北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (1): 68-76. doi: 10.19723/j.issn.1671-167X.2022.01.011
口腔鳞状细胞癌患者修复重建术后感染的病原学特征及感染风险预测模型的构建
苏俊琪1,宋扬1,谢尚2,△( )
)
- 1.北京大学口腔医学院·口腔医院 检验科,北京 100081
2.北京大学口腔医学院·口腔医院 口腔颌面外科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔数字化医疗技术和材料国家工程实验室,口腔数字医学北京市重点实验室,国家卫生健康委员会口腔医学计算机应用工程技术研究中心,国家药品监督管理局口腔生物材料重点实验室,北京 100081
Analysis of etiological characteristics and establishment of prediction model of postoperative infections in patients undergoing oral squamous cell carcinoma surgery with free flap reconstruction
SU Jun-qi1,SONG Yang1,XIE Shang2,△()
- 1. Department of Clinical Laboratory, Peking University School and Hospital of Stomatology, Beijing 100081, China
2. Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
摘要:
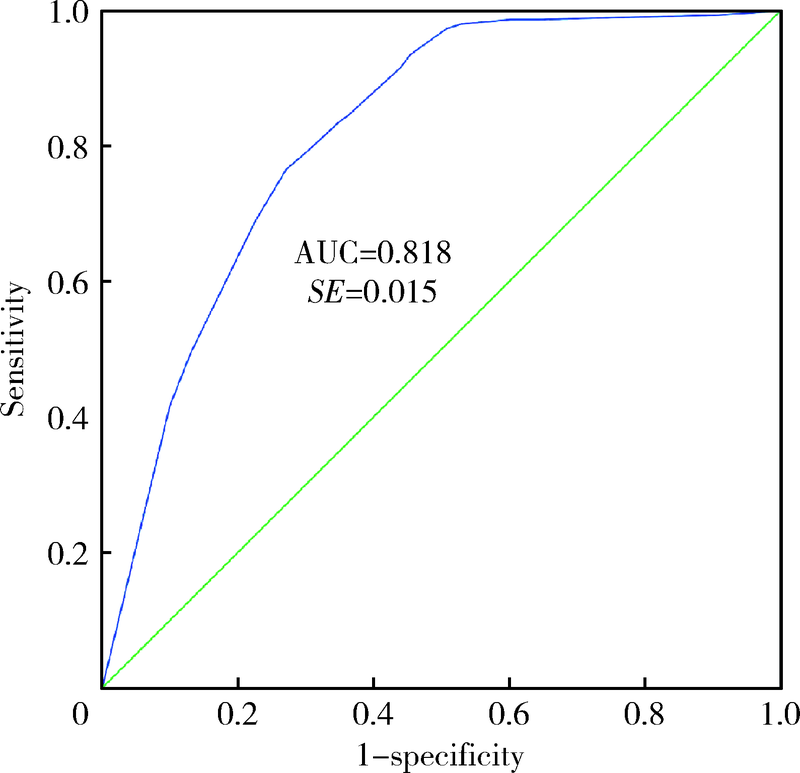
目的: 旨在发现行根治性肿瘤切除、颈淋巴结清扫并游离皮瓣修复重建术的原发性口腔鳞状细胞癌患者术后感染的病原学特征,并构建感染风险预测模型。方法: 选取2018年1月至2020年12月在北京大学口腔医院行根治性肿瘤切除并游离皮瓣修复重建术的口腔鳞状细胞癌患者1 596例为研究对象,按照患者术后感染发生情况分为感染组(n=154)和未感染组(n=1 442), 分析感染组患者的病原菌特征。以患者是否发生术后感染作为结果变量,采用单因素和多因素Logistic回归分析来确定术后感染的相关因素,并用于构建感染风险预测模型,采用受试者工作特征(receiver operating characteristic,ROC)曲线评估模型的预测效能。结果: 1 596例口腔鳞状细胞癌患者行修复重建术后发生感染154例,感染率为9.65%,感染部位以手术切口和呼吸道为主;共培养分离病原菌268株,其中革兰阴性菌240株,占89.55%,以铜绿假单胞菌(Pseudomonas aeruginosa)和肺炎克雷伯菌(Klebsiella pneumoniae)为主;革兰阳性菌23株,占8.58%,以粪肠球菌(Enterococcus faecalis)和金黄色葡萄球菌(Staphylococcus aureus)为主;真菌5株,占1.87%。分离出的铜绿假单胞菌对亚胺培南和美罗培南的耐药率较高,对环丙沙星等比较敏感;分离出的金黄色葡萄球菌对红霉素和克林霉素耐药率较高,对万古霉素敏感。N分期≥1、美国麻醉医师协会(American Society of Anesthesiologists,ASA)分级≥Ⅱ级、气管切开、住院天数>13 d是患者术后感染的独立危险因素(P<0.05), 据此构建感染风险预测模型的表达式为:预测概率值P=1/(1+e-a),a=-0.803+0.674×(N分期≥1)+0.518×(ASA分级≥Ⅱ级)+0.918×(气管切开)+1.581×(住院天数>13 d),Hosmer-Lemeshow χ2=10.647,P=0.223,提示模型的拟合度较好。模型预测患者术后感染的ROC曲线下面积为0.818,95%CI为0.789~0.846。结论: 口腔鳞状细胞癌修复重建术后感染发生率较高,主要致病菌为革兰阴性菌。多因素Logistic回归分析构建的感染预测模型可以有效预测口腔鳞状细胞癌修复重建术后感染的发生,使临床能够有针对性地采取监测和干预措施,合理使用抗菌药物,有利于预防和减少术后感染。
中图分类号:
- R782.3
| [1] |
Panarese I, Aquino G, Ronchi A, et al. Oral and oropharyngeal squamous cell carcinoma: Prognostic and predictive parameters in the etiopathogenetic route[J]. Expert Rev Anticancer ther, 2019, 19(2):105-119.
doi: 10.1080/14737140.2019.1561288 |
| [2] |
Cannon RB, Houlton JJ, Mendez E, et al. Methods to reduce postoperative surgical site infections after head and neck oncology surgery[J]. Lancet Oncol, 2017, 18(7):e405-e413.
doi: 10.1016/S1470-2045(17)30375-3 |
| [3] |
McBain AJ, Sissons C, Ledder RG, et al. Development and cha-racterization of a simple perfused oral microcosm[J]. J Appl Microbiol, 2005, 98(3):624-634.
pmid: 15715865 |
| [4] | Jansisyanont P, Kasemsai W, Bamroong P. Factors related to the treatment outcome of maxillofacial fascia space infection[J]. J Oral Max Surg Med Pathol, 2015, 27(4):458-464. |
| [5] | 张建丽, 刘玉坤, 任起辉, 等. 行口腔颌面外科术患者术后感染病原学特征及相关因素分析[J]. 中华医院感染学杂志, 2018, 28(3):440-443. |
| [6] | 李月莉, 苏翠霞, 高凤蕊, 等. 口腔颌面外科患者气管切开术后肺部感染的病原学分析及干预对策[J]. 中华医院感染学杂志, 2014, 24(5):1239-1241. |
| [7] |
Manchon A, Prados-Frutos JC, Rueda-Rodriguez C, et al. Anti-biotic release from calcium phosphate materials in oral and maxillofacial surgery: Molecular, cellular and pharmaceutical aspects[J]. Curr Pharm Biotechnol, 2017, 18(1):52-63.
doi: 10.2174/1389201018666161114145827 |
| [8] | 刘登峰, 孙仁义, 肖进, 等. 口腔颌面外科患者医院感染病原菌分布及耐药性分析[J]. 中华医院感染学杂志, 2014, 24(23):5928-5930. |
| [9] | 李新芳, 顾华芳, 顾永华, 等. 肠杆菌科细菌耐药性与抗菌药物使用强度的相关性分析[J]. 中华医院感染学杂志, 2016, 26(1):16-18. |
| [10] |
Batard E, Ollivier F, Boutoille D, et al. Relationship between hospital antibiotic use and quinolone resistance in Escherichia coli[J]. Int J Infect Dis, 2013, 17(4):e254-e258.
doi: 10.1016/j.ijid.2012.10.005 |
| [11] | 解泽强, 菅记涌, 孙盼盼, 等. 2010—2015年医院铜绿假单胞菌感染分布及耐药性分析[J]. 中华医院感染学杂志, 2017, 27(3):498-500. |
| [12] | 张艳, 魏华波, 王志强, 等. 医院感染铜绿假单胞菌的分布及耐药性研究[J]. 中华医院感染学杂志, 2014, 24(13):3139-3141. |
| [13] | 侯飞, 王玲, 崔伟锋, 等. 铜绿假单胞菌医院感染的危险因素及耐药性分析[J]. 中华医院感染学杂志, 2013, 23(16):4050-4052. |
| [14] | Zhao Y, Guo L, Li J, et al. Molecular epidemiology, antimicro-bial susceptibility, and pulsed-field gel electrophoresis genotyping of Pseudomonas aeruginosa isolates from mink[J]. Can J Vet Res, 2018, 82(4):256-263. |
| [15] |
Shanthi J, Pazhanimurugan R, Gopikrishnan V, et al. Mechanism of drug resistance, characterization of plasmid-borne determinants and transformation study in P. aeruginosa from burn and ICU units-its susceptibility pattern[J]. Burns, 2013, 39(4):643-649.
doi: 10.1016/j.burns.2012.08.012 pmid: 22980776 |
| [16] | 郑百慧, 龚春梅, 黎敏, 等. 呼吸与危重症医学病房分离的碳青霉烯耐药铜绿假单胞菌的分子流行病学[J]. 中华医院感染学杂志, 2020, 30(17):2610-2614. |
| [17] |
Oliveira MC, Oliveira CR, Gonçalves KV, et al. Enterobacte-riaceae resistant to third generation cephalosporins upon hospital admission: Risk factors and clinical outcomes[J]. Braz J Infect Dis, 2015, 19(3):239-245.
doi: 10.1016/j.bjid.2015.01.006 |
| [18] |
Guo Z, Zhang J, Gong Z, et al. Correlation of factors associated with postoperative infection in patients with malignant oral and maxillofacial tumours: A Logistic regression analysis[J]. Br J Oral Maxillofac Surg, 2019, 57(5):460-465.
doi: S0266-4356(19)30123-8 pmid: 31006505 |
| [19] | Anehosur VS, Karadiguddi P, Joshi VK, et al. Elective tracheostomy in head and neck surgery: Our experience[J]. J Clin Diagn Res, 2017, 11(5): ZC36-ZC39. |
| [20] |
Goetz C, Burian NM, Weitz J, et al. Temporary tracheotomy in microvascular reconstruction in maxillofacial surgery: Benefit or threat?[J]. J Craniomaxillofac Surg, 2019, 47(4):642-646.
doi: 10.1016/j.jcms.2019.01.017 |
| [21] |
Li L, Yuan W, Zhang S, et al. Analysis of risk factors for pneumonia in 482 patients undergoing oral cancer surgery with tracheo-tomy[J]. J Oral Maxillofac Surg, 2016, 74(2):415-419.
doi: 10.1016/j.joms.2015.08.018 |
| [22] |
Xu J, Hu J, Yu P, et al. Perioperative risk factors for postoperative pneumonia after major oral cancer surgery: A retrospective analysis of 331 cases[J]. PLoS One, 2017, 12(11):e0188167.
doi: 10.1371/journal.pone.0188167 |
| [23] |
Algar FJ, Alvarez A, Salvatierra A, et al. Predicting pulmonary complications after pneumonectomy for lung cancer[J]. Eur J Cardiothorac Surg, 2003, 23(2):201-208.
doi: 10.1016/S1010-7940(02)00719-4 |
| [24] |
Maeng SH, Yoo HS, Choi SH, et al. Impact of parainfluenza virus infection in pediatric cancer patients[J]. Pediatr Blood Cancer, 2012, 59(4):708-710.
doi: 10.1002/pbc.23390 pmid: 22095941 |
| [25] |
Liu P, Li X, Luo M, et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection: A meta-analysis[J]. Microb Drug Resist, 2018, 24(2):190-198.
doi: 10.1089/mdr.2017.0061 |
| [26] |
Zhu WM, Yuan Z, Zhou HY. Risk factors for carbapenem-resis-tant Klebsiella pneumoniae infection relative to two types of control patients: A systematic review and meta-analysis[J]. Antimicrob Resist Infect Control, 2020, 9(1):23.
doi: 10.1186/s13756-020-0686-0 |
| [1] | 付浩, 申潞艳, 黄冰洋, 马少华. 免疫治疗背景下食管鳞状细胞癌围手术期治疗的临床思考[J]. 北京大学学报(医学版), 2026, 58(2): 266-271. |
| [2] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [3] | 温倩颖, 张丽卿, 秦安霖, 李小峰. 无症状高尿酸血症患者小肠细菌过度生长及炎症细胞因子表达水平[J]. 北京大学学报(医学版), 2026, 58(2): 313-318. |
| [4] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [5] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [6] | 耿芸玲, 刘超, 杨萍, 郑佳佳, 沈宁, 杜毅鹏. 医院获得性肺炎患者肺炎克雷伯菌多部位感染的临床特征及毒力基因分布[J]. 北京大学学报(医学版), 2026, 58(1): 201-207. |
| [7] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [8] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [9] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [10] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [11] | 杨子铭, 李淑雅, 李肖彤, 沈鹏, 孙烨祥, 林鸿波, 江志琴, 詹思延, 刘志科. 2015—2024年宁波市鄞州区肺炎人群呼吸道病原体分布特点[J]. 北京大学学报(医学版), 2025, 57(3): 496-506. |
| [12] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [13] | 朱慧, 闵赛南, 苏家增, 陈艳, 彭歆, 于尧, 俞光岩. 口腔黏膜嗜酸性溃疡的临床病理分析[J]. 北京大学学报(医学版), 2025, 57(3): 620-625. |
| [14] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [15] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
|
||
