北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (6): 1115-1121. doi: 10.19723/j.issn.1671-167X.2021.06.018
有幽门螺杆菌感染家族史儿童胃部菌群的特点
王子靖,李在玲( )
)
- 北京大学第三医院儿科, 北京 100191
Characteristics of gastric microbiota in children with Helicobacter pylori infection family history
WANG Zi-jing,LI Zai-ling()
- Department of Pediatric, Peking University Third Hospital, Beijing 100191, China
摘要:
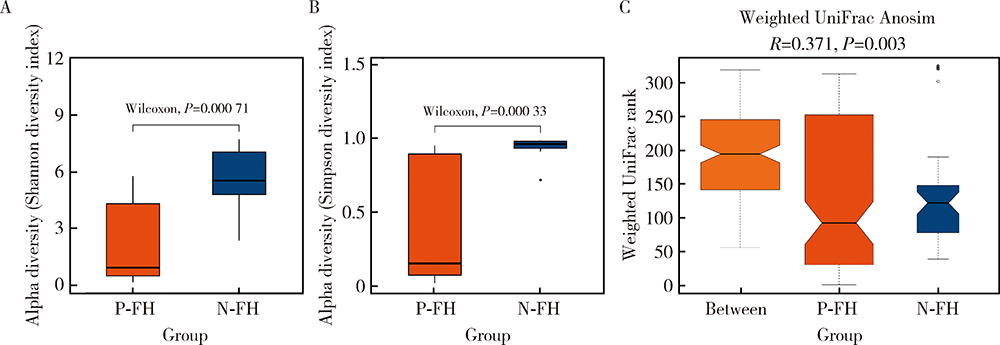
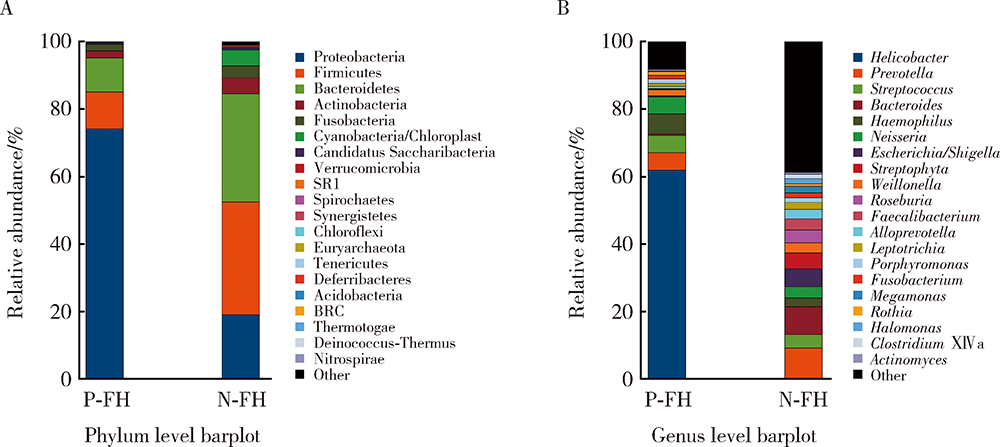
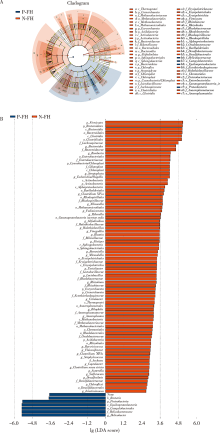
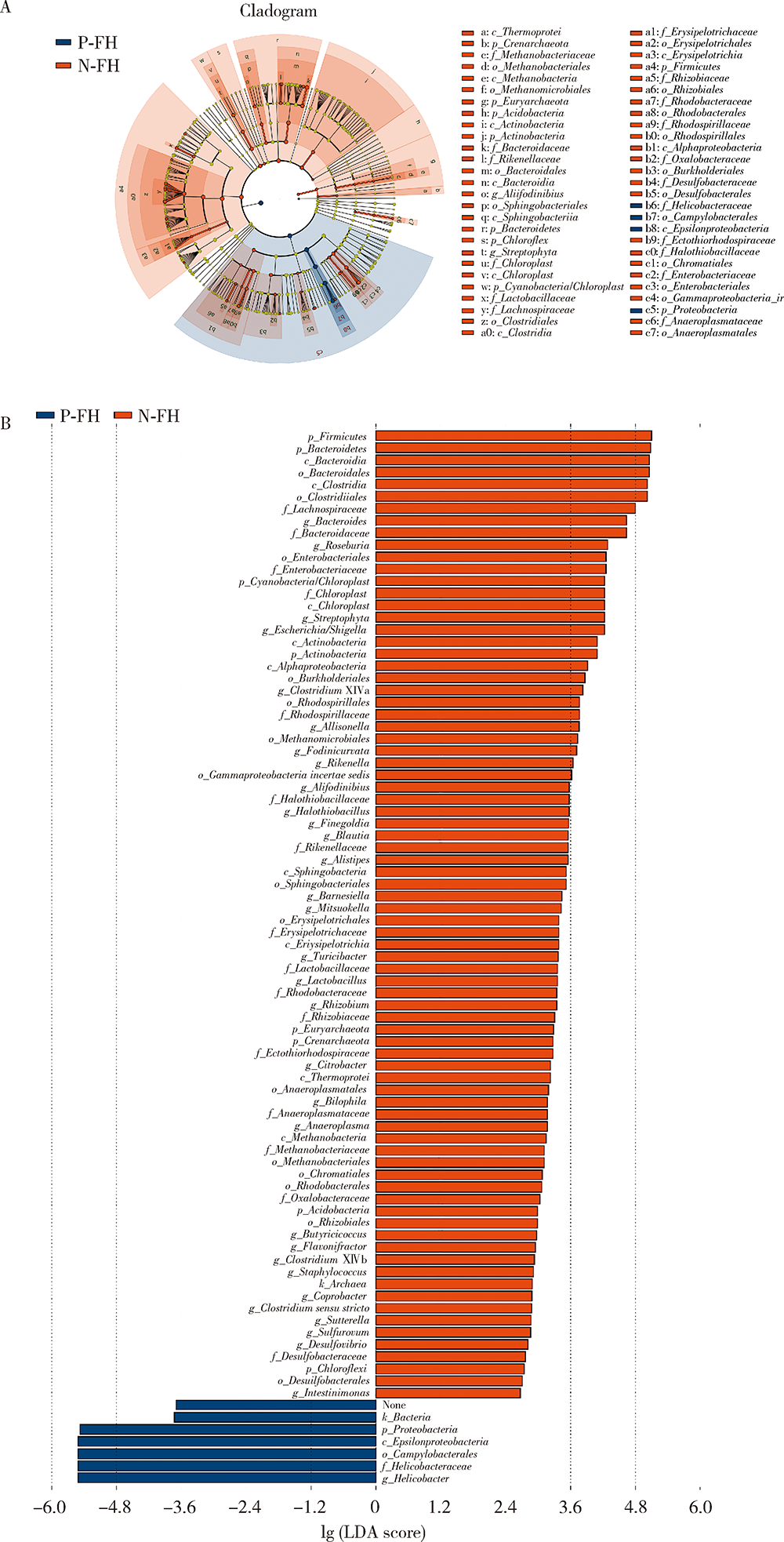
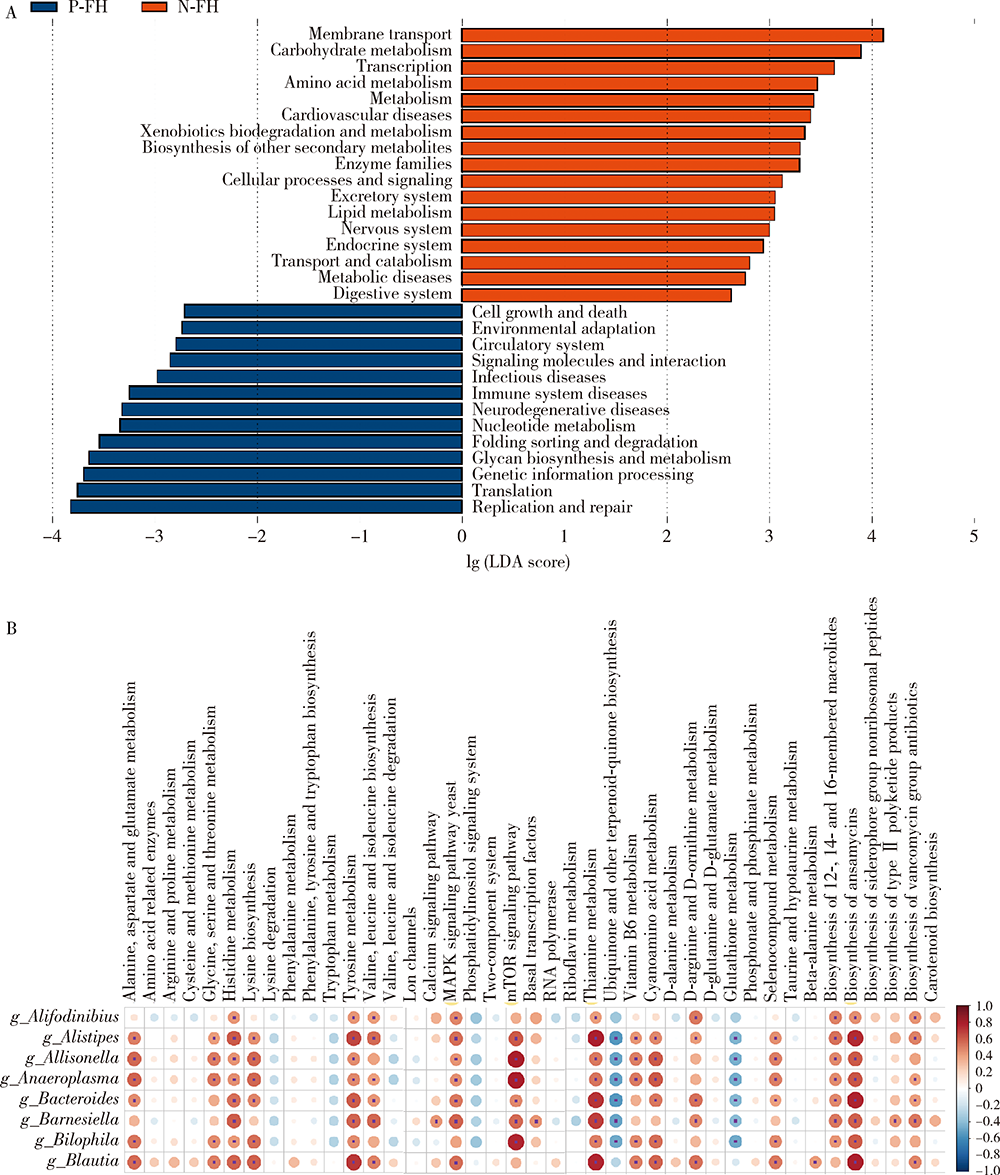
目的:探究有幽门螺杆菌(Helicobacter pylori, H. pylori)感染家族史,发生和未发生H. pylori感染的儿童胃部菌群特点。方法:分别采集患儿胃体和胃窦的黏膜标本,通过标本DNA提取、16S核糖体DNA(ribosomal DNA,rDNA)V3-V4区域PCR扩增、高通量测序、数据处理等步骤后,得到胃部黏膜菌群分析结果,将结果中有H. pylori感染家族史的标本根据是否发生H. pylori感染分为感染组(n=18)和非感染组(n=24),比较两组间菌群的α和β多样性、菌群丰度变化等指标,找出差异菌群,并对菌群功能进行预测分析。结果:感染组与非感染组胃部菌群α多样性和β多样性之间差异有统计学意义(P<0.05), 感染组的菌群多样性要低于非感染组。菌群相对丰度方面,门水平占优势的主要有变形菌门(Proteobacteria)、厚壁菌门(Firmicutes)、拟杆菌门(Bacteroidetes)、放线菌门(Actinobacteria)和梭杆菌门(Fusobacteria);属水平上,非感染组中拟杆菌(Bacteroides)、普雷沃氏菌(Prevotella)、链球菌(Streptococcus)和奈瑟菌(Neisseria)为优势菌种。差异物种方面,通过LEfSe分析,发现非感染组中属水平的拟杆菌属等的相对丰度显著高于感染组。功能预测发现,拟杆菌属与一些氨基酸和维生素代谢、丝裂原活化蛋白激酶(mitogen-activated protein kinase,MAPK)、哺乳动物雷帕霉素靶蛋白(mammalian target of rapamycin, mTOR)信号通路、安沙霉素(ansamycin)的合成相关通路均呈显著正相关。结论:有H. pylori感染家族史的儿童中,发生H. pylori感染和未发生感染者的胃部菌群存在显著差异,拟杆菌可能与儿童是否发生H. pylori感染存在关联。
中图分类号:
- R725.7



| [1] | Misak Z, Hojsak I, Homan M. Review: Helicobacter pylori in pediatrics[J]. Helicobacter, 2019, 24(Suppl 1):e12639. |
| [2] |
Weyermann M, Rothenbacher D, Brenner H. Acquisition of Helicobacter pylori infection in early childhood: Independent contributions of infected mothers, fathers, and siblings[J]. Am J Gastroenterol, 2009, 104(1):182-189.
doi: 10.1038/ajg.2008.61 pmid: 19098867 |
| [3] |
Ueno T, Suzuki H, Hirose M, et al. Influence of living environment during childhood on Helicobacter pylori infection in Japanese young adults[J]. Digestion, 2020, 101(6):779-784.
doi: 10.1159/000502574 |
| [4] |
Polk DB, Peek RM. Helicobacter Pylori: Gastric cancer and beyond[J]. Nat Rev Cancer, 2010, 10(6):403-414.
doi: 10.1038/nrc2857 |
| [5] |
Waskito LA, Salama NR, Yamaoka Y. Pathogenesis of Helicobac-ter pylori infection[J]. Helicobacter, 2018, 23(Suppl 1):e12516.
doi: 10.1111/hel.2018.23.issue-S1 |
| [6] |
Yan R, Guo Y, Gong Q, et al. Microbiological evidences for gastric cardiac microflora dysbiosis inducing the progression of inflammation[J]. J Gastroenterol Hepatol, 2020, 35(6):1032-1041.
doi: 10.1111/jgh.v35.6 |
| [7] | 中华医学会儿科学分会消化学组, 《中华儿科杂志》编辑委员会. 儿童幽门螺杆菌感染诊治专家共识[J]. 中华儿科杂志, 2015, 53(7):496-498. |
| [8] |
Llorca L, Pérez-Pérez G, Urruzuno P, et al. Characterization of the gastric microbiota in a pediatric population according to Helicobacter pylori status[J]. Pediatr Infect Dis J, 2017, 36(2):173-178.
doi: 10.1097/INF.0000000000001383 pmid: 27820723 |
| [9] | 彭贤慧, 周丽雅, 何利华, 等. 幽门螺杆菌感染者胃内菌群特征分析[J]. 胃肠病学和肝病学杂志, 2017, 26(6):658-663. |
| [10] |
Bik EM, Eckburg PB, Gill SR, et al. Molecular analysis of the bacterial microbiota in the human stomach[J]. Proc Natl Acad Sci U S A, 2006, 103(3):732-737.
doi: 10.1073/pnas.0506655103 |
| [11] | Bruno G, Rocco G, Zaccari P, et al. Helicobacter pylori infection and gastric dysbiosis: Can probiotics administration be useful to treat this condition?[J]. Can J Infect Dis Med Microbiol, 2018, 2018:6237239. |
| [12] | Delgado S, Leite AM, Ruas-Madiedo P, et al. Probiotic and technological properties of Lactobacillus spp. strains from the human stomach in the search for potential candidates against gastric microbial dysbiosis[J]. Front Microbiol, 2015, 5:766. |
| [13] |
Ascencio F, Gama NL, Philippis RD, et al. Effectiveness of Cyanothece spp. and Cyanospira capsulata exocellular polysaccharides as antiadhesive agents for blocking attachment of Helicobacter pylori to human gastric cells[J]. Folia Microbiol (Praha), 2004, 49(1):64-70.
doi: 10.1007/BF02931648 |
| [14] | Lorca GL, Wadstrom T, Valdez GF, et al. Lactobacillus acidophilus autolysins inhibit Helicobacter pylori in vitro[J]. Curr Micro-biol, 2001, 42(1):39-44. |
| [15] |
Nedenskov P. Nutritional requirements for growth of Helicobacter pylori[J]. Appl Environ Microbiol, 1994, 60(9):3450-3453.
doi: 10.1128/aem.60.9.3450-3453.1994 |
| [16] | Hayashi S, Sugiyama T, Asaka M, et al. Modification of Helicobacter pylori adhesion to human gastric epithelial cells by antiadhesion agents[J]. Dig Dis Sci, 1998, 43(Suppl 9):56S-60S. |
| [17] |
Dunne C, Dolan B, Clyne M. Factors that mediate colonization of the human stomach by Helicobacter pylori[J]. World J Gastroenterol, 2014, 20(19):5610-5624.
doi: 10.3748/wjg.v20.i19.5610 |
| [18] |
Slomiany BL, Slomiany A. Involvement of p38 MAPK-dependent activator protein (AP-1) activation in modulation of gastric mucosal inflammatory responses to Helicobacter pylori by ghrelin[J]. Inflammopharmacology, 2013, 21(1):67-78.
doi: 10.1007/s10787-012-0141-9 pmid: 22669511 |
| [1] | 高嘉琪, 李文鹏, 李晓怡, 谭音希, 李奕昕, 段丽萍, 吴涛, 陈大方, 胡永华, 王梦莹. 基于可穿戴设备的老年人身体活动模式与肠道菌群的关联[J]. 北京大学学报(医学版), 2026, 58(3): 551-559. |
| [2] | 温倩颖, 张丽卿, 秦安霖, 李小峰. 无症状高尿酸血症患者小肠细菌过度生长及炎症细胞因子表达水平[J]. 北京大学学报(医学版), 2026, 58(2): 313-318. |
| [3] | 魏竞尧, 叶菊香, 周美玲, 付伟伟, 刘鑫, 翟康乐, 石岩岩, 丁士刚, 张静. 原发性胃淋巴瘤的内镜特征分析及疗效预测[J]. 北京大学学报(医学版), 2026, 58(2): 342-350. |
| [4] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [5] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [6] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [7] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [8] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [9] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [10] | 付玮, 宁静, 付伟伟, 张静, 丁士刚. CMTM6对幽门螺杆菌感染的胃上皮细胞中PD-L1的作用[J]. 北京大学学报(医学版), 2025, 57(2): 245-252. |
| [11] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
| [12] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [13] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [14] | 赵双云, 邹思雨, 李雪莹, 沈丽娟, 周虹. 中文版口腔健康素养量表简版(HeLD-14)在学龄前儿童家长中应用的信度和效度评价[J]. 北京大学学报(医学版), 2024, 56(5): 828-832. |
| [15] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
|
||
