北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (1): 13-21. doi: 10.19723/j.issn.1671-167X.2023.01.003
369例口腔颌面部非霍奇金淋巴瘤的临床病理特点及预后
宿骞1,彭歆1,周传香2,*( ),俞光岩1,*()
),俞光岩1,*()
- 1. 北京大学口腔医学院·口腔医院口腔颌面外科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔生物材料和数字诊疗装备国家工程研究中心,口腔数字医学北京市重点实验室,国家卫生健康委员会口腔医学计算机应用工程技术研究中心,国家药品监督管理局口腔生物材料重点实验室,北京 100081
2. 北京大学口腔医学院·口腔医院口腔病理科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔生物材料和数字诊疗装备国家工程研究中心,口腔数字医学北京市重点实验室,国家卫生健康委员会口腔医学计算机应用工程技术研究中心,国家药品监督管理局口腔生物材料重点实验室,北京 100081
Clinicopathological characteristics and prognosis of non-Hodgkin lymphoma in oral and maxillofacial regions: An analysis of 369 cases
Qian SU1,Xin PENG1,Chuan-xiang ZHOU2,*(),Guang-yan YU1,*()
- 1. Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomato-logy & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
2. Department of Oral Pathology, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomato-logy & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
摘要:
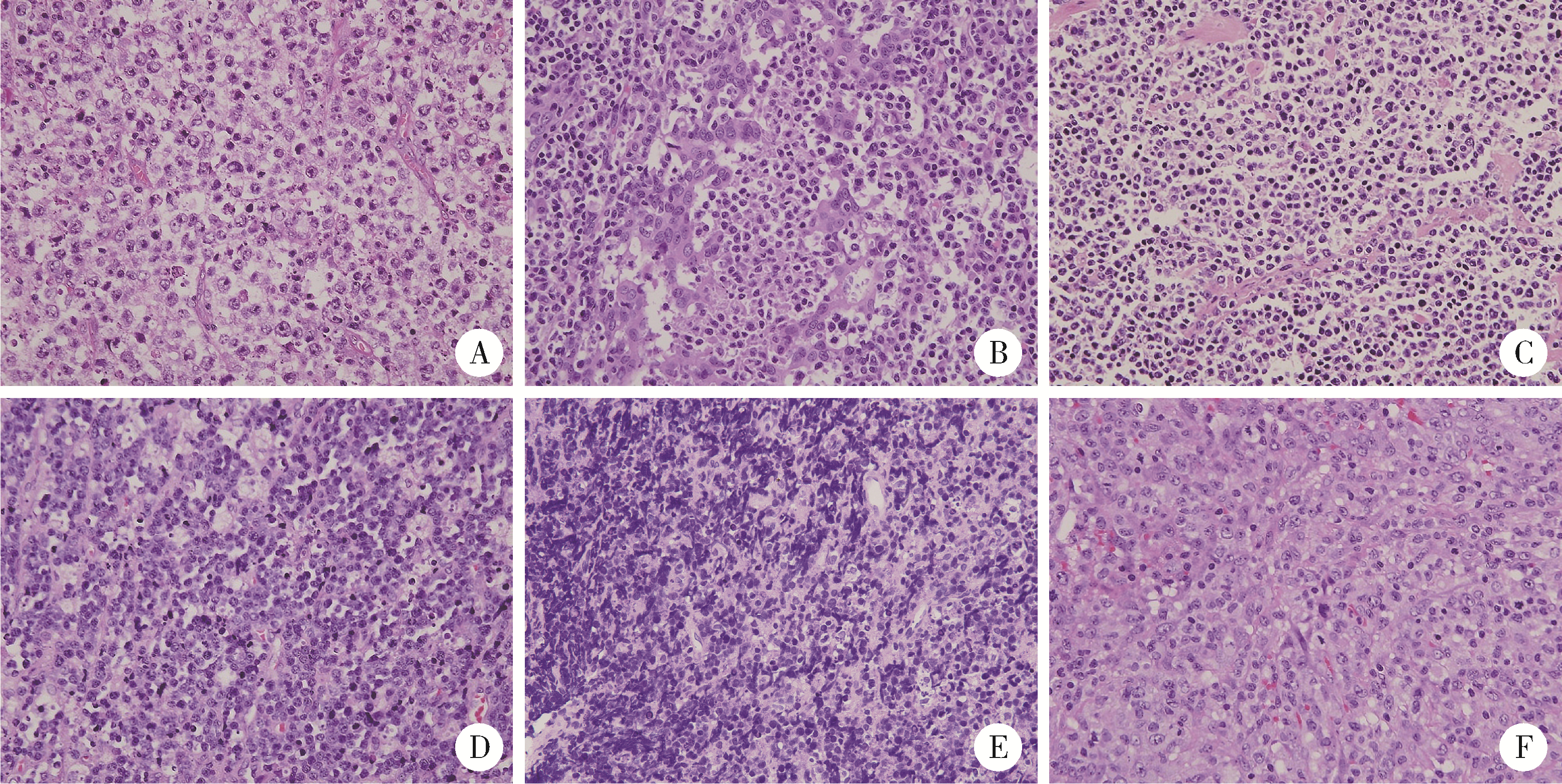
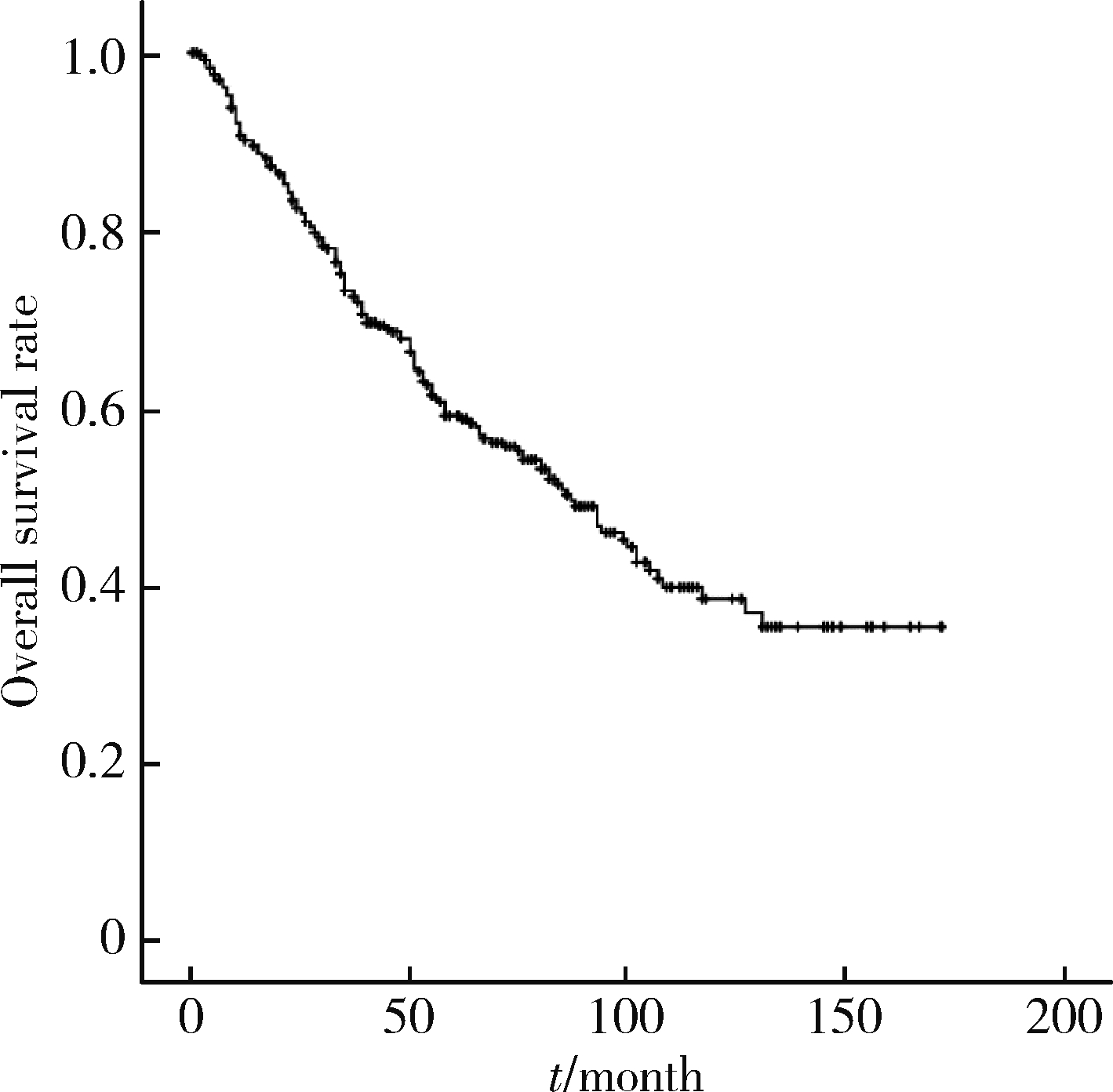
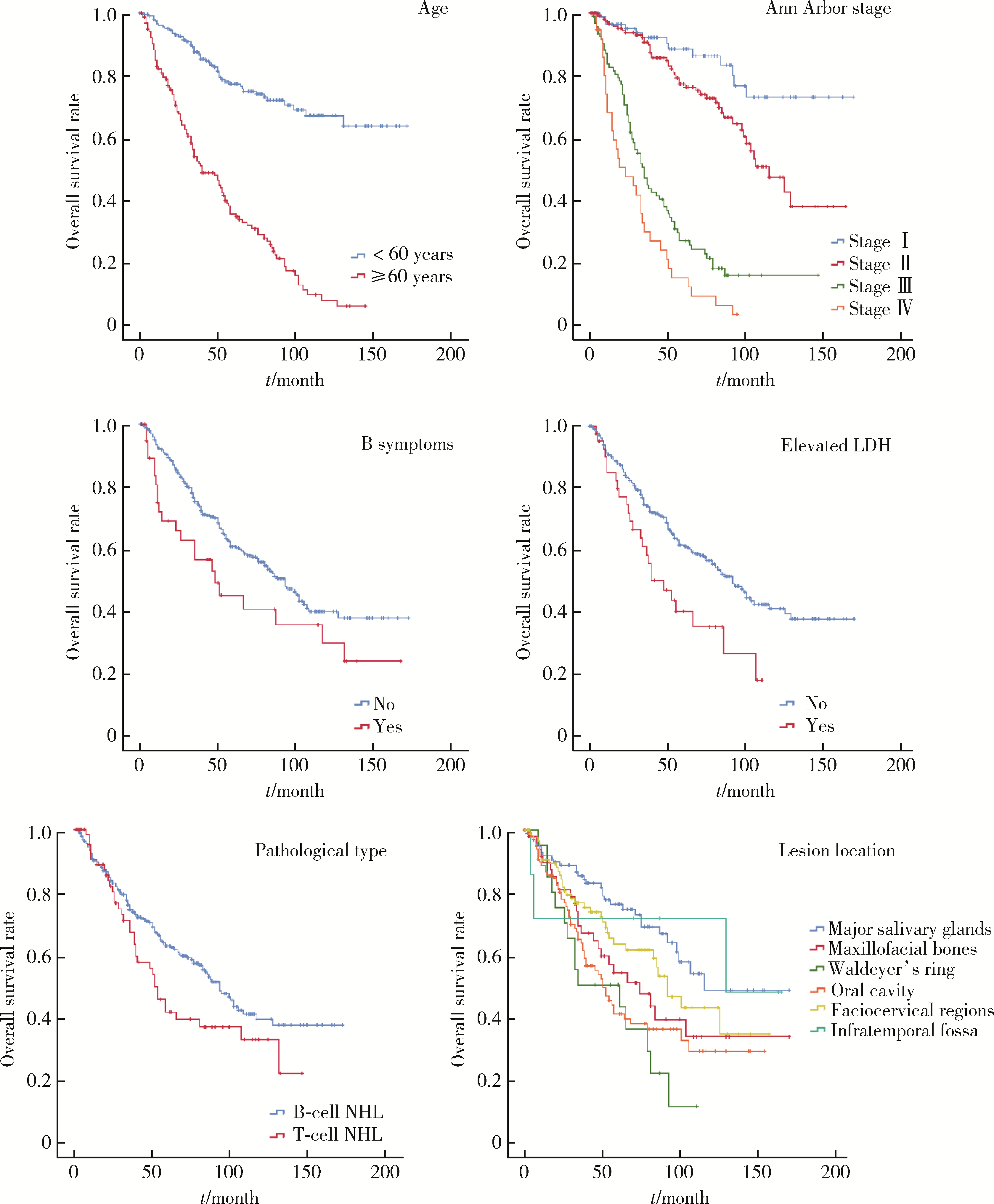
目的: 探讨口腔颌面部非霍奇金淋巴瘤(non-Hodgkin lymphoma,NHL)的临床病理特点及影响患者预后的因素。方法: 回顾性分析2008年1月至2020年6月北京大学口腔医院口腔颌面外科收治的口腔颌面部NHL患者的临床病理资料,结合随访结果,总结其临床病理特点及影响患者预后的因素。结果: 369例患者中,男性180例,女性189例;中位年龄56岁(3个月至92岁),中位病期3个月。283例患者临床表现为肿块,38例为组织溃疡坏死,48例呈软组织弥漫性肿胀。病变位于面颈部软组织者90例(颈部75例,占20.3%),大唾液腺99例(腮腺77例,占20.9%),口腔软组织103例,颌面部骨组织50例,咽部软组织20例,颞下窝7例。247例伴发颈部淋巴结肿大,仅40例伴有B症状。298例为B细胞NHL,70例为T细胞NHL。弥漫性大B细胞淋巴瘤、黏膜相关淋巴组织淋巴瘤、滤泡淋巴瘤、结外自然杀伤/T细胞淋巴瘤鼻型最常见。Ann ArborⅠ期87例、Ⅱ期138例、Ⅲ期106例、Ⅳ期38例。中位随访时间48个月,164例患者死亡,1年、2年和5年总生存率分别为90.1%、82.4%和59.9%,中位生存期为(86.00±7.98)个月。多因素分析结果显示,年龄(P < 0.001)、临床分期(P < 0.001)、血清乳酸脱氢酶升高(P=0.014)、病理分型(P=0.049)是总生存期的独立影响因素。结论: 口腔颌面部NHL具有多样化的临床表现及独特的病理类型分布,与全身性淋巴瘤存在差异。颈部软组织和腮腺为最常见的受侵部位,患者较少伴全身症状。高龄、临床晚期、伴有B症状、T细胞NHL患者的预后较差。
中图分类号:
- R739.8



| 1 | 李小秋, 李甘地, 高子芬, 等. 中国淋巴瘤亚型分布: 国内多中心性病例10 002例分析[J]. 诊断学理论与实践, 2012, 11 (2): 111- 115. |
| 2 |
Zelenetz AD , Gordon LI , Abramson JS , et al. NCCN guidelines insights: B-cell lymphomas, version 3.2019[J]. J Natl Compr Canc Netw, 2019, 17 (6): 650- 661.
doi: 10.6004/jnccn.2019.0029 |
| 3 |
Skarin AT , Dorfman DM . Non-Hodgkin's lymphomas: Current classification and management[J]. CA Cancer J Clin, 1997, 47 (6): 351- 372.
doi: 10.3322/canjclin.47.6.351 |
| 4 | Swerdlow SH , Campo E , Harris NL , et al. WHO classification of tumours of haematopoietic and lymphoid tissues[M]. Lyon: IARC Press, 2008. |
| 5 |
Siegel RL , Miller KD , Fuchs HE , et al. Cancer satistics, 2021[J]. CA Cancer J Clin, 2021, 71 (1): 7- 33.
doi: 10.3322/caac.21654 |
| 6 |
Sung H , Ferlay J , Siegel RL , et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71 (3): 209- 249.
doi: 10.3322/caac.21660 |
| 7 |
庹吉妤, 张敏, 郑荣寿, 等. 2015年中国恶性淋巴瘤发病与死亡分析[J]. 中国肿瘤, 2021, 30 (1): 35- 40.
doi: 10.3969/j.issn.1000-8179.2021.01.726 |
| 8 |
温玉明, 代晓明, 王昌美, 等. 口腔颌面部恶性肿瘤6 539例临床病理分析[J]. 华西口腔医学杂志, 2001, 19 (5): 296- 299.
doi: 10.3321/j.issn:1000-1182.2001.05.008 |
| 9 |
Swerdlow SH , Campo E , Pileri SA , et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms[J]. Blood, 2016, 127 (20): 2375- 2390.
doi: 10.1182/blood-2016-01-643569 |
| 10 | The 2022 global patient survey on lymphoma & CLL. https://lymphomacoalition.org/wp-content/uploads/LC-2020-GPS-Global-Re-port-Final.pdf[Z]. Lymphoma Coalition, 2020. |
| 11 |
肖畅, 苏祖兰, 吴秋良, 等. 根据WHO新分类对493例非霍奇金淋巴瘤的临床病理分析[J]. 中华病理学杂志, 2005, 34 (1): 22- 27.
doi: 10.3760/j.issn:0529-5807.2005.01.007 |
| 12 |
Etemad-Moghadam S , Tirgary F , Keshavarz S , et al. Head and neck non-Hodgkin's lymphoma: A 20-year demographic study of 381 cases[J]. Int J Oral Maxillofac Surg, 2010, 39 (9): 869- 872.
doi: 10.1016/j.ijom.2010.03.029 |
| 13 |
Aoki R , Karube K , Sugita Y , et al. Distribution of malignant lymphoma in Japan: Analysis of 2 260 cases, 2001-2006[J]. Pathol Int, 2008, 58 (3): 174- 182.
doi: 10.1111/j.1440-1827.2007.02207.x |
| 14 | 杨小芸, 沈丽达, 龙庭凤, 等. 1 326例非霍奇金淋巴瘤临床病理特点分析[J]. 中华肿瘤防治杂志, 2016, 23 (9): 605- 609. |
| 15 |
Feinstein AJ , Ciarleglio MM , Cong X , et al. Parotid gland lymphoma: Prognostic analysis of 2 140 patients[J]. The Laryngoscope, 2013, 123 (5): 1199- 1203.
doi: 10.1002/lary.23901 |
| 16 | El-Naggar A , John K , Grandis J . WHO classification of head and neck tumours. WHO classification of tumours of the salivary glands[J]. Lyon: IARC Press, 2017, 160- 184. |
| 17 |
周立强, 孙燕, 谭文勇, 等. 非霍奇金淋巴瘤1 125例临床病理分析[J]. 癌症进展, 2006, 4 (5): 391- 397.
doi: 10.3969/j.issn.1672-1535.2006.05.004 |
| 18 |
Jaffe ES . Diagnosis and classification of lymphoma: Impact of technical advances[J]. Semin Hematol, 2019, 56 (1): 30- 36.
doi: 10.1053/j.seminhematol.2018.05.007 |
| 19 |
Salles G , Barrett M , Foà R , et al. Rituximab in B-cell hematologic malignancies: A review of 20 years of clinical experience[J]. Adv Ther, 2017, 34 (10): 2232- 2273.
doi: 10.1007/s12325-017-0612-x |
| 20 |
Berger GK , Mcbride A , Lawson S , et al. Brentuximab vedotin for treatment of non-Hodgkin lymphomas: A systematic review[J]. Crit Rev Oncol Hematol, 2017, 109, 42- 50.
doi: 10.1016/j.critrevonc.2016.11.009 |
| 21 |
Allemani C , Matsuda T , Di Carlo V , et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries[J]. Lancet, 2018, 391 (10125): 1023- 1075.
doi: 10.1016/S0140-6736(17)33326-3 |
| 22 | 马肖容, 徐燕, 王瑾, 等. 254例非霍奇金淋巴瘤的临床疗效与预后分析[J]. 中国实验血液学杂志, 2016, 24 (4): 1044- 1050. |
| 23 |
Cheson BD , Fisher RI , Barrington SF , et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification[J]. J Clin Oncol, 2014, 32 (27): 3059- 3068.
doi: 10.1200/JCO.2013.54.8800 |
| 24 | Chen SY , Yang Y , Qi SN , et al. Validation of nomogram-revised risk index and comparison with other models for extranodal nasal-type NK/T-cell lymphoma in the modern chemotherapy era: Indication for prognostication and clinical decision-making[J]. Leukemia, 2021, 35 (1): 130- 142. |
| 25 | Ruppert AS , Dixon JG , Salles G , et al. International prognostic indices in diffuse large B-cell lymphoma: A comparison of IPI, R-IPI, and NCCN-IPI[J]. Blood, 2020, 135 (23): 2041- 2048. |
| [1] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [2] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [3] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [4] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [5] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
| [6] | 曾媛媛,谢云,陈道南,王瑞兰. 脓毒症患者发生正常甲状腺性病态综合征的相关因素[J]. 北京大学学报(医学版), 2024, 56(3): 526-532. |
| [7] | 苏俊琪,王晓颖,孙志强. 舌鳞状细胞癌根治性切除术后患者预后预测列线图的构建与验证[J]. 北京大学学报(医学版), 2024, 56(1): 120-130. |
| [8] | 李建斌,吕梦娜,池强,彭一琳,刘鹏程,吴锐. 干燥综合征患者发生重症新型冠状病毒肺炎的早期预测[J]. 北京大学学报(医学版), 2023, 55(6): 1007-1012. |
| [9] | 刘欢锐,彭祥,李森林,苟欣. 基于HER-2相关基因构建风险模型用于膀胱癌生存预后评估[J]. 北京大学学报(医学版), 2023, 55(5): 793-801. |
| [10] | 薛子璇,唐世英,邱敏,刘承,田晓军,陆敏,董靖晗,马潞林,张树栋. 青年肾肿瘤伴瘤栓的临床病理特征及预后分析[J]. 北京大学学报(医学版), 2023, 55(5): 802-811. |
| [11] | 卢汉,张建运,杨榕,徐乐,李庆祥,郭玉兴,郭传瑸. 下颌牙龈鳞状细胞癌患者预后的影响因素[J]. 北京大学学报(医学版), 2023, 55(4): 702-707. |
| [12] | 时云飞,王豪杰,刘卫平,米岚,龙孟平,刘雁飞,赖玉梅,周立新,刁新婷,李向红. 血管免疫母细胞性T细胞淋巴瘤临床与分子病理学特征分析[J]. 北京大学学报(医学版), 2023, 55(3): 521-529. |
| [13] | 王哲,孙伟,杨雪,宋颖,姬爱平,白洁. 口腔急诊颌面部感染患者临床分析[J]. 北京大学学报(医学版), 2023, 55(3): 543-547. |
| [14] | 朱晓娟,张虹,张爽,李东,李鑫,徐玲,李挺. 人表皮生长因子受体2低表达乳腺癌的临床病理学特征及预后[J]. 北京大学学报(医学版), 2023, 55(2): 243-253. |
| [15] | 赖玉梅,李忠武,李欢,吴艳,时云飞,周立新,楼雨彤,崔传亮. 68例肛管直肠黏膜黑色素瘤临床病理特征及预后[J]. 北京大学学报(医学版), 2023, 55(2): 262-269. |
|
||
