7.39年(累计1 562 141人年)的随访期间,共有11 703人(7.49/1 000人年)发生死亡,9 815人(6.30/1 000人年)发生心血管病发病和死亡复合结局事件。Light BioAge模型计算的生物学年龄及年龄差值的中位数分别为49.31和-5.19,提示其整体上低于时序年龄;虽然Light BioAge模型在全人群中预测全因死亡的区分度较好(C统计量:0.742,95%CI:0.738~0.746),但在男性中的区分度低于女性[C统计量分别为0.722(95%CI:0.714~0.730)和0.755(95%CI:0.749~0.761)]。调整其他影响因素后,心血管病结局事件的风险呈现随年龄差值增大而增高的趋势(Ptrend < 0.001);年龄差值处于上四分位数组与下四分位数组相比,男性心血管病结局事件的风险增加了21%(HR=1.21,95%CI:1.12~1.30),女性增加了27%(HR=1.27,95%CI:1.17~1.38)。限制性立方样条回归的结果进一步显示,总人群的心血管病结局事件的风险随年龄差值的增加而升高,且男性、女性亚组中并未发现明显的阈值效应(非线性关联P>0.05)。在WHO模型中采用生物学年龄替换时序年龄后,预测心血管病风险的区分度无改善,但校准度有明显提升,尤其是在女性人群中从时序年龄模型整体风险高估的20.5%[预测/观察比(expected/observed ratio,EOR)=1.205,95%CI:1.167~1.246]改善为生物学年龄替换后的整体风险仅略微低估2.1%(EOR=0.979,95%CI:0.948~1.012)。结论: Light BioAge模型构建的简易生物学年龄在大样本社区人群中预测全因死亡的区分度较好,生物学年龄和时序年龄的差值增大将增加心血管病结局事件的风险,在WHO心血管病风险预测模型中用生物学年龄替换时序年龄后,模型的校准度明显改善,特别是在女性人群。
中图分类号:
- R181.2
| 1 |
|
| 2 |
doi: 10.1111/acel.13080 |
| 3 |
doi: 10.1038/s44161-024-00438-8 |
| 4 |
|
| 5 |
doi: 10.1016/j.jacc.2019.11.062 |
| 6 |
|
| 7 |
doi: 10.1161/CIRCRESAHA.121.318965 |
| 8 |
|
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
|
| 17 |
|
| 18 |
|
| [1] | 王玉霖, 郜鑫, 刘志科, 詹思延. 2018—2023年江苏省0~3岁婴幼儿肠套叠发病的流行病学特征[J]. 北京大学学报(医学版), 2026, 58(3): 490-495. |
| [2] | 徐慧颖, 何兴侯, 黄薇, 张彬, 李梦瑶, 刘家辉, 方言, 赵二璐, 魏相睿, 马旭, 杨英. 中国育龄女性围孕期冷热暴露与先天性心脏病发病风险的关联[J]. 北京大学学报(医学版), 2026, 58(3): 503-512. |
| [3] | 范梦, 王梦莹, 王斯悦, 彭和香, 王雪珩, 郭煌达, 侯天姣, 秦雪英, 陈大方, 胡永华, 李劲, 武轶群, 吴涛. 动脉硬化相关指标与死亡风险的前瞻性队列研究[J]. 北京大学学报(医学版), 2025, 57(6): 1153-1159. |
| [4] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [5] | 周恬静,刘秋萍,张明露,刘晓非,康佳丽,沈鹏,林鸿波,唐迅,高培. 基于马尔科夫模型的社区人群启动降压药物治疗预防心血管病的策略比较[J]. 北京大学学报(医学版), 2024, 56(3): 441-447. |
| [6] | 刘晓强,周寅. 牙种植同期植骨术围术期高血压的相关危险因素[J]. 北京大学学报(医学版), 2024, 56(1): 93-98. |
| [7] | 张紫薇,花语蒙,刘爱萍. 中国中老年人群抑郁症状、缺血性心血管疾病10年风险对心血管疾病的联合影响[J]. 北京大学学报(医学版), 2023, 55(3): 465-470. |
| [8] | 于欢,杨若彤,王斯悦,吴俊慧,王梦莹,秦雪英,吴涛,陈大方,武轶群,胡永华. 2型糖尿病患者使用二甲双胍与缺血性脑卒中发病风险的队列研究[J]. 北京大学学报(医学版), 2023, 55(3): 456-464. |
| [9] | 马涛,李艳辉,陈曼曼,马莹,高迪,陈力,马奇,张奕,刘婕妤,王鑫鑫,董彦会,马军. 青春期启动提前与儿童肥胖类型的关联研究: 基于横断面调查和队列调查[J]. 北京大学学报(医学版), 2022, 54(5): 961-970. |
| [10] | 梁喆,范芳芳,张岩,秦献辉,李建平,霍勇. 中国高血压人群中H型高血压的比率和特征及与美国人群的比较[J]. 北京大学学报(医学版), 2022, 54(5): 1028-1037. |
| [11] | 王佳敏,刘秋萍,张明露,巩超,刘舒丹,陈暐烨,沈鹏,林鸿波,高培,唐迅. 基于马尔可夫模型的社区人群糖尿病筛查预防心血管病的效果评价[J]. 北京大学学报(医学版), 2022, 54(3): 450-457. |
| [12] | 巩超, 刘秋萍, 王佳敏, 刘晓非, 张明露, 杨瀚, 沈鹏, 林鸿波, 唐迅, 高培. 社区人群他汀干预策略预防心血管病效果的马尔可夫模型评价[J]. 北京大学学报(医学版), 2022, 54(3): 443-449. |
| [13] | 刘晓强,杨洋,周建锋,刘建彰,谭建国. 640例单牙种植术对血压和心率影响的队列研究[J]. 北京大学学报(医学版), 2021, 53(2): 390-395. |
| [14] | 刘欢,何映东,刘金波,黄薇,赵娜,赵红薇,周晓华,王宏宇. 血管健康指标对新发心脑血管事件的预测价值:北京血管健康分级标准的初步验证[J]. 北京大学学报(医学版), 2020, 52(3): 514-520. |
| [15] | 孟文颖,黄琬桐,张杰,焦明远,金蕾,靳蕾. 孕早期血清维生素E水平与妊娠期高血压疾病发病风险的关系[J]. 北京大学学报(医学版), 2020, 52(3): 470-478. |
|
||
