北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (2): 351-358. doi: 10.19723/j.issn.1671-167X.2026.02.020
胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素
赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪*( )
)
- 北京大学人民医院重症医学科, 创伤救治中心, 北京 100044
Risk factors for ventilator-associated pneumonia in patients with chest trauma in intensive care unit
Jie ZHAO, Chun FU, Xiujuan ZHAO, Haiyan XUE, Shu LI, Zhenzhou WANG, Fengxue ZHU*()
- Department of Critical Care Medicine, Trauma Treatment Center, Peking University People's Hospital, Beijing 100044, China
摘要:
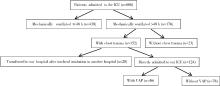
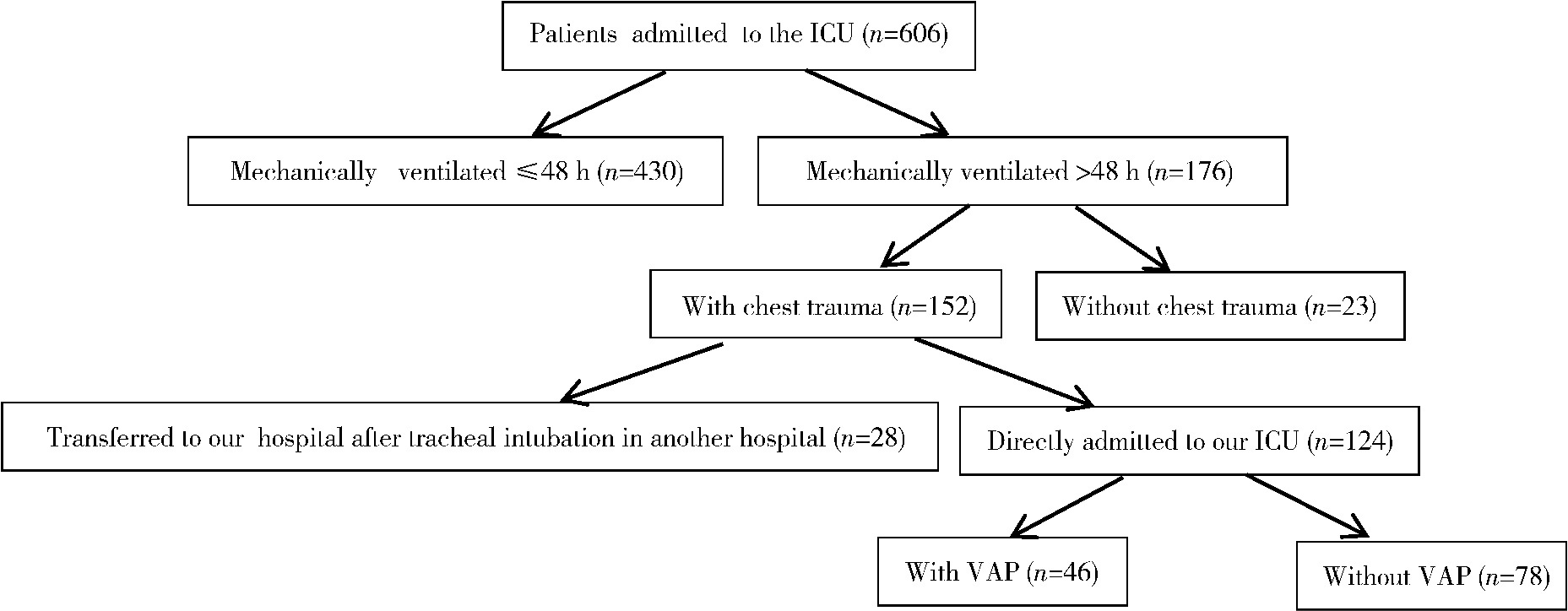
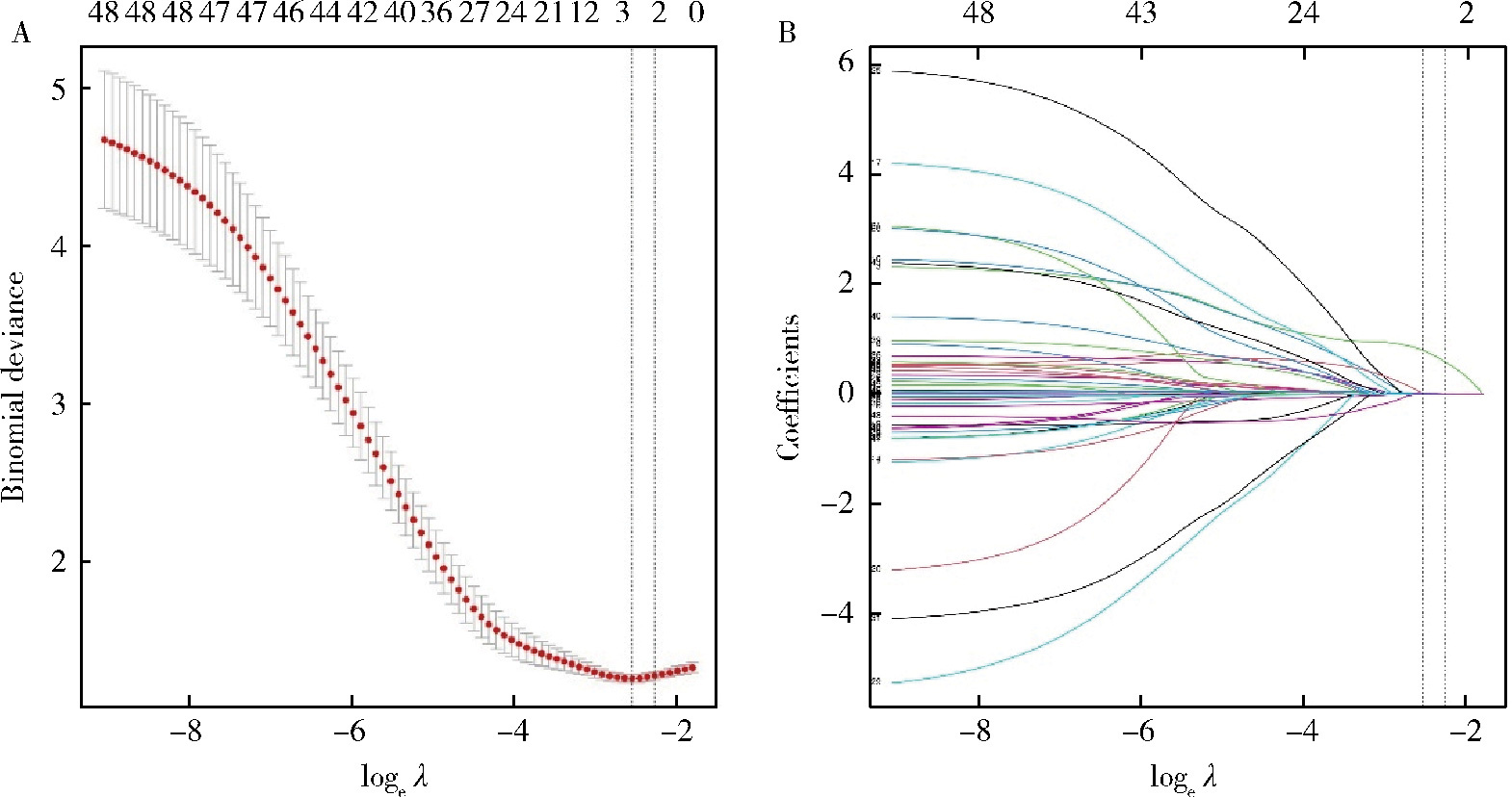
目的: 探讨胸部创伤患者在重症监护病房(intensive care unit, ICU)内发生呼吸机相关性肺炎(ventilator-associated pneumonia,VAP)的危险因素。方法: 回顾性分析2019年6月至2023年6月收住北京大学人民医院外科ICU、入院24 h内进行气管插管且机械通气>48 h的124例成人创伤患者的临床资料。根据住院期间是否发生VAP分为VAP组(46例)和非VAP组(78例),采用Lasso回归分析进行筛选并采用Logistic进行多因素回归分析以确定胸部创伤患者在ICU内发生VAP的危险因素。结果: 多因素回归分析显示,损伤严重度评分(injury severity score,ISS)(OR=1.08,95%CI:1.02~1.14,P=0.007)和气管切开(OR=4.61,95%CI:1.74~13.11,P=0.003)是胸部创伤患者发生VAP的独立危险因素(P < 0.05)。早期VAP患者19例,晚期VAP患者27例。所有VAP病例中,最常见的病原体是肺炎克雷伯菌(Klebsiella pneumoniae),共18次(39.1%);早期VAP病例中肺炎克雷伯菌最多见(10次,52.6%),晚期VAP中铜绿假单胞菌(Pseudomonas aeruginosa)和鲍曼不动杆菌(Acinetobacter baumannii)的出现频率最高,均为10次(37.0%)。结论: 胸部创伤患者在ICU内是否发生VAP与多个因素有关,ISS评分高以及气管切开是胸部创伤患者发生VAP的独立危险因素。
中图分类号:
- R563.1

| 1 |
中华医学会呼吸病学分会感染学组. 中国成人医院获得性肺炎与呼吸机相关性肺炎诊断和治疗指南(2018年版)[J]. 中华结核和呼吸杂志, 2018, 41 (4): 255- 280.
|
| 2 |
doi: 10.1093/cid/ciy543 |
| 3 |
doi: 10.1016/j.jcrc.2023.154284 |
| 4 |
doi: 10.1007/s00134-020-05980-0 |
| 5 |
doi: 10.3390/antibiotics9020051 |
| 6 |
doi: 10.1186/cc13775 |
| 7 |
doi: 10.1093/cid/cis926 |
| 8 |
doi: 10.4187/respcare.05500742 |
| 9 |
doi: 10.1016/j.ijid.2013.02.004 |
| 10 |
doi: 10.4103/0972-5229.130570 |
| 11 |
doi: 10.4066/AMJ.2013.1710 |
| 12 |
|
| 13 |
|
| 14 |
doi: 10.1007/s00268-019-05286-3 |
| 15 |
doi: 10.5455/jmas.42509 |
| 16 |
|
| 17 |
doi: 10.1007/s00134-004-2514-z |
| 18 |
doi: 10.1016/j.ijid.2015.07.005 |
| 19 |
doi: 10.1016/j.amjsurg.2015.06.029 |
| 20 |
doi: 10.5090/kjtcs.2017.50.5.346 |
| 21 |
doi: 10.5847/wjem.j.1920-8642.2018.03.007 |
| 22 |
doi: 10.1089/sur.2006.069 |
| 23 |
doi: 10.1016/j.chest.2020.06.064 |
| 24 |
doi: 10.1007/s12028-019-00773-w |
| 25 |
doi: 10.1016/j.joms.2015.08.018 |
| 26 |
doi: 10.3390/jcm10153319 |
| 27 |
doi: 10.1016/j.jocn.2023.06.004 |
| 28 |
|
| 29 |
doi: 10.3390/jpm12040597 |
| 30 |
doi: 10.1186/s12879-017-2566-7 |
| 31 |
doi: 10.4103/0974-2700.120364 |
| 32 |
doi: 10.5005/jp-journals-10071-24465 |
| 33 |
|
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [3] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [4] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [5] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [6] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [7] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [8] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [9] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [10] | 李钰锴, 王红彦, 罗靓, 李云, 李春. 抗磷脂抗体在白塞病合并血栓中的临床意义[J]. 北京大学学报(医学版), 2024, 56(6): 1036-1040. |
| [11] | 田杨, 韩永正, 李娇, 王明亚, 曲音音, 房景超, 金辉, 李民, 王军, 徐懋, 王圣林, 郭向阳. 颈椎前路手术后硬膜外血肿的发生率和危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1058-1064. |
| [12] | 王明瑞, 赖金惠, 姬家祥, 唐鑫伟, 胡浩浦, 王起, 许克新, 徐涛, 胡浩. 使用中文版威斯康星结石生活质量问卷预测肾结石患者生活质量降低的危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1069-1074. |
| [13] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [14] | 颜野,李小龙,夏海缀,朱学华,张羽婷,张帆,刘可,刘承,马潞林. 前列腺癌根治术后远期膀胱过度活动症的危险因素[J]. 北京大学学报(医学版), 2024, 56(4): 589-593. |
| [15] | 陈延,李况蒙,洪锴,张树栋,程建星,郑仲杰,唐文豪,赵连明,张海涛,姜辉,林浩成. 阴茎海绵体注射试验对阴茎血管功能影响的回顾性研究[J]. 北京大学学报(医学版), 2024, 56(4): 680-686. |
|
||
