Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (4): 698-705. doi: 10.19723/j.issn.1671-167X.2019.04.018
Previous Articles Next Articles
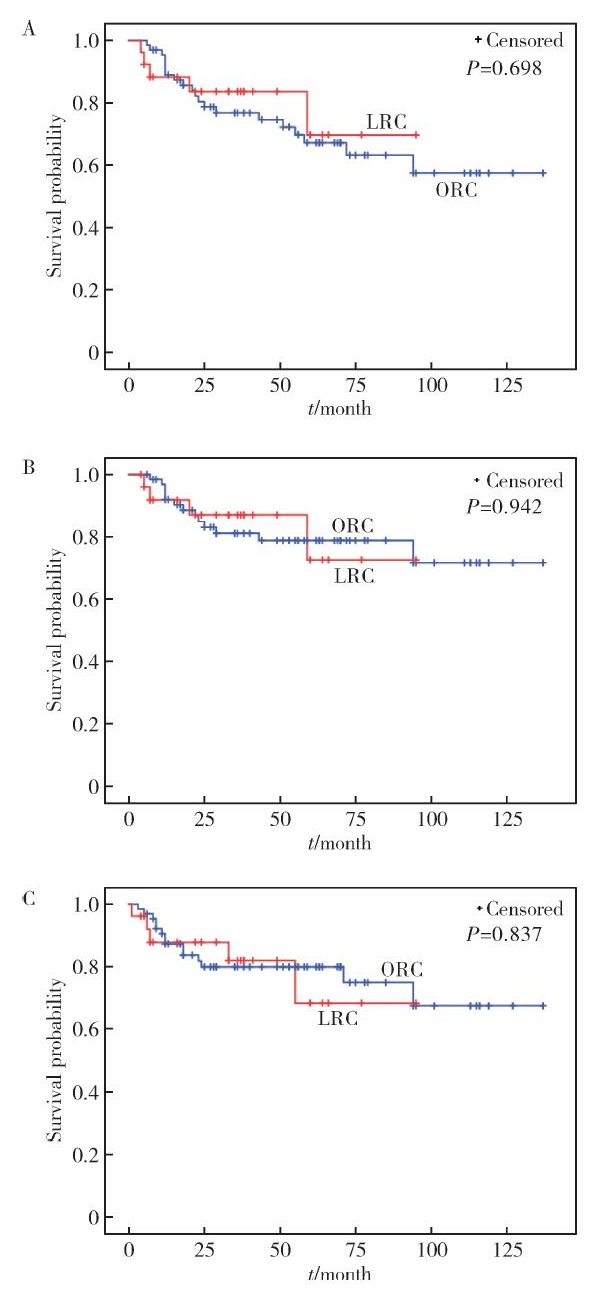
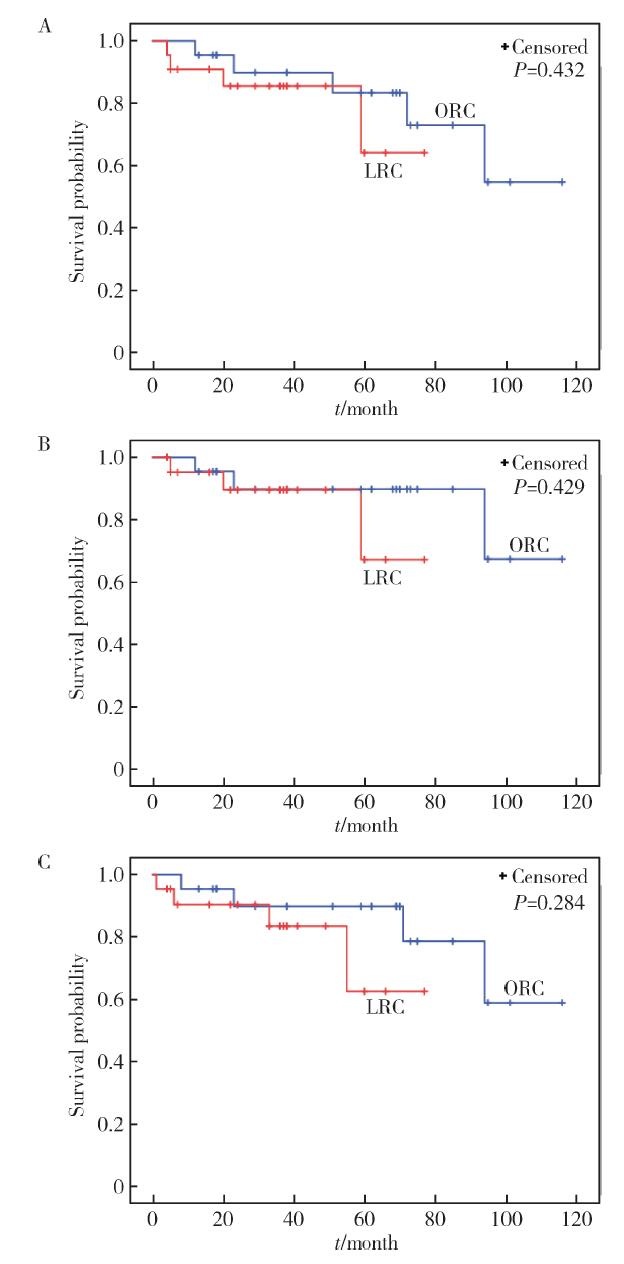
Propensity-matched comparison of laparoscopic and open radical cystectomy for female patients with bladder cancer
Hai-wen HUANG1,Bing YAN2,Mei-xia SHANG3,Li-bo LIU1,Han HAO1,Zhi-jun XI1,△( )
)
- 1.Department of Urology, Peking University First Hospital; Institute of Urology, Peking University; National Urological Cancer Center, Beijing 100034, China
2. Department of Urology, Xingtai People’s Hospital, Xingtai 054001, Hebei, China
3. Department of Medical Statistics, Peking University First Hospital, Beijing 100034, China
CLC Number:
- R737.14


| [1] | Antoni S, Ferlay J, Soerjomataram I , et al. Bladder cancer incidence and mortality: A global overview and recent trends[J]. Eur Urol, 2017,71(1):96-108. |
| [2] | Pang C, Guan Y, Li H , et al. Urologic cancer in China[J]. Jpn J Clin Oncol, 2016,46(6):497-501. |
| [3] | Tang K, Li H, Xia D , et al. Laparoscopic versus open radical cystectomy in bladder cancer: A systematic review and meta-analysis of comparative studies[J]. PLoS One, 2014,9(5):e95667. |
| [4] | Esquinas C, Alonso JM, Mateo E , et al. Prospective study comparing laparoscopic and open radical cystectomy: Surgical and oncological results[J]. Actas Urol Esp, 2018,42(2):94-102. |
| [5] | Guillotreau J, Game X, Mouzin M , et al. Radical cystectomy for bladder cancer: morbidity of laparoscopic versus open surgery[J]. J Urol, 2009,181(2):554-559. |
| [6] | Ha US, Kim SI, Kim SJ , et al. Laparoscopic versus open radical cystectomy for the management of bladder cancer: Mid-term oncological outcome[J]. Int J Urol, 2010,17(1):55-61. |
| [7] | Haber GP, Crouzet S, Gill IS . Laparoscopic and robotic assisted radical cystectomy for bladder cancer: A critical analysis[J]. Eur Urol, 2008,54(1):54-62. |
| [8] | Hemal AK, Kolla SB . Comparison of laparoscopic and open radical cystoprostatectomy for localized bladder cancer with 3-year oncological followup: a single surgeon experience[J]. J Urol, 2007,178(6):2340-2343. |
| [9] | Porpiglia F, Renard J, Billia M , et al. Open versus laparoscopy-assisted radical cystectomy: Results of a prospective study[J]. J Endourol, 2007,21(3):325-329. |
| [10] | Wang SZ, Chen LW, Zhang YH , et al. Comparison of hand-assisted laparoscopic and open radical cystectomy for bladder can-cer[J]. Urol Int, 2010,84(1):28-33. |
| [11] | Lin T, Fan X, Zhang C , et al. A prospective randomised controlled trial of laparoscopic vs. open radical cystectomy for bladder cancer: perioperative and oncologic outcomes with 5-year follow-up T Lin et al[J]. Br J Cancer, 2014,110(4):842-849. |
| [12] | Dobruch J, Daneshmand S, Fisch M , et al. Gender and bladder cancer: a collaborative review of etiology, biology, and outcomes[J]. Eur Urol, 2016,69(2):300-310. |
| [13] | Stenzl A . Cystectomy: technical considerations in male and female patients[J]. EAU Update Series, 2005,3(3):138-146. |
| [14] |
孟一森, 王宇, 范宇 , 等. 根治性膀胱全切手术及尿流改道方式对高龄患者围手术期并发症的影响[J]. 北京大学学报(医学版), 2016,48(4):632-637.
doi: 10.3969/j.issn.1671-167X.2016.04.013 |
| [15] | Shabsigh A, Korets R, Vora KC , et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology[J]. Eur Urol, 2009,55(1):164-174. |
| [16] | Stein JP, Lieskovsky G, Cote R , et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1 054 patients[J]. J Clin Oncol, 2001,19(3):666-675. |
| [17] | Studer UE, Burkhard FC, Schumacher M , et al. Twenty years experience with an ileal orthotopic low pressure bladder substitute: lessons to be learned[J]. J Urol, 2006,176(1):161-166. |
| [18] | Parra RO, Andrus CH, Jones JP , et al. Laparoscopic cystectomy: initial report on a new treatment for the retained bladder[J]. J Urol, 1992,148(4):1140-1144. |
| [19] | Aboumarzouk OM, Hughes O, Narahari K , et al. Safety and feasibility of laparoscopic radical cystectomy for the treatment of bladder cancer[J]. J Endourol, 2013,27(9):1083-1095. |
| [20] | Biondi-Zoccai G, Romagnoli E, Agostoni P , et al. Are propensity scores really superior to standard multivariable analysis?[J]. Contemp Clin Trials, 2011,32(5):731-740. |
| [21] | 焦明旭, 张晓, 刘迪 , 等. 倾向性评分匹配在非随机对照研究中的应用[J]. 中国卫生统计, 2016,33(2):350-352. |
| [22] | 王永吉, 蔡宏伟, 夏结来 , 等. 倾向指数匹配法与Logistic回归分析方法对比研究[J]. 现代预防医学, 2011,38(12):2217-2219. |
| [23] | Challacombe BJ, Bochner BH, Dasgupta P , et al. The role of laparoscopic and robotic cystectomy in the management of muscle-invasive bladder cancer with special emphasis on cancer control and complications[J]. Eur Urol, 2011,60(4):767-775. |
| [24] | Rios GE, Lopez-Tello GJ, Martinez-Pineiro LL . Laparoscopic radical cystectomy[J]. Clin Transl Oncol, 2009,11(12):799-804. |
| [25] | Chade DC, Laudone VP, Bochner BH , et al. Oncological outcomes after radical cystectomy for bladder cancer: open versus minimally invasive approaches[J]. J Urol, 2010,183(3):862-869. |
| [26] | Liedberg F, Mansson W . Lymph node metastasis in bladder cancer[J]. Eur Urol, 2006,49(1):13-21. |
| [27] | Dotan ZA, Kavanagh K, Yossepowitch O , et al. Positive surgical margins in soft tissue following radical cystectomy for bladder cancer and cancer specific survival[J]. J Urol, 2007,178(6):2308-2312. |
| [28] | Hadjizacharia P, Stein JP, Cai J , et al. The impact of positive soft tissue surgical margins following radical cystectomy for high-grade, invasive bladder cancer[J]. World J Urol, 2009,27(1):33-38. |
| [1] | Bin LI, Han LIANG. Robotic gastrectomy: Research progress and practical challenges [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 416-422. |
| [2] | Shenmo LI, Dandan SU, Jiyu LIN, Haodong SONG, Lulin MA, Xiaofei HOU, Guoliang WANG, Hongxian ZHANG, Jianfei YE, Shudong ZHANG. Prognostic analysis of laparoscopic simultaneous radical cystectomy and nephroureterectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 961-966. |
| [3] | Lingfu ZHANG, Gang WANG, Chunsheng HOU, Long CUI, Lixin WANG, Xiaofeng LING, Zhi XU. Laparoscopic modified transcystic biliary drainage for the treatment of biliary stones and diagnosis of biliary disease [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 748-752. |
| [4] | Huanrui WANG, Shicong LAI, Haopu HU, Zehua DING, Tao XU, Hao HU. Efficacy analysis of laparoscopy combined with flexible ureteroscope in the treatment of complex ureteral stricture [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 784-788. |
| [5] | Jing QIN, Yubo ZHOU, Hongtian LI, Ying MENG, Jianmeng LIU. Nutritional status and influencing factors of breast milk vitamin A among lactating women in three regions of Chin [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 794-801. |
| [6] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [7] | Yue WEI,Lan YAO,Xi LU,Jun WANG,Li LIN,Kun-peng LIU. Evaluation of gastric emptying after drinking carbohydrates before cesarean section by gastric ultrasonography [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1082-1087. |
| [8] | Min QIU,You-long ZONG,Bin-shuai WANG,Bin YANG,Chu-xiao XU,Zheng-hui SUN,Min LU,Lei ZHAO,Jian LU,Cheng LIU,Xiao-jun TIAN,Lu-lin MA. Treatment outcome of laparoscopic partial nephrectomy in patients with renal tumors of moderate to high complexity [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 833-837. |
| [9] | Hui-li LIU,Yan-han LV,Xiao-xiao WANG,Min LI. Factors influencing the chronic post-surgical pain after laparoscopic surgery for elderly patients with urinary tract tumors [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 851-856. |
| [10] | Xiao-wei WANG,Ying-chao MU,Zhen-yu GUO,Yu-bo ZHOU,Yong ZHANG,Hong-tian LI,Jian-meng LIU. Secular trends of age at menarche and age at menopause in women born since 1951 from a county of Shandong Province, China [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 502-510. |
| [11] | Ling-fu ZHANG,Chun-sheng HOU,Zhi XU,Li-xin WANG,Xiao-feng LING,Gang WANG,Long CUI,Dian-rong XIU. Clinical effect of laparoscopic transcystic drainage combined with common bile duct exploration for the patients with difficult biliary stones [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1185-1189. |
| [12] | Li-zhe AN,Liu-lin XIONG,Liang CHEN,Huan-rui WANG,Wei-nan CHEN,Xiao-bo HUANG. Laparoscopic pyeloplasty combined with ultrasonic lithotripsy via nephroscope for treatment of ureteropelvic junction obstruction with renal calculi [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 746-750. |
| [13] | Yun-fei XING,Chun-yi LIU,Wen-ying MENG,Jie ZHANG,Ming-yuan JIAO,Lei JIN,Lei JIN. Relationship between micronutrients supplementation during periconceptional period and serum concentration of vitamin E in the 1st trimester of gestational period [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 434-442. |
| [14] | ZHANG Fan,CHEN Qu,HAO Yi-chang,YAN Ye,LIU Cheng,HUANG Yi,MA Lu-lin. Relationship between recovery of urinary continence after laparoscopic radical prostatectomy and preoperative/postoperative membranous urethral length [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 299-303. |
| [15] | ZHANG Fan,HUANG Xiao-juan,YANG Bin,YAN Ye,LIU Cheng,ZHANG Shu-dong,HUANG Yi,MA Lu-lin. Relationship between prostate apex depth and early recovery of urinary continence after laparoscopic radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 692-696. |
|
||