北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (4): 740-747. doi: 10.19723/j.issn.1671-167X.2025.04.018
较大的肱骨大结节角和峰盂角与肩袖撕裂的相关性
蒋华1, 颜宇2, 李盼盼1, 陈康1, 马红兵1, 曾勇1, 唐新2, 崔国庆3,*( )
)
- 1. 成都市第二人民医院/成都医学院附属医院骨科, 成都 610017
2. 四川大学华西医院骨科, 成都 610041
3. 北京大学第三医院运动医学科, 北京 100191
Association of increased greater tubercle angle and critical shoulder angle with rotator cuff tears
Hua JIANG1, Yu YAN2, Panpan LI1, Kang CHEN1, Hongbing MA1, Yong ZENG1, Xin TANG2, Guoqing CUI3,*()
- 1. Department of Orthopedics, Chengdu Second People ' s Hospital, Affiliated Hospital of Chengdu Medical College, Chengdu 610017, China
2. Department of Orthopedics, West China Hospital, Sichuan University, Chengdu 610041, China
3. Department of Sports Medicine, Peking University Third Hospital, Beijing 100191, China
摘要:
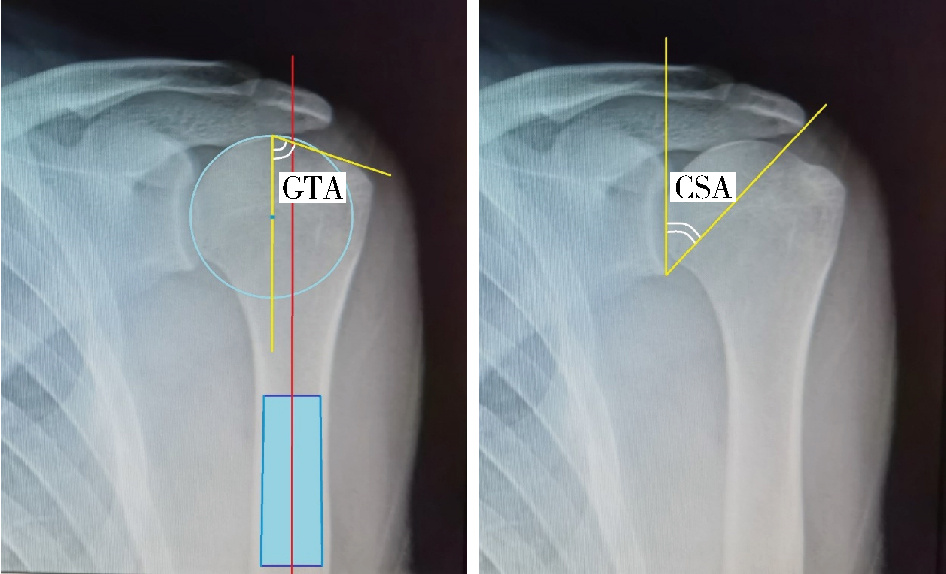
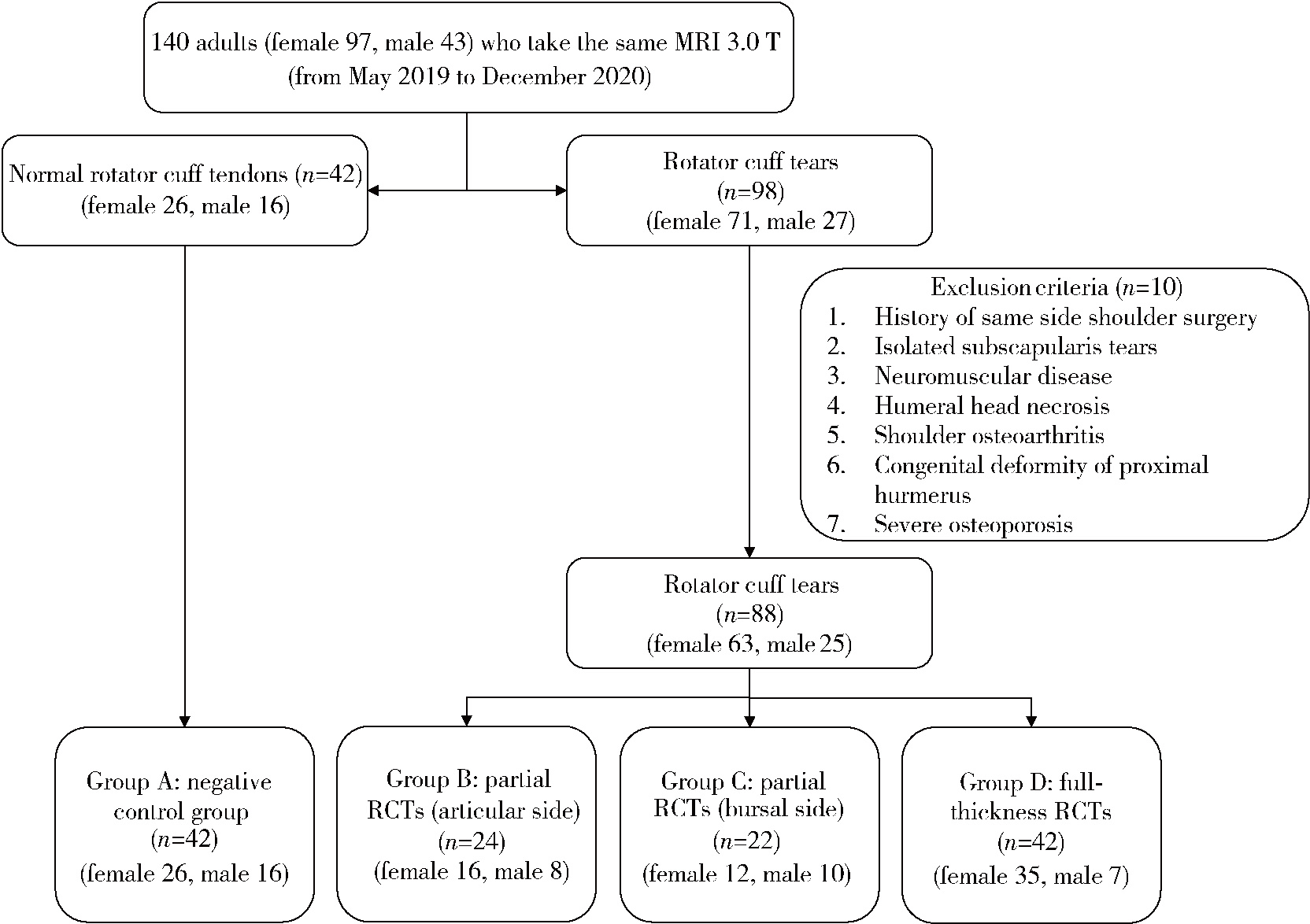
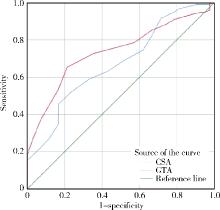
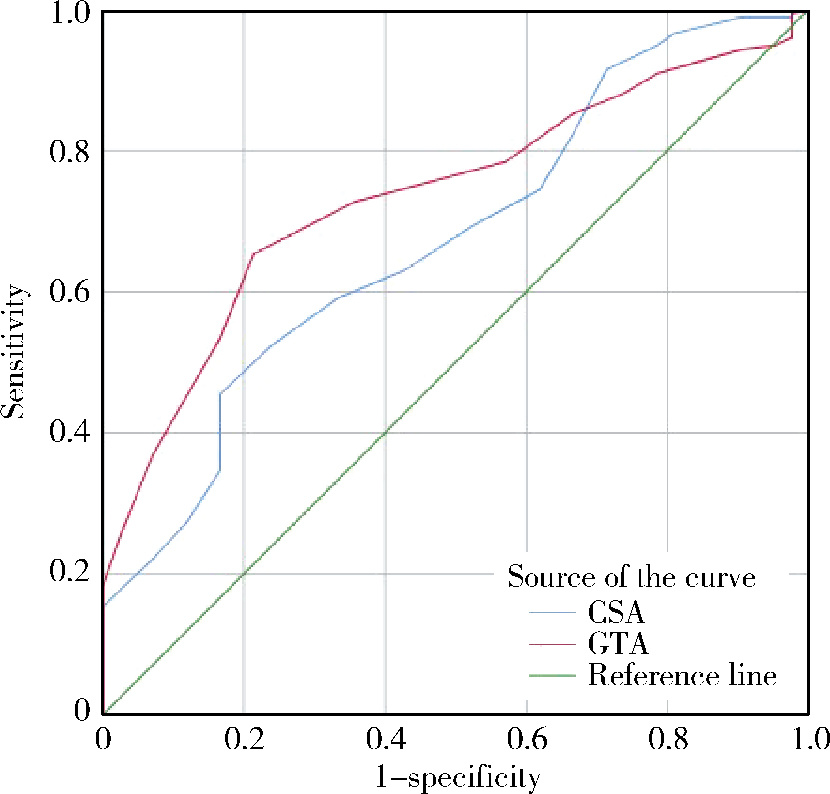
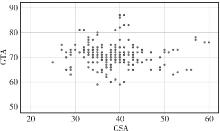
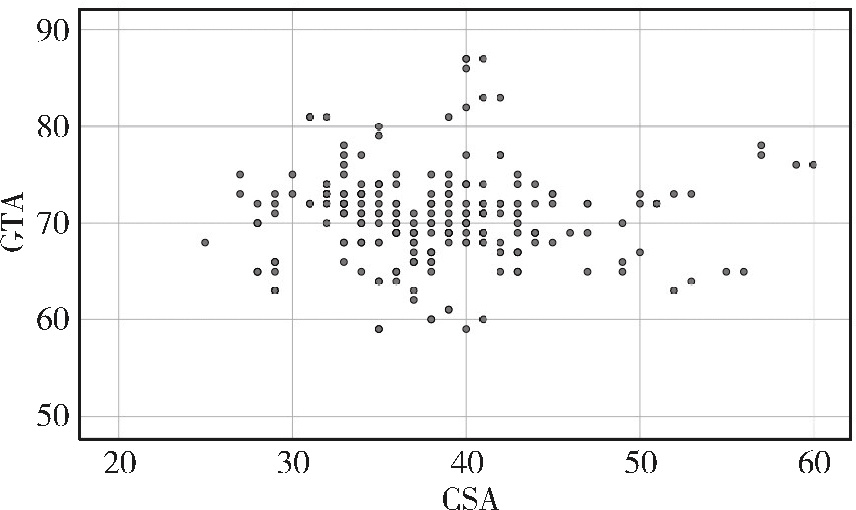
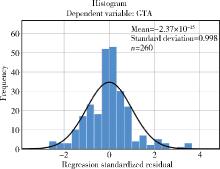
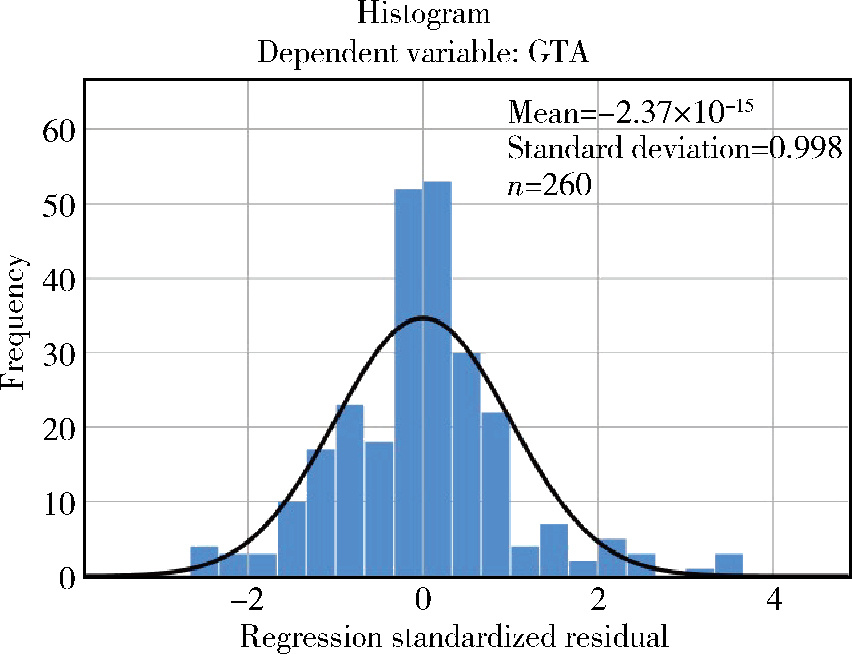
目的: 肱骨大结节角(greater tuberosity angle,GTA)和峰盂角(critical shoulder angle,CSA)通常作为影像学标记用于描述肱骨大结节和肩峰的形态,本研究分析肩袖撕裂患者GTA和CSA的变化趋势和风险阈值,并探讨肩袖撕裂的保护因素和危险因素。方法: 从2019年5月至2020年12月共回顾性纳入130例患者,根据南加州骨科研究所(Southern California Orthopaedic Institute,SCOI)的分类法,将患者分为4组:A组,正常对照组;B组,部分肩袖撕裂(关节侧)组;C组,部分肩袖撕裂(滑囊侧)组;D组,全层肩袖撕裂组。在单盲条件下,由同一组医生分别在手臂中立位的肩胛骨正位X线片上测量GTA和CSA,分析其对肩袖撕裂的诊断价值,同时对可能影响肩袖撕裂的因素进行相关性分析。结果: 根据受试者工作特征(receiver operating characteristic,ROC)曲线下面积(area under curve,AUC),在95%置信区间(confidence interval,CI)内,肩袖撕裂组(B、C、D组)的GTA和CSA分别为0.736和0.673,肩袖撕裂患者的GTA和CSA临界值(cut-off value)分别为70.5°和39.5°。与对照组相比,各肩袖撕裂组在身高、年龄、体重指数(body mass index,BMI)等方面差异均有统计学意义(P < 0.05),全层肩袖撕裂组(D组)患者的年龄更大(P < 0.05,临界值为56.5岁),比A、B组身高更低(P < 0.05,临界值为1.58 m)。散点图和回归分析显示,GTA与CSA之间不存在线性相关。与对照组相比,肩袖撕裂组在性别、优势肩和吸烟等方面差异无统计学意义(P>0.05)。结论: 较大的GTA(>70.5°)和CSA(>39.5°)可能对诊断肩袖撕裂具有较高的预测价值,相较而言,GTA的诊断价值更高;年龄>56.5岁、身高 < 1.58 m的患者更易发生全层肩袖撕裂;性别、优势肩、吸烟既不是危险因素,也不是保护因素。
中图分类号:
- R684




| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
王琦, 王会祥, 吴晓明. 峰盂角的定义及临床研究进展[J]. 中华骨科杂志, 2020, 40 (1): 55- 59.
|
| 8 |
陈俊, 楼珏翔, 申屠国建, 等. 肩关节峰盂角对肩袖撕裂修补术后再撕裂的影响[J]. 中国运动医学杂志, 2022, 41 (6): 423- 429.
doi: 10.3969/j.issn.1000-6710.2022.06.002 |
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
|
| 17 |
|
| 18 |
|
| 19 |
|
| 20 |
|
| 21 |
|
| 22 |
|
| 23 |
|
| 24 |
|
| 25 |
|
| 26 |
|
| 27 |
|
| 28 |
|
| 29 |
|
| 30 |
|
| 31 |
|
| 32 |
|
| 33 |
|
| 34 |
|
| 35 |
|
| 36 |
|
| 37 |
|
| 38 |
|
| 39 |
|
| 40 |
|
| 41 |
|
| [1] | 王翠萍, 陈哲, 程永静. 超微血流成像评估与膝骨关节炎临床症状的关联研究[J]. 北京大学学报(医学版), 2025, 57(6): 1096-1100. |
| [2] | 胡枫艺, 孟庆阳, 陈拿云, 王佳宁, 刘振龙, 马勇, 杨渝平, 龚熹, 王成, 刘平, 史尉利. 镜下内侧髌股复合体重建治疗伴高级别滑车发育不良复发性髌骨脱位的临床疗效[J]. 北京大学学报(医学版), 2025, 57(5): 947-955. |
| [3] | 安思兰,郑群怡,王锴,高姗. 全膝关节置换术后患者早期疼痛的特点及其影响因素[J]. 北京大学学报(医学版), 2024, 56(1): 167-173. |
| [4] | 傅强,高冠英,徐雁,林卓华,孙由静,崔立刚. 无症状髋关节前上盂唇撕裂超声与磁共振检查的对比研究[J]. 北京大学学报(医学版), 2023, 55(4): 665-669. |
| [5] | 吴浩,潘利平,刘恒,塔拉提百克·买买提居马,王洪彬,宁太国,曹永平. 胫骨假体的不同后倾角度对内侧间室单髁置换术后膝关节功能的影响[J]. 北京大学学报(医学版), 2021, 53(5): 877-882. |
| [6] | 郑佳鹏,肖棋,邓辉云,吴清泉,翟文亮,林达生. 外侧半月板腘肌腱区损伤的关节镜下分型和处理[J]. 北京大学学报(医学版), 2021, 53(5): 891-895. |
| [7] | 邵振兴,宋庆法,赵宇晴,崔国庆. 一种结合线袢固定的关节镜下“嵌入式”喙突移位术:手术技术及术后影像学分析[J]. 北京大学学报(医学版), 2021, 53(5): 896-901. |
| [8] | 朱敬先,鲁胜楠,蒋艳芳,姜玲,王健全. 老年肩袖损伤手术患者术前肺功能的影响因素[J]. 北京大学学报(医学版), 2021, 53(5): 902-906. |
| [9] | 刘中砥,许庭珉,党育,张殿英,付中国. 关节镜下改良outside-in穿刺缝合技术修复半月板撕裂的中期临床随访[J]. 北京大学学报(医学版), 2020, 52(5): 870-874. |
| [10] | 江东,胡跃林,焦晨,郭秦炜,谢兴,陈临新,赵峰,皮彦斌. 慢性踝关节不稳合并后踝撞击同期手术中长期疗效及影响因素分析[J]. 北京大学学报(医学版), 2019, 51(3): 505-509. |
| [11] | 张翠平,刘佩佩,傅强,高冠英,崔立刚,徐雁,王健全. 超声引导下髋关节药物注射在关节镜盂唇修复术后康复中的应用[J]. 北京大学学报(医学版), 2019, 51(2): 265-267. |
| [12] | 吕明, 张金庆, 王兴山, 黄野, 李为, 张春雨. 直接前入路髋关节置换术及其早期临床疗效[J]. 北京大学学报(医学版), 2017, 49(2): 206-213. |
| [13] | 李杨,李子剑,张克,田华,刘延青,蔡宏,李锋,赵旻暐. 膝髋关节置换术非计划性暂停手术的原因分析[J]. 北京大学学报(医学版), 2017, 49(2): 231-235. |
| [14] | 张铁超,张志山,周方,田耘,姬洪全,郭琰,吕扬,杨钟玮,侯国进. 颈基底型股骨粗隆部骨折的诊断及治疗[J]. 北京大学学报(医学版), 2017, 49(2): 246-251. |
| [15] | 于峥嵘,李淳德,朱赛楠,孙浩林,赵耀,漆龙涛. 经皮椎间孔入路内镜下神经根减压治疗腰椎管狭窄症的短期随访[J]. 北京大学学报(医学版), 2017, 49(2): 252-255. |
|
||
