北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (6): 1089-1096. doi: 10.19723/j.issn.1671-167X.2024.06.023
2型糖尿病对口腔鳞状细胞癌患者预后的影响
毛雅晴1, 陈震1, 于尧1, 章文博1, 刘洋2,*( ), 彭歆1,*()
), 彭歆1,*()
- 1. 北京大学口腔医学院·口腔医院口腔颌面外科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔生物材料和数字诊疗装备国家工程研究中心,口腔数字医学北京市重点实验室,北京 100081
2. 北京大学口腔医学院·口腔医院口腔黏膜科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔生物材料和数字诊疗装备国家工程研究中心,口腔数字医学北京市重点实验室,北京 100081
Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma
Yaqing MAO1, Zhen CHEN1, Yao YU1, Wenbo ZHANG1, Yang LIU2,*(), Xin PENG1,*()
- 1. Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
2. Department of Oral Medicine, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
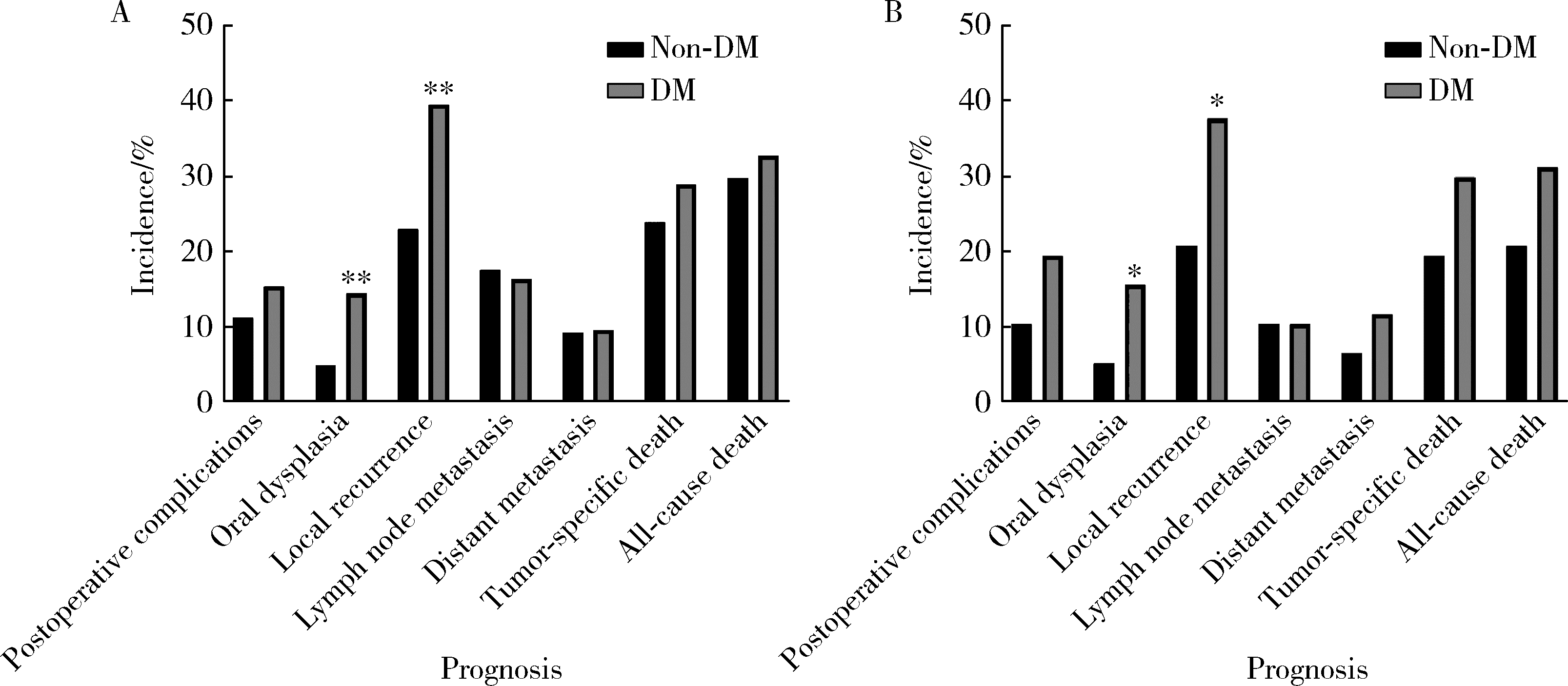
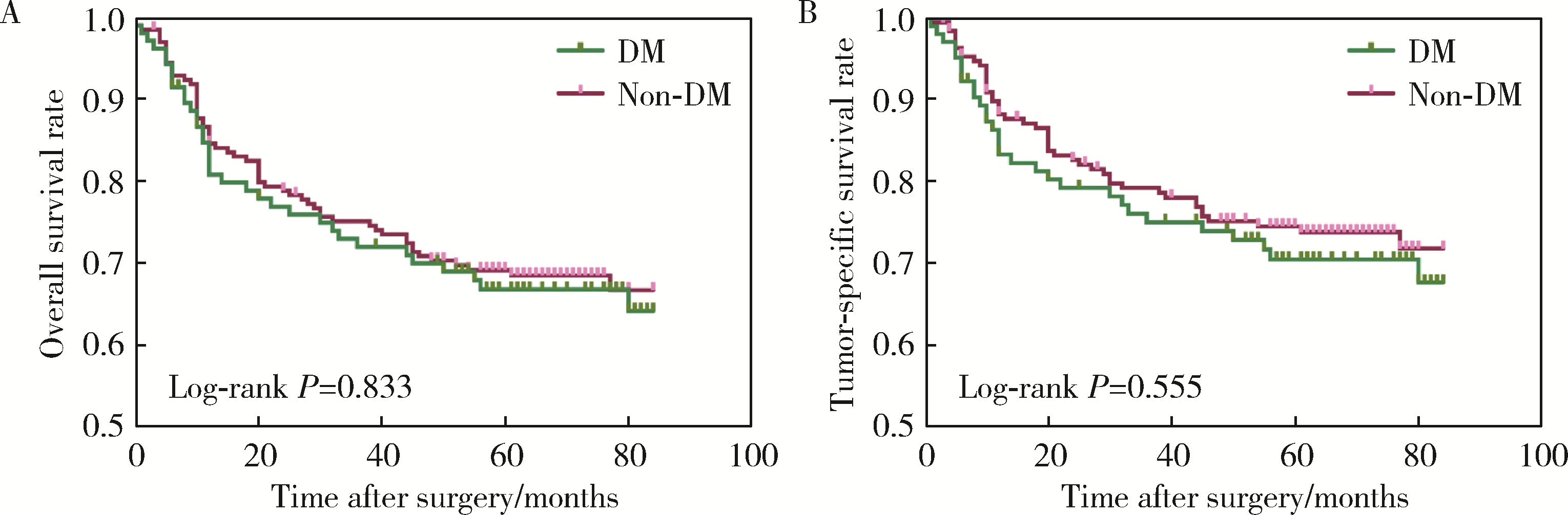
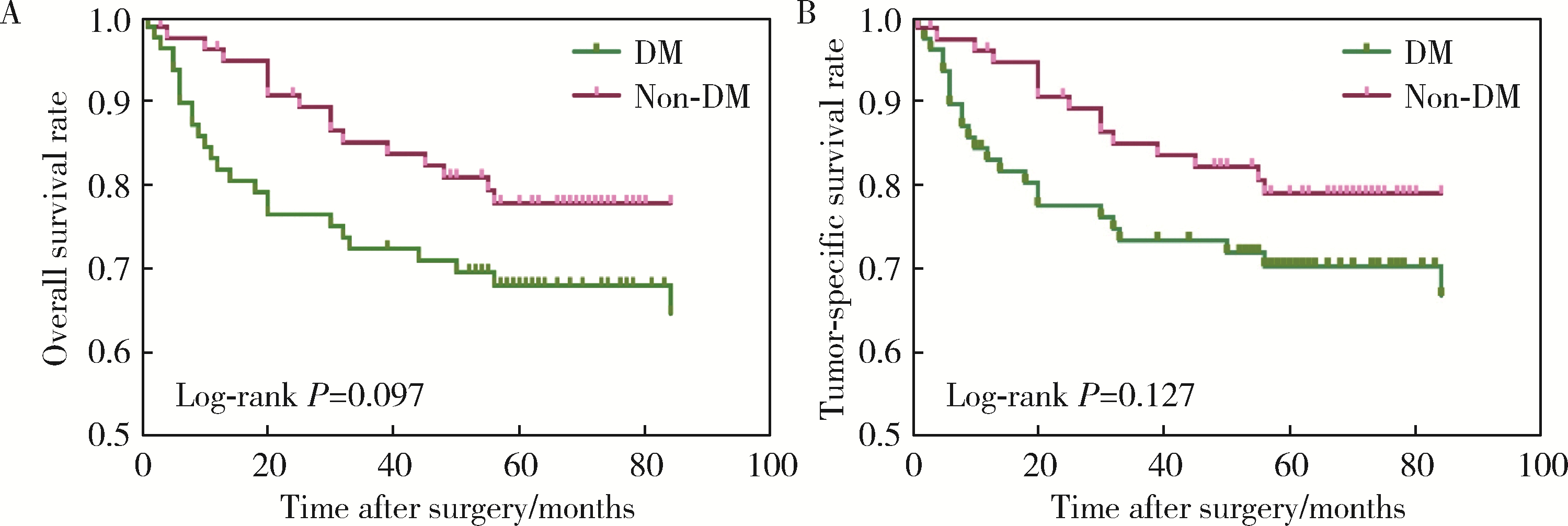
目的: 分析合并2型糖尿病(diabetes mellitus, DM)对罹患口腔鳞状细胞癌(oral squamous cell carcinoma, OSCC)的患者预后的影响。方法: 回顾性分析2014年1月至2017年12月间北京大学口腔医院口腔颌面外科收治的309例OSCC患者的临床病理资料,其中DM组104例,无DM组205例,对患者的基本临床资料和预后情况进行总结分析,利用倾向评分匹配(propensity score matching, PSM)方法均衡两组的组间协变量,采用Kaplan-Meier方法计算两组患者的生存率,采用Cox回归分析影响预后的风险因素,并分析DM组血糖控制情况对生存结果的影响。结果: 经过PSM,两组共有77对匹配成功,组间协变量达到均衡。两组患者术后出现黏膜癌前病变以及局部复发的比例差异有统计学意义(P < 0.05)。两组患者的生存分析结果差异无统计学意义,但经过匹配后,DM组的生存率有低于无DM组的趋势。单因素及多因素分析显示,肿瘤分期是OSCC患者总生存率及肿瘤特异性生存率的独立影响因素(P < 0.05),而有无DM对OSCC患者的生存影响差异无统计学意义(P>0.05)。针对DM组的多因素分析发现,肿瘤分期、甘油三酯水平、术前平均末梢血糖(空腹)、术后平均末梢血糖(餐后2 h)是DM组患者术后总生存情况的独立危险因素;肿瘤分期和术后平均末梢血糖(餐后2 h)是DM组患者术后肿瘤特异性生存率的独立危险因素。DM组内的血糖控制欠佳组出现术后并发症及远处转移的风险有高于血糖控制良好组的趋势。结论: 有无DM对患者的总生存率及肿瘤特异性生存率的影响差异无统计学意义,但DM组术后出现黏膜癌前病变或局部肿瘤复发的可能性高于无DM组;糖尿病患者的肿瘤分期、甘油三酯水平、血糖控制情况可能影响其预后。
中图分类号:
- R739.8

| 1 |
Campbell PT , Newton CC , Patel AV , et al.Diabetes and cause-specific mortality in a prospective cohort of one million U.S. adults[J].Diabetes Care,2012,35(9):1835-1844.
doi: 10.2337/dc12-0002 |
| 2 | 赵佳, 韩雪, 谢梦, 等.2型糖尿病并发恶性肿瘤患者的流行病学分析[J].中国慢性病预防与控制,2018,26(7):514-516. |
| 3 |
Tsilidis KK , Kasimis JC , Lopez DS , et al.Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies[J].BMJ,2015,350,g7607.
doi: 10.1136/bmj.g7607 |
| 4 | Vairaktaris E , Spyridonidou S , Goutzanis L , et al.Diabetes and oral oncogenesis[J].Anticancer Res,2007,27(6B):4185-4193. |
| 5 |
Wu CH , Wu TY , Li CC , et al.Impact of diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma: A retrospective cohort study[J].Ann Surg Oncol,2010,17(8):2175-2183.
doi: 10.1245/s10434-010-0996-1 |
| 6 |
Stott-Miller M , Chen C , Schwartz SM .Type Ⅱ diabetes and metabolic syndrome in relation to head and neck squamous cell carcinoma risk: A SEER-Medicare database study[J].Cancer Epidemiol,2013,37(4):428-433.
doi: 10.1016/j.canep.2013.03.006 |
| 7 |
Tseng CH .Oral cancer in Taiwan: Is diabetes a risk factor?[J].Clin Oral Investig,2013,17(5):1357-1364.
doi: 10.1007/s00784-012-0820-3 |
| 8 |
中华医学会糖尿病学分会.中国2型糖尿病防治指南(2020年版)[J].中华内分泌代谢杂志,2021,37(4):311-398.
doi: 10.3760/cma.j.cn311282-20210304-00142 |
| 9 |
Pfister DG , Spencer S , Adelstein D , et al.Head and neck cancers, version 2.2020, NCCN clinical practice guidelines in oncology[J].J Natl Compr Canc Netw,2020,18(7):873-898.
doi: 10.6004/jnccn.2020.0031 |
| 10 | Amin MB , Edge SB , Greene FL , et al.AJCC cancer staging manual[M].8th ed. New York: Springer,2017. |
| 11 |
高柳, 毛驰, 俞光岩, 等.成人并存疾病评价指数27条目中文简体版引进的授权、翻译回译和语义调适[J].中华口腔医学杂志,2016,51(10):623-627.
doi: 10.3760/cma.j.issn.1002-0098.2016.10.010 |
| 12 |
Austin PC .An introduction to propensity score methods for reducing the effects of confounding in observational studies[J].Multivariate Behav Res,2011,46(3):399-424.
doi: 10.1080/00273171.2011.568786 |
| 13 | Ling S , Brown K , Miksza JK , et al.Risk of cancer incidence and mortality associated with diabetes: A systematic review with trend analysis of 203 cohorts[J].Nutr Metab Cardiovasc Dis,2020,31(1):14-22. |
| 14 |
Pearson-Stuttard J , Bennett J , Cheng YJ , et al.Trends in predominant causes of death in individuals with and without diabetes in England from 2001 to 2018: An epidemiological analysis of linked primary care records[J].Lancet Diabetes Endocrinol,2021,9(3):165-173.
doi: 10.1016/S2213-8587(20)30431-9 |
| 15 | 周维, 何明艳, 沈婉莹, 等.2005—2015年中国口腔癌发病及死亡趋势分析[J].华中科技大学学报(医学版),2020,49(6):58-63. |
| 16 | Végh D , Bányai D , Ujpál M .Change in the incidence of diabetes mellitus in oral cancer patients based on a long-term comparative study[J].Fogorv Sz,2015,108(1):9-12. |
| 17 |
Yan P , Wang Y , Yu X , et al.Type 2 diabetes mellitus and risk of head and neck cancer subtypes: A systematic review and meta-analysis of observational studies[J].Acta Diabetol,2021,58(5):549-565.
doi: 10.1007/s00592-020-01643-0 |
| 18 | 王新革. 舌鳞癌与肿瘤侵袭模式、2型糖尿病的相关性研究[D]. 西安: 第四军医大学, 2017: 42. |
| 19 |
Supabphol S , Seubwai W , Wongkham S , et al.High glucose: An emerging association between diabetes mellitus and cancer progression[J].J Mol Med (Berl),2021,99(9):1175-1193.
doi: 10.1007/s00109-021-02096-w |
| 20 |
Cignarelli A , Annamaria Genchi V , Caruso I , et al.Diabetes and cancer: Pathophysiological fundamentals of a "dangerous affair"[J].Diabetes Res Clin Pract,2018,143,378-388.
doi: 10.1016/j.diabres.2018.04.002 |
| 21 | Liu CJ , Chang WJ , Chen CY , et al.Dynamic cellular and mole-cular modulations of diabetes mediated head and neck carcinogenesis[J].Oncotarget,2015,30(6):29268-29284. |
| 22 | 张东升, 郑家伟, 张陈平, 等.口腔癌合并全身系统性疾病患者的多学科协作诊疗模式专家共识[J].华西口腔医学杂志,2020,38(6):603-615. |
| 23 | 李金, 华红. 口腔癌中国流行病学趋势及口腔白斑癌变危险因素分析[D]. 北京: 北京大学, 2019. |
| 24 |
Villa A , Woo SB .Leukoplakia: A diagnostic and management algorithm[J].J Oral Maxillofac Surg,2017,75(4):723-734.
doi: 10.1016/j.joms.2016.10.012 |
| 25 |
Li G , Da M , Zhang W , et al.Alteration of serum lipid profile and its prognostic value in head and neck squamous cell carcinoma[J].J Oral Pathol Med,2016,45(3):167-172.
doi: 10.1111/jop.12344 |
| 26 |
Shalapour S , Karin M .Immunity, inflammation, and cancer: An eternal fight between good and evil[J].J Clin Invest,2015,125(9):3347-3355.
doi: 10.1172/JCI80007 |
| 27 | Lu A , Li H , Zheng Y , et al.Prognostic significance of neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio, and platelet to lymphocyte ratio in patients with nasopharyngeal carcinoma[J].Biomed Res Int,2017,2017,3047802. |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 袁思妍, 闵鹤葳, 陈平, 吴一波, 崔红霞, 张旭熙, 孙昕霙. 基于大五人格特质的2型糖尿病患者健康教育偏好[J]. 北京大学学报(医学版), 2026, 58(3): 600-605. |
| [3] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [4] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 闵鹤葳, 吴一波, 史宇晖, 李明子, 孙昕霙. 基于健康行动过程取向模型分析2型糖尿病患者膳食模式及血糖控制的影响因素[J]. 北京大学学报(医学版), 2025, 57(6): 1145-1152. |
| [7] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [8] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [9] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [10] | 陈子砚, 张晓悦, 顾亦梧, 常春. 2型糖尿病患者使用E-health管理疾病意愿与影响机制[J]. 北京大学学报(医学版), 2025, 57(3): 522-528. |
| [11] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [12] | 徐励, 史闻, 李月华, 沈亚俊, 谢尚, 单小峰, 蔡志刚. 含LIM调宁蛋白同源域蛋白1可能作为辅助口腔鳞状细胞癌预后判断的生物学标志物[J]. 北京大学学报(医学版), 2025, 57(1): 19-25. |
| [13] | 马民英, 晁晓芹, 赵扬, 赵国廷. LncRNA SNHG20靶向调控miR-520c-3p/RAB22A通路对人口腔鳞状细胞癌细胞上皮间质转化及微管形成的影响[J]. 北京大学学报(医学版), 2025, 57(1): 26-32. |
| [14] | 张培恒, 高莹, 吴红花, 张健, 张俊清. 暴发性1型糖尿病合并急性胰腺炎1例及文献回顾[J]. 北京大学学报(医学版), 2024, 56(5): 923-927. |
| [15] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
|
||
