北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (5): 915-922. doi: 10.19723/j.issn.1671-167X.2023.05.021
急性痛风发作的昼夜差异: 一项男性痛风患者的临床研究
董泓1,2,王丽敏1,王志强1,刘彦卿1,张晓刚1,张明明1,刘娟1,李振彬1,*( )
)
- 1. 中国人民解放军联勤保障部队第九八〇医院风湿免疫科, 石家庄 050082
2. 河北医科大学研究生院, 石家庄 050011
Diurnal differences in acute gout attacks: A clinical study of male gout patients
Hong DONG1,2,Li-min WANG1,Zhi-qiang WANG1,Yan-qing LIU1,Xiao-gang ZHANG1,Ming-ming ZHANG1,Juan LIU1,Zhen-bin LI1,*()
- 1. Department of Rheumatology and Immunology, PLA Joint Logistic Support Force No.980 Hospital, Shijiazhuang 050082, China
2. The Graduate School, Hebei Medical University, Shijiazhuang 050011, China
摘要:
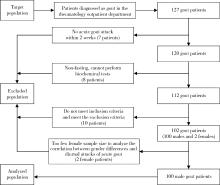
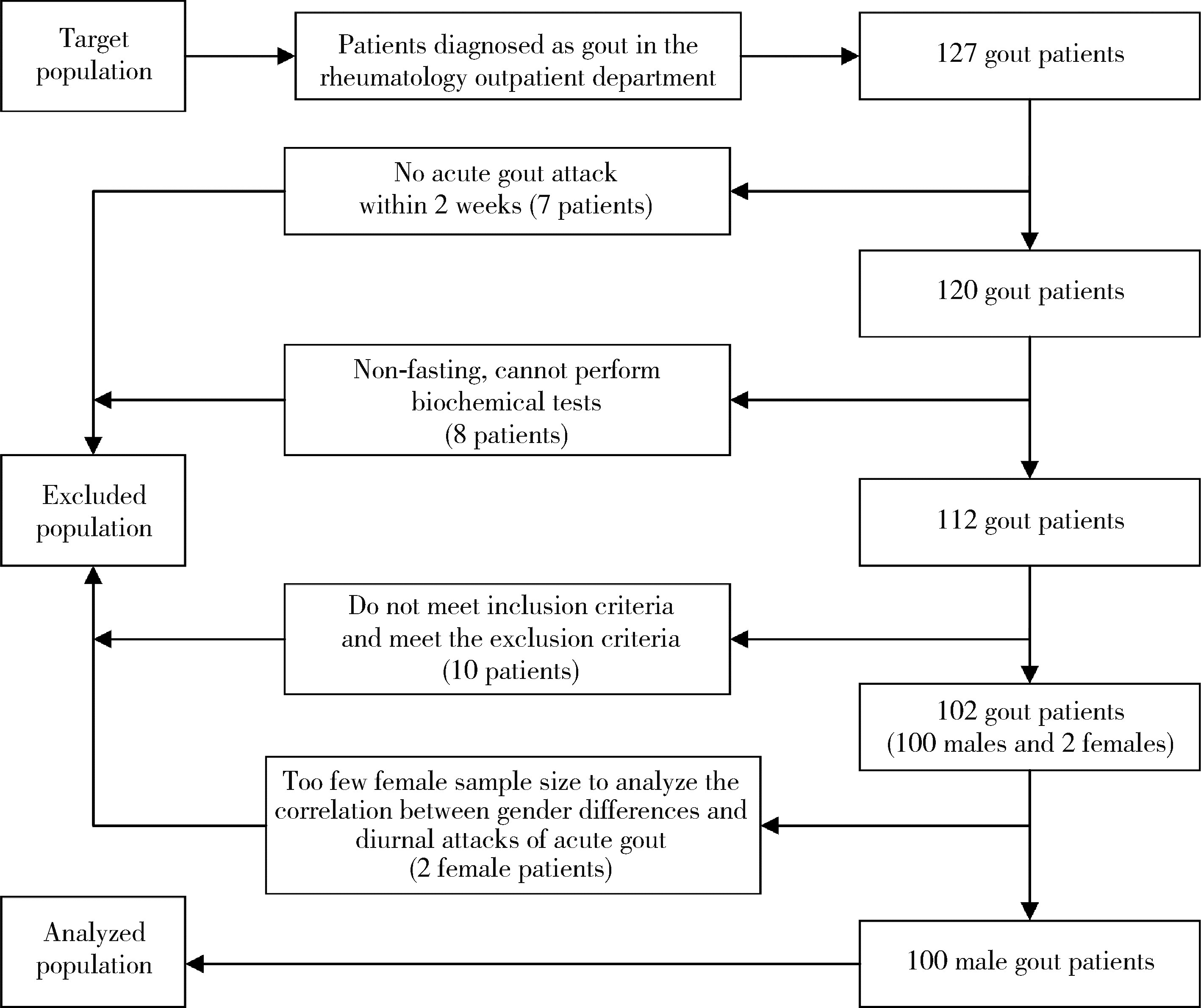
目的: 观察男性急性痛风发作的昼夜差异, 为临床精准防治提供参考。方法: 采用单中心、横断面研究设计, 选取2021年10月至2022年4月在中国人民解放军联勤保障部队第九八〇医院风湿免疫科门诊确诊为痛风的患者, 记录其本次或最近1次急性痛风发作的信息, 包括发作日期和时间、关节症状和体征、药物使用, 以及就诊当日相关生化检测等指标。分析男性痛风患者急性发作的昼夜时间差异, 进一步对急性痛风发作的昼夜差异与临床特点、生化指标等进行单因素比较及多因素Logistic回归分析。结果: 共纳入100例男性痛风患者, 记录100次急性发作。急性痛风发作人数的昼夜时间分布为: 上午(6:00~11:59, 18, 18%), 下午(12:00~17:59, 11, 11%), 前半夜(18:00~23:59, 22, 22%), 后半夜(0:00~05:59, 49, 49%); 白天(包括上午和下午, 29, 29%), 夜间(包括前半夜和后半夜, 71, 71%)。急性痛风夜间发作的比率明显高于白天, 夜间: 白天约为2.5 : 1。痛风无论是初发还是复发, 也无论病程长短, 其急性发作均存在昼少夜多的昼夜差异。夜间发作者与白天发作者相比, 血尿酸(serum urate, SU)水平更高(P=0.044);是否合并共病在急性痛风发作例次的昼夜构成比差异也具有统计学意义(P=0.028)。经多元Logistic回归分析, SU水平(OR=1.005, 95%CI: 1.001~1.009)、合并共病(OR=3.812, 95%CI: 1.443~10.144)是急性痛风夜间发作的相关因素。结论: 痛风无论初发和复发, 也无论病程长短, 其急性发作均具有以夜间多发为特点的昼夜差异; SU水平增高、存在共病是痛风患者夜间急性发作的相关因素。
中图分类号:
- R593.2
| 1 | Singh JA , Gaffo A . Gout epidemiology and comorbidities[J]. Semin Arthritis Rheum, 2020, 50 (Suppl 3): 11- 16. |
| 2 |
Choi HK , Mount DB , Reginato AM . Pathogenesis of gout[J]. Ann Intern Med, 2005, 143 (7): 499- 516.
doi: 10.7326/0003-4819-143-7-200510040-00009 |
| 3 |
Li Q , Li X , Wang J , et al. Diagnosis and treatment for hyperuricemia and gout: A systematic review of clinical practice guidelines and consensus statements[J]. BMJ Open, 2019, 9 (8): e026677.
doi: 10.1136/bmjopen-2018-026677 |
| 4 |
Allada R , Bass J . Circadian mechanisms in medicine[J]. N Engl J Med, 2021, 384 (6): 550- 561.
doi: 10.1056/NEJMra1802337 |
| 5 |
Ursini F , Giorgi AD , D'Onghia M , et al. Chronobiology and chronotherapy in inflammatory joint diseases[J]. Pharmaceutics, 2021, 13 (11): 1832- 1834.
doi: 10.3390/pharmaceutics13111832 |
| 6 | Early JO , Menon D , Wyse CA , et al. Circadian clock protein BMAL1 regulates IL-1β in macrophages via NRF2[J]. Proc Natl Acad Sci USA, 2018, 115 (36): E8460- E8468. |
| 7 |
Scheiermann C , Gibbs J , Ince L , et al. Clocking in to immunity[J]. Nat Rev Immunol, 2018, 18 (7): 423- 437.
doi: 10.1038/s41577-018-0008-4 |
| 8 |
Choi HK , Niu J , Neogi T , et al. Nocturnal risk of gout attacks[J]. Arthritis Rheumatol, 2015, 67 (2): 555- 562.
doi: 10.1002/art.38917 |
| 9 |
Gaffo AL , Dalbeth N , Saag KG , et al. Brief report: Validation of a definition of flare in patients with established gout[J]. Arthritis Rheumatol, 2018, 70 (3): 462- 467.
doi: 10.1002/art.40381 |
| 10 |
García D , Armengol NS , Crespo EL , et al. Blood uric acid levels in patients with sleep-disordered breathing[J]. Arch Bronconeumol, 2006, 42 (10): 492- 500.
doi: 10.1157/13093391 |
| 11 | Pływaczewski R , Bednarek M , Jonczak L , et al. Hyperuricaemia in males with obstructive sleep apnoea (OSA)[J]. Pneumonol Alergol Pol, 2005, 73 (3): 254- 259. |
| 12 | Chou YT , Chuang LP , Li HY , et al. Hyperlipidaemia in patients with sleep-related breathing disorders: prevalence & risk factors[J]. Indian J Med Res, 2010, 131, 121- 125. |
| 13 | Abrams B . High prevalence of gout with sleep apnea[J]. Med Hypotheses, 2012, 78 (2): 349- 351. |
| 14 |
Roddy E , Muller S , Hayward R , et al. The association of gout with sleep disorders: A cross-sectional study in primary care[J]. BMC Musculoskelet Disord, 2013, 14 (1): 119- 124.
doi: 10.1186/1471-2474-14-119 |
| 15 |
Dalbeth N , Gosling AL , Gaffo A , et al. Gout[J]. Lancet, 2021, 397 (10287): 1843- 1855.
doi: 10.1016/S0140-6736(21)00569-9 |
| 16 |
Kanabrocki , Eugene L . Circadian relationship of serum uric acid and nitric oxide[J]. JAMA, 2000, 283 (17): 2240- 2241.
doi: 10.1001/jama.283.17.2235 |
| 17 |
Kanabrocki EL , Murray D , Hermida RC , et al. Circadian variation in oxidative stress markers in healthy and type Ⅱ diabetic men[J]. Chronobiol Int, 2002, 19 (2): 423- 439.
doi: 10.1081/CBI-120002914 |
| 18 | Kanabrocki EL , Ryan M , Hermida RC , et al. Altered circadian relationship between serum nitric oxide, carbon dioxide, and uric acid in multiple Sclerosis[J]. Chronobiol Int, 2004, 21 (4/5): 739- 758. |
| 19 |
Devgun MS , Dhillon HS . Importance of diurnal variations on clinical value and interpretation of serum urate measurements[J]. J Clin Pathol, 1992, 45 (2): 110- 113.
doi: 10.1136/jcp.45.2.110 |
| 20 |
Selmaoui B , Lambrozo J , Touitou Y . Assessment of the effects of nocturnal exposure to 50 Hz magnetic fields on the human circadian system. A comprehensive study of biochemical variables[J]. Chronobiol Int, 1999, 16 (6): 789- 810.
doi: 10.3109/07420529909016946 |
| 21 |
Morrison B , Shenkin A , Mclelland A , et al. Intra-individual variation in commonly analyzed serum constituents[J]. Clin Chem, 1979, 25 (10): 1799- 1805.
doi: 10.1093/clinchem/25.10.1799 |
| 22 |
Statland BE , Winkel P , Bokelund H . Factors contributing to intra-individual variation of serum constituents. 1. Within-day variation of serum constituents in healthy subjects[J]. Clin Chem, 1973, 19 (12): 1374- 1379.
doi: 10.1093/clinchem/19.12.1374 |
| 23 |
Chagoya de Sánchez V , Hernández-Muñoz R , Suárez J , et al. Temporal variations of adenosine metabolism in human blood[J]. Chronobiol Int, 1996, 13 (3): 163- 177.
doi: 10.3109/07420529609012650 |
| 24 | Singh RK , Bansal A . Studies on circadian periodicity of serum and urinary urate in healthy Indians and renal stone formers[J]. Prog Clin Biol Res, 1987, 227, 305- 313. |
| 25 |
Cameron M , Maalouf NM , Poindexter J , et al. The diurnal variation in urine acidification differs between normal individuals and uric acid stone formers[J]. Kidney Int, 2012, 81 (11): 1123- 1130.
doi: 10.1038/ki.2011.480 |
| 26 |
司可, 王颜刚. 尿酸排泄昼夜节律与尿酸结石[J]. 中华风湿病学杂志, 2021, 25 (10): 711- 714.
doi: 10.3760/cma.j.cn141217-20201222-00490 |
| 27 |
Harrison D , Bock MG , Doedens JR , et al. Discovery and optimization of triazolopyrimidinone derivatives as selective NLRP3 inflammasome inhibitors[J]. ACS Med Chem Lett, 2022, 13 (8): 1321- 1328.
doi: 10.1021/acsmedchemlett.2c00242 |
| 28 |
Pourcet B , Zecchin M , Ferri L , et al. Nuclear receptor subfamily 1 group D member 1 regulates circadian activity of NLRP3 inflammasome to reduce the severity of fulminant hepatitis in mice[J]. Gastroenterology, 2018, 154 (5): 1449- 1464.
doi: 10.1053/j.gastro.2017.12.019 |
| 29 |
Pourcet B , Duez H . Circadian control of inflammasome pathways: Implications for circadian medicine[J]. Front Immunol, 2020, 11, 1630- 1642.
doi: 10.3389/fimmu.2020.01630 |
| 30 | Avouac J , Gossec L , Dougados M . Diagnostic and predictive value of anti-cyclic citrullinated protein antibodies in rheumatoid arthritis: A systematic literature review[J]. Ann Rheum Dis, 2006, 65 (7): 845- 851. |
| 31 | 李振彬, 王自强. 中医时间用药法探讨[J]. 山东中医学院学报, 1988, 12 (2): 14-16, 73. |
| 32 |
Smolensky MH , Portaluppi F , Manfredini R , et al. Diurnal and twenty-four hour patterning of human diseases: Cardiac, vascular, and respiratory diseases, conditions, and syndromes[J]. Sleep Med Rev, 2015, 21, 3- 11.
doi: 10.1016/j.smrv.2014.07.001 |
| 33 |
Riha RL . The use and misuse of exogenous melatonin in the treatment of sleep disorders[J]. Curr Opin Pulm Med, 2018, 24 (6): 543- 548.
doi: 10.1097/MCP.0000000000000522 |
| [1] | 甘地, 付强, 唐小惠, 李楚炜, 舒兆平. 胸锁关节痛风1例[J]. 北京大学学报(医学版), 2026, 58(3): 670-673. |
| [2] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [3] | 叶一林,刘恒,潘利平,柴卫兵. 全膝关节置换术后假体周围痛风发作误诊1例[J]. 北京大学学报(医学版), 2023, 55(2): 362-365. |
| [4] | 王昱,张慧敏,邓雪蓉,刘伟伟,陈璐,赵宁,张晓慧,宋志博,耿研,季兰岚,王玉,张卓莉. 尿枸橼酸定量检测在原发性痛风患者肾结石诊断中的应用价值[J]. 北京大学学报(医学版), 2022, 54(6): 1134-1140. |
| [5] | 谢晓炜,李芬,凌光辉,谢希,许素清,陈谊月. 痛风患者健康教育知识知晓度测量问卷的研制及临床应用[J]. 北京大学学报(医学版), 2022, 54(4): 699-704. |
| [6] | 彭喆,丁亚敏,裴林,姚海红,张学武,唐素玫. 痛风患者发生关节及肌腱内晶体沉积的临床特点[J]. 北京大学学报(医学版), 2021, 53(6): 1067-1071. |
| [7] | 张学武. 痛风关节炎治疗中几个备受关注的问题[J]. 北京大学学报(医学版), 2021, 53(6): 1017-1019. |
| [8] | 王贵红,左婷,李然,左正才. 瑞巴派特在大鼠痛风性关节炎急性发作中的作用[J]. 北京大学学报(医学版), 2021, 53(4): 716-720. |
| [9] | 谢一帆,王昱,邓雪蓉,耿研,季兰岚,张卓莉. 影响双能CT尿酸盐结晶检出率的因素[J]. 北京大学学报(医学版), 2021, 53(2): 261-265. |
| [10] | 王昱,邓雪蓉,季兰岚,张晓慧,耿研,张卓莉. 超声检测痛风患者肌腱受累的危险因素和诊断价值[J]. 北京大学学报(医学版), 2021, 53(1): 143-149. |
| [11] | 季兰岚,郝燕捷,张卓莉. 原发性骨髓纤维化引起的继发性痛风1例[J]. 北京大学学报(医学版), 2018, 50(6): 1117-1119. |
| [12] | 张倩茹,王昱,张卓莉. 2015 ACR/EULAR痛风分类标准与既往标准诊断价值的比较研究[J]. 北京大学学报(医学版), 2017, 49(6): 979-984. |
| [13] | 赵卫, 高辉, 朱佳鑫, 张学武, 栗占国. 血清Dickkopf-1与原发性痛风性关节炎骨破坏的相关性[J]. 北京大学学报(医学版), 2012, 44(2): 254-258. |
| [14] | 武丽君, 宋小芸, 库尔班江, 石亚妹, 黄慈波, 黄嘉, 刘爱华, 米克拉依, 滕玉芬, 古丽娜, 孟新艳, 单新洁, 木亚赛, 苑爱萍, 张莉. 新疆吐鲁番地区维吾尔族人群高尿酸血症和痛风的流行病学调查[J]. 北京大学学报(医学版), 2012, 44(2): 250-253. |
| [15] | 刘湘源, 郑晓娟. 尿酸持续达标是难治性痛风治疗的关键[J]. 北京大学学报(医学版), 2012, 44(2): 168-170. |
|
||
