北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (1): 153-160. doi: 10.19723/j.issn.1671-167X.2022.01.024
老年流感肺炎的临床特征及D-二聚体与疾病严重程度的相关性
李佳1,徐钰2,王优雅3,高占成3,△( )
)
- 1.北京大学人民医院急诊科,北京 100044
2.北京积水潭医院呼吸与危重症医学科,北京 100035
3.北京大学人民医院呼吸与危重症医学科,北京 100044
Clinical characteristics of influenza pneumonia in the elderly and relationship between D-dimer and disease severity
LI Jia1,XU Yu2,WANG You-ya3,GAO Zhan-cheng3,△()
- 1. Department of Emergency, Peking University People’s Hospital, Beijing 100044, China
2. Department of Pulmonary and Critical Care Medicine, Beijing Jishuitan Hospital, Beijing 100035, China
3. Department of Pulmonary and Critical Care Medicine, Peking University People’s Hospital, Beijing 100044, China
摘要:
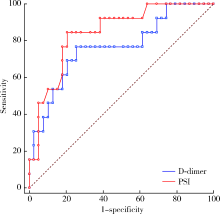
目的: 研究老年流感肺炎的临床特征以及D-二聚体与流感肺炎严重程度的相关性,以期提高临床医生对此类肺炎的甄别和管理。方法: 回顾性收集2014年起连续5个流感季(当年10月1日至次年3月31日)于北京大学人民医院诊断为流感肺炎的住院患者,年龄>65岁,收集患者的一般资料、临床症状、实验室检查、治疗方式及预后,比较重症和非重症肺炎的临床特点,分析D-二聚体与肺炎严重程度的关系,并应用受试者工作特征(receiver operating characteristic, ROC)曲线评估其预测流感肺炎死亡的效能。结果: 共纳入实验室确诊的老年流感肺炎住院患者52例,男性31例(59.6%),平均年龄(77.1±7.4)岁,符合重症肺炎诊断标准者19例(36.5%),约70%病例出现不同程度发热,重症肺炎组与非重症肺炎组相比,呼吸困难的发生率差异有统计学意义(14/19例,73.7% vs. 10/33例,30.3%,P=0.004),重症肺炎组的CURB-65(confusion, urea, respiratory rate, blood pressure, and age>65)评分、肺炎严重度指数(pneumonia severity index, PSI)评分、C反应蛋白、乳酸脱氢酶、尿素氮、空腹血糖、D-二聚体均高于非重症肺炎组,两组间差异有统计学意义(P值分别为0.004、<0.001、<0.001、0.003、0.038、0.018、<0.001),重症肺炎组的白蛋白则低于非重症肺炎组[(35.8±5.6) g/L vs. (38.9±3.5) g/L, t=-2.348,P=0.018]。入院首次检测的D-二聚体与PSI评分呈显著正相关(r=0.540, 95%CI:0.302~0.714,P<0.001),与氧合指数呈显著负相关(r=-0.559, 95%CI:-0.726-~0.330,P<0.001)。以患者是否住院期间死亡绘制ROC曲线,D-二聚体曲线下面积为0.765(95%CI:0.627~0.872),PSI曲线下面积为0.843(95%CI:0.716~0.929),二者相比,检验效能差异无统计学意义(Z=2.360,P=0.174)。D-二聚体>1 225 μg/L预测流感肺炎住院期间死亡的敏感性为76.92%,特异性为74.36%。结论: 高龄老年流感肺炎患者的发热症状不典型,呼吸困难是重症肺炎的突出表现,D-二聚体升高与老年流感肺炎严重程度相关,D-二聚体>1 200 μg/L对于老年重症流感肺炎住院期间死亡具有较好的预测价值。
中图分类号:
- R563.1



| [1] |
Luliano AD, Roguski KM, Chang HH, et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study[J]. Lancet, 2018, 391(10127):1285-1300.
doi: 10.1016/S0140-6736(17)33293-2 |
| [2] |
Gefenaite G, Pistol A, Popescu R, et al. Estimating burden of influenza-associated influenza-like illness and severe acute respiratory infection at public healthcare facilities in Romania during the 2011/12-2015/16 influenza seasons[J]. Influenza Other Respir Viruses, 2018, 12(1):183-192.
doi: 10.1111/irv.2018.12.issue-1 |
| [3] |
Loubet P, Samihlenzi N, Galtier F, et al. Factors associated with poor outcomes among adults hospitalized for influenza in France: A three-year prospective multicenter study[J]. J Clin Virol, 2016, 79:68-73.
doi: S1386-6532(16)30069-5 pmid: 27105315 |
| [4] | 中华人民共和国国家健康委员会. 流行性感冒诊疗方案(2018年版修订版)[J]. 中华临床感染病杂志, 2019, 12(1):1-5. |
| [5] | 中华医学会呼吸病学分会. 中国成人社区获得性肺炎诊断和治疗指南(2016年版)[J]. 中华结核和呼吸杂志, 2016, 39(4):253-279. |
| [6] | 中华医学会血液学分会血栓与止血学组. 弥散性血管内凝血诊断中国专家共识(2017年版)[J]. 中华血液学杂志, 2017, 38(5):361-363. |
| [7] | Palevsky PM, Liu KD, Brophy PD, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for acute kidney injury[J]. Am J Kindney Dis, 2013, 61(5):649-672. |
| [8] |
Dellinger RP, Levy MM, Carlet JM, et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2008[J]. Crit Care Med, 2008, 36(1):296-327.
pmid: 18158437 |
| [9] |
Fan E, Brodie D, Slutsky AS. Acute respiratory distress syndrome: Advances in diagnosis and treatment[J]. JAMA, 2018, 319(7):698-710.
doi: 10.1001/jama.2017.21907 |
| [10] |
Childs A, Zullo AR, Joyce NR, et al. The burden of respiratory infections among older adults in long-term care: A systematic review[J]. BMC Geriatr, 2019, 19(1):210.
doi: 10.1186/s12877-019-1236-6 |
| [11] |
Chow EJ, Doyle JD, Uyeki TM. Influenza virus-related critical illness: prevention, diagnosis, treatment[J]. Crit Care, 2019, 23(1):214.
doi: 10.1186/s13054-019-2491-9 |
| [12] | Czaja CA, Miller L, Alden N, et al. Age-related differences in hospitalization rates, clinical presentation, outcomes among older adults hospitalized with influenza: U.S. Influenza Hospitalization Surveillance Network(FluSurv-NET)[J]. Open Forum Infect Dis, 2019, 6(7): ofz225. |
| [13] |
Matsuno O, Kataoka H, Takenaka R, et al. Influence of age on symptoms and laboratory findings at presentation in patients with influenza-associated pneumonia[J]. Arch Gerontol Geriatr, 2009, 49(2):322-325.
doi: 10.1016/j.archger.2008.11.015 |
| [14] |
Talbot HK. Influenza in older adults[J]. Infect Dis Clin North Am, 2017, 31(4):757-766.
doi: 10.1016/j.idc.2017.07.005 |
| [15] |
Aronen M, Viikari L, Kohonen I, et al. Respiratory tract virus infections in the elderly with pneumonia[J]. BMC Geriatrics, 2019, 19(1):111.
doi: 10.1186/s12877-019-1125-z pmid: 30991957 |
| [16] |
Chung JY, Hsu CC, Chen JH, et al. Shock index predicted mortality in geriatric patients with influenza in the emergency department[J]. Am J Emerg Med, 2019, 37(3):391-394.
doi: 10.1016/j.ajem.2018.05.059 |
| [17] |
van Asten L, Luna Pinzon A, de Lange DW, et al. Estimating severity of influenza epidemics from severe acute respiratory infections (SARI) in intensive care units[J]. Crit Care, 2018, 22(1):351.
doi: 10.1186/s13054-018-2274-8 |
| [18] |
Zhou F, Li H, Gu L, et al. Risk factors for nosocomial infection among hospitalised severe influenza A(H1N1)pdm09 patients[J]. Resp Med, 2018, 134:86-91.
doi: 10.1016/j.rmed.2017.11.017 |
| [19] |
Sahuquillo JM, Menéndez R, Méndez R, et al. Age-related risk factors for bacterial aetiology in community-acquired pneumonia[J]. Respirology, 2016, 21(8):1472-1479.
doi: 10.1111/resp.12851 pmid: 27417291 |
| [20] |
Daoud A, Laktineh A, Macrander C, et al. Pulmonary complications of influenza infection: A targeted narrative review[J]. Postgrad Med, 2019, 131(5):299-308.
doi: 10.1080/00325481.2019.1592400 pmid: 30845866 |
| [21] |
Nguyen JL, Yang W, Ito K, et al. Seasonal influenza infections and cardiovascular disease mortality[J]. JAMA Cardiol, 2016, 1(3):274-281.
doi: 10.1001/jamacardio.2016.0433 |
| [22] |
Kilic H, Kanbay A, Karalezli A, et al. Clinical characteristics of 75 pandemic H1N1 influenza patients from Turkey; risk factors for fatality[J]. Turk J Med Sci, 2015, 45(3):562-567.
doi: 10.3906/sag-1401-111 |
| [23] |
Ma S, Lai X, Chen Z, et al. Clinical characteristics of critically ill patients co-infected with SARS-CoV-2 and the influenza virus in Wuhan, China[J]. Int J Infect Dis, 2020, 96(1):683-687.
doi: 10.1016/j.ijid.2020.05.068 |
| [24] |
Zhang L, Yan X, Fan Q, et al. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19[J]. J Thromb Haemost, 2020, 18(6):1324-1329.
doi: 10.1111/jth.v18.6 |
| [25] |
Wang ZF, Su F, Lin XJ, et al. Serum D-dimer changes and prognostic implication in 2009 novel influenza A(H1N1)[J]. Thromb Res, 2011, 127(3):198-201.
doi: 10.1016/j.thromres.2010.11.032 pmid: 21216444 |
| [26] |
Kim MA, Park JS, Lee CW, et al. Pneumonia severity index in viral community acquired pneumonia in adults[J]. PLoS One, 2019, 14(3):e0210102.
doi: 10.1371/journal.pone.0210102 |
| [27] |
Dominguez-Cherit G, De la Torre A, Rishu A, et al. Influenza A(H1N1pdm09)-related critical illness and mortality in Mexico and Canada, 2014[J]. Crit Care Med, 2016, 44(10):1861-1870.
doi: 10.1097/CCM.0000000000001830 pmid: 27359085 |
| [1] | 吴音格, 黄旸木. 基于层次-K均值混合聚类法的中国人乳头瘤病毒疫苗双边国际合作优先程度评估[J]. 北京大学学报(医学版), 2026, 58(3): 446-454. |
| [2] | 许春春, 简伟研. 基于中国家庭追踪调查的居民主观认知、收入变化与就医点选择转移的关联[J]. 北京大学学报(医学版), 2026, 58(3): 455-463. |
| [3] | 高嘉琪, 李文鹏, 李晓怡, 谭音希, 李奕昕, 段丽萍, 吴涛, 陈大方, 胡永华, 王梦莹. 基于可穿戴设备的老年人身体活动模式与肠道菌群的关联[J]. 北京大学学报(医学版), 2026, 58(3): 551-559. |
| [4] | 张晓悦, 杨晓晨, 林昊翔, 纪颖, 曹望楠, 常春. 基于保护动机理论的我国18~44岁成年人电子烟戒断意愿和戒断行为的影响因素[J]. 北京大学学报(医学版), 2026, 58(3): 575-583. |
| [5] | 袁思妍, 闵鹤葳, 陈平, 吴一波, 崔红霞, 张旭熙, 孙昕霙. 基于大五人格特质的2型糖尿病患者健康教育偏好[J]. 北京大学学报(医学版), 2026, 58(3): 600-605. |
| [6] | 赵豆豆, 齐晅, 黄博, 高伟波, 裴源源, 金月波, 邵苗, 何菁. 感染性肺炎与免疫相关间质性肺病中淋巴细胞亚群的表达[J]. 北京大学学报(医学版), 2026, 58(3): 624-630. |
| [7] | 白晓强, 袁芷若, 周永胜, 吕珑薇. 动态牵张促进人骨髓间充质干细胞三维培养的成骨分化[J]. 北京大学学报(医学版), 2026, 58(3): 641-649. |
| [8] | 季加孚, 韦静涛, 季科, 步召德. 胃癌诊疗的瓶颈与破局:迈向精准化与智能化融合的新纪元[J]. 北京大学学报(医学版), 2026, 58(2): 231-238. |
| [9] | 高加勒, 张忠涛. 局部进展期直肠癌精准治疗现状与展望[J]. 北京大学学报(医学版), 2026, 58(2): 247-250. |
| [10] | 杜文, 章文博, 于尧, 刘硕, 苏惠裕, 胡耒豪, 唐祖南, 吴彬彰, 陈震, 李家琦, 王昊, 彭歆. 口腔颌面部肿瘤"数智化外科"诊疗流程探索与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 278-284. |
| [11] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [12] | 李斌, 梁寒. 机器人胃癌根治术:研究进展与实践挑战[J]. 北京大学学报(医学版), 2026, 58(2): 416-422. |
| [13] | 黄宁, 刘笑晗, 郭静. 医疗保险对流动慢性病患者卫生服务利用的影响以及健康风险感知在其中的调节作用[J]. 北京大学学报(医学版), 2026, 58(1): 160-168. |
| [14] | 耿芸玲, 刘超, 杨萍, 郑佳佳, 沈宁, 杜毅鹏. 医院获得性肺炎患者肺炎克雷伯菌多部位感染的临床特征及毒力基因分布[J]. 北京大学学报(医学版), 2026, 58(1): 201-207. |
| [15] | 魏粤晖, 简伟研. 中国老年人社会经济地位与视力障碍的相关性[J]. 北京大学学报(医学版), 2025, 57(6): 1136-1144. |
|
||
