北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (6): 1124-1129. doi: 10.19723/j.issn.1671-167X.2020.06.023
混合现实技术在口腔颌面部肿瘤手术中的应用
唐祖南,Hui Yuh Soh,胡耒豪,于尧,章文博,彭歆( )
)
- 北京大学口腔医学院·口腔医院,口腔颌面外科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
Application of mixed reality technique for the surgery of oral and maxillofacial tumors
Zu-nan TANG,Yuh SOH Hui,Lei-hao HU,Yao YU,Wen-bo ZHANG,Xin PENG()
- Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
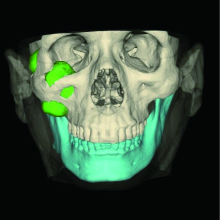
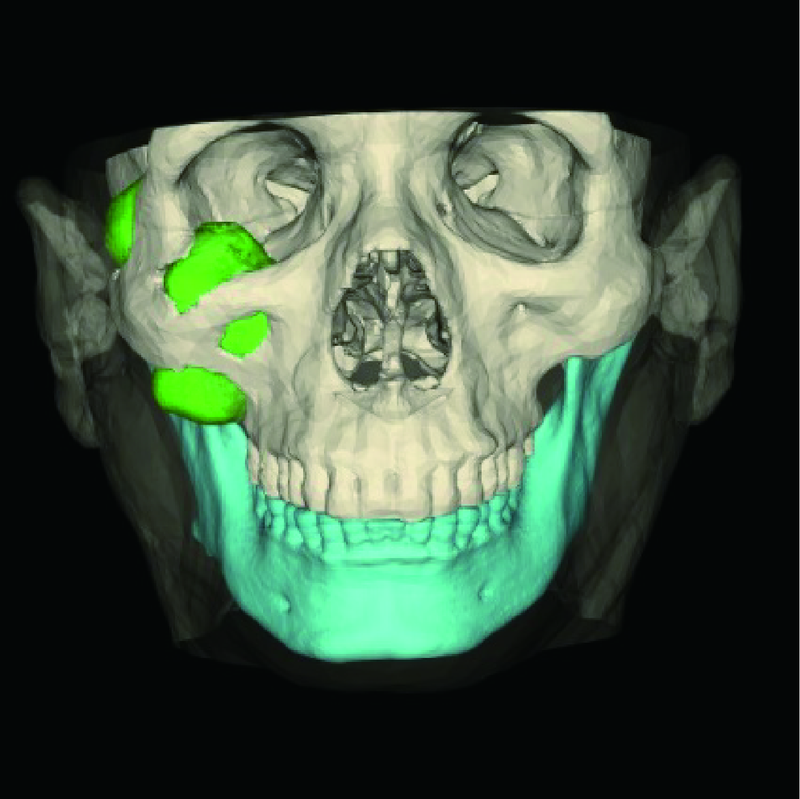
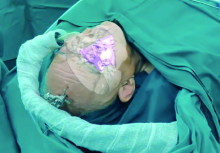
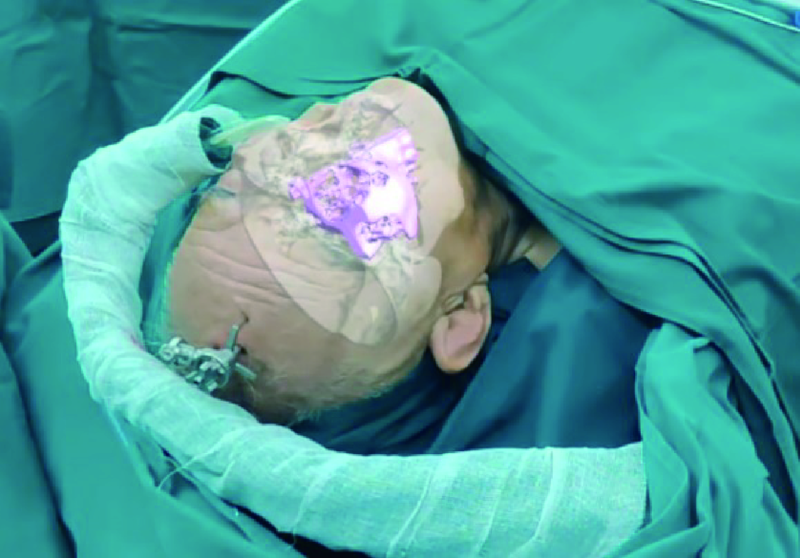
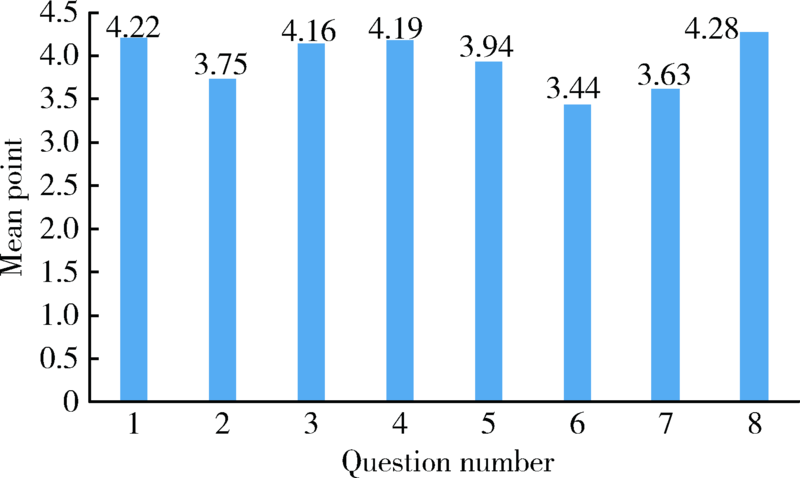
目的:探讨混合现实技术在口腔颌面部肿瘤手术中的应用价值。方法:选择2018年12月—2020年1月就诊于北京大学口腔医院口腔颌面外科需行手术治疗的肿瘤患者,将患者术前增强CT原始数据导入星图医学影像工作站(维卓致远,中国北京),分别对肿瘤、血管、骨骼等重要解剖结构进行三维模型重构,显示其术前空间关系,对重点结构进行标记,并进行术前规划。通过混合现实技术在术区立体显示三维重建模型,术者利用简单手势在术中保持无菌状态下对眼前的三维重建模型进行调整,观察肿瘤范围、大小、位置及其与周围临近重要解剖结构的关系。应用混合现实技术辅助手术进行,手术开始前进行三维模型配准,肿瘤显露过程中进行术中验证,术后利用Likert量表对混合现实技术的应用效果进行评价。结果:入选的8例患者均顺利实施了混合现实技术辅助下的肿瘤切除手术,手术过程中三维重建模型平均配准时间为12.0 min,术者在所有病例的手术中均都能直观、立体地观看肿物以及周围解剖结构的三维重建模型,并可在术中自行调整图像。Likert量表评价结果显示:在感知准确性、帮助确定解剖部位、术中图像引导作用,以及改善手术安全性的潜力方面均获得较高评分(分别为4.22、4.19、4.16和4.28分)。8例患者术后愈合良好,无手术并发症发生。结论:混合现实技术能通过三维重建模型实时立体可视化,提供术区解剖结构信息,引导和修正手术操作,提高口腔颌面部肿瘤切除手术的准确性和安全性。
中图分类号:
- R782.05


| [1] | 章文博, 于尧, 王洋, 等. 数字化外科技术在上颌骨缺损重建中的应[J]. 北京大学学报(医学版), 2017,49(1):1-5. |
| [2] |
Bouchard C, Magill JC, Nikonovskiy V, et al. Osteomark: a surgical navigation system for oral and maxillofacial surgery[J]. Int J Oral Maxillofac Surg, 2012,41(2):265-270.
doi: 10.1016/j.ijom.2011.10.017 pmid: 22103996 |
| [3] |
Haddock NT, Monaco C, Weimer KA, et al. Increasing bony contact and overlap with computer-designed offset cuts in free fibula mandible reconstruction[J]. J Craniofac Surg, 2012,23(6):1592-1595.
doi: 10.1097/SCS.0b013e318257576c pmid: 23147284 |
| [4] |
Pietruski P, Majak M, wiatek-Najwer E, et al. Navigation-guided fibula free flap for mandibular reconstruction: A proof of concept study[J]. J Plast Reconstr Aesthet Surg, 2019,72(4):572-580.
doi: 10.1016/j.bjps.2019.01.026 pmid: 30803870 |
| [5] |
Tepper OM, Rudy HL, Lefkowitz A, et al. Mixed reality with holoLens: where virtual reality meets augmented reality in the operating room[J]. Plast Reconstr Surg, 2017,140(5):1066-1070.
pmid: 29068946 |
| [6] |
Mitsuno D, Ueda K, Hirota Y, et al. Effective application of mixed reality device hololens: simple manual alignment of surgical field and holograms[J]. Plast Reconstr Surg, 2019,143(2):647-651.
doi: 10.1097/PRS.0000000000005215 pmid: 30688914 |
| [7] |
Incekara F, Smits M, Dirven C, et al. Clinical feasibility of a wearable mixed-reality device in neurosurgery[J]. World Neurosurg, 2018,118:e422-e427.
doi: 10.1016/j.wneu.2018.06.208 pmid: 30257298 |
| [8] |
Zhu H, Li Y, Wang C, et al. A first attempt of inferior vena cava filter successfully guided by a mixed-reality system: a case report[J]. J Geriatr Cardiol, 2019,16(7):575-577.
doi: 10.11909/j.issn.1671-5411.2019.07.008 pmid: 31447896 |
| [9] |
Saito Y, Sugimoto M, Imura S, et al. Intraoperative 3d hologram support with mixed reality techniques in liver surgery[J]. Ann Surg, 2020,271(1):e4-e7.
doi: 10.1097/SLA.0000000000003552 pmid: 31425293 |
| [10] | Rose AS, Kim H, Fuchs H, et al. Development of augmented-reality applications in otolaryngology-head and neck surgery[J]. Laryngoscope, 2019,129(S3):S1-S11. |
| [11] | 乔晨. 增强现实牙科虚拟手术的关键技术研究[D]. 北京理工大学, 2011. |
| [12] | 张益. 数字化外科技术及眼眶骨折精确重建[J]. 中华口腔医学杂志, 2012,47(8):463-465. |
| [13] | 于尧, 章文博, 王洋, 等. iPlan CMF软件辅助下增强CT三维重建在头颈部肿瘤治疗中的应用[J]. 北京大学学报(医学版), 2017,49(5):878-882. |
| [14] | 赵峰, 高勃, 刘震侠, 等. Dicom标准和Mimics软件辅助建立下颌骨三维有限元模型[J]. 西南国防医药, 2005,15(5):479-481. |
| [15] |
Sauer IM, Queisner M, Tang P, et al. Mixed reality in visceral surgery: development of a suitable workflow and evaluation of intraoperative use-cases[J]. Ann Surg, 2017,266(5):706-712.
doi: 10.1097/SLA.0000000000002448 pmid: 28767561 |
| [16] |
Léger É, Drouin S, Collins DL, et al. Quantifying attention shifts in augmented reality image-guided neurosurgery[J]. Healthc Technol Lett, 2017,4(5):188-192.
doi: 10.1049/htl.2017.0062 pmid: 29184663 |
| [17] |
Khor WS, Baker B, Amin K, et al. Augmented and virtual reality in surgery-the digital surgical environment: applications, limitations and legal pitfalls[J]. Ann Transl Med, 2016,4(23):454.
doi: 10.21037/atm.2016.12.23 pmid: 28090510 |
| [18] |
Gregory TM, Gregory J, Sledge J, et al. Surgery guided by mixed reality: presentation of a proof of concept[J]. Acta Orthop, 2018,89(5):480-483.
doi: 10.1080/17453674.2018.1506974 pmid: 30350756 |
| [19] |
McJunkin JL, Jiramongkolchai P, Chung W, et al. Development of a mixed reality platform for lateral skull base anatomy[J]. Otol Neurotol, 2018,39(10):e1137-e1142.
doi: 10.1097/MAO.0000000000001995 pmid: 30239435 |
| [20] | 叶哲伟, 吴星火. 混合现实技术在骨科的最新应用进展[J]. 临床外科杂志, 2018,26(1):13-14. |
| [21] |
Zhang WB, Mao C, Liu XJ, et al. Outcomes of orbital floor reconstruction after extensive maxillectomy using the computer-assisted fabricated individual titanium mesh technique[J]. J Oral Maxillofac Surg, 2015,73(10):2065.
pmid: 26188101 |
| [22] |
Sukegawa S, Kanno T, Furuki Y. Application of computer-assisted navigation systems in oral and maxillofacial surgery[J]. Jpn Dent Sci Rev, 2018,54(3):139-149.
pmid: 30128061 |
| [23] | 陈宝权, 秦学英. 混合现实中的虚实融合与人机智能交融[J]. 中国科学(信息科学), 2016,46(12):1737-1747. |
| [24] | Likert R. A technique for the measurement of attitudes[J]. Arch Psychol, 1932,22:5-55. |
| [1] | 洪洪,钱宇婷,付磊,王武,李成辉,尹毅青. 困难气道中运用CT 三维重建技术指导硬质纤维气管镜行气管插管[J]. 北京大学学报(医学版), 2019, 51(5): 870-874. |
| [2] | 陈素华,杨军,韩鸿宾,崔德华,孙建军,马长城,和清源,林国中,韩芸峰,吴超,马凯明,张一博. 弥散张量成像联合虚拟现实三维重建在功能区胶质瘤手术中的应用[J]. 北京大学学报(医学版), 2019, 51(3): 530-535. |
| [3] | 于尧, 章文博, 王洋, 刘筱菁, 郭传瑸, 俞光岩, 彭歆. iPlan CMF软件辅助下增强CT三维重建在头颈部肿瘤治疗中的应用[J]. 北京大学学报(医学版), 2017, 49(5): 878-882. |
| [4] | 赵一姣,王斯维,刘怡,王勇. 基于影像学牙周膜解剖特征快速提取活体牙三维牙根形态的方法[J]. 北京大学学报(医学版), 2017, 49(1): 54-059. |
|
||
