北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (5): 863-869. doi: 10.19723/j.issn.1671-167X.2020.05.011
经左胸前外侧微创冠脉搭桥治疗冠心病多支病变
许志锋1,2,凌云鹏2,∆( ),崔仲奇2,赵鸿2,宫一辰2,傅元豪2,杨航2,万峰2
),崔仲奇2,赵鸿2,宫一辰2,傅元豪2,杨航2,万峰2
- 1.北京大学深圳医院心血管外科,广东深圳 518036
2.北京大学第三医院心脏外科,北京 100083
Feasibility and safety of minimally invasive cardiac coronary artery bypass grafting surgery for patients with multivessel coronary artery disease: Early outcome and short-mid-term follow up results
Zhi-feng XU1,2,Yun-peng LING2,∆(),Zhong-qi CUI2,hong ZHAO2,Yi-chen GONG2,Yuan-hao FU2,Hang YANG2,Feng WAN2
- 1. Department of Cardiac Surgery, Peking University Shenzhen Hospital, Shenzhen 518036, Guangdong, China
2. Department of Cardiac Surgery, Peking University Third Hospital, Beijing 100191, China
摘要:
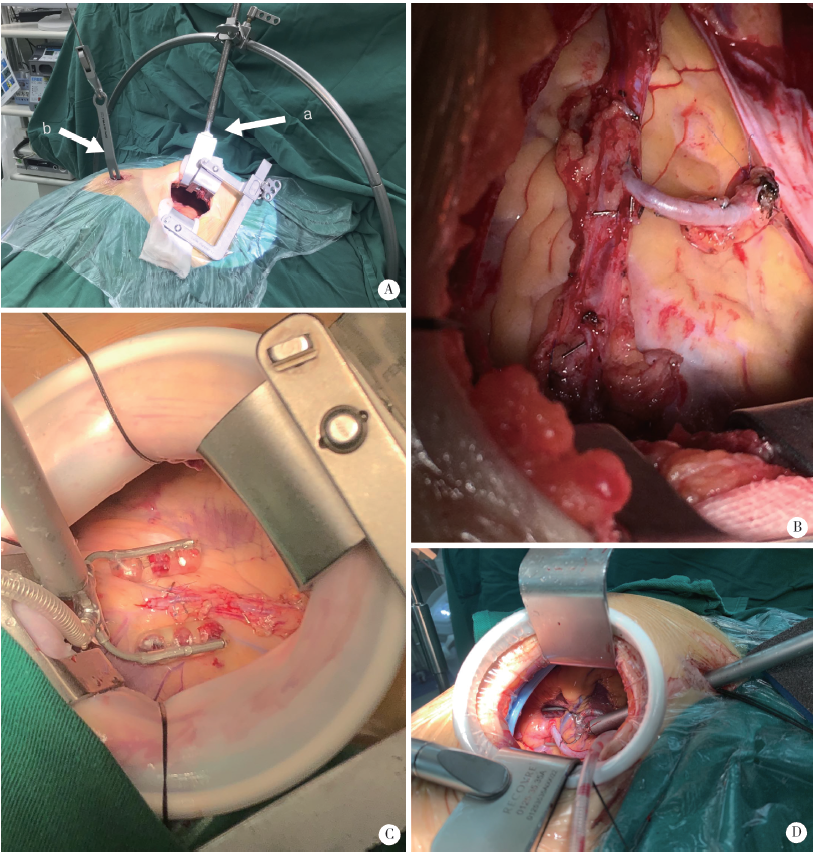
目的:评估经左胸前外侧微创冠脉搭桥术(minimally invasive cardiac surgery coronary artery bypass grafting, MICS CABG)治疗冠心病多支病变的可行性、安全性及近中期临床疗效。方法:选择2015年11月—2017年11月在北京大学第三医院完成的经左胸前外侧微创冠脉搭桥术患者作为实验组(MICS CABG组),同期收集接受常规正中开胸非体外循环冠脉搭桥手术(off-pump coronary aortic bypass grafting, OPCABG)患者,应用倾向性评分匹配法,按照年龄、性别、左心室射血分数、体重指数、冠脉血管病变程度以及是否存在吸烟、糖尿病、高血压病、高脂血症、肾功能不全、脑血管意外史、慢性阻塞性肺病史与接受MICS CABG的患者进行1 ∶1配对作为对照组(OPCABG组)。比较两组患者住院临床资料及近中期随访结果。结果:MICS CABG组共入选85例患者,其中男性68例(80.0%),女性17例(20%),平均年龄(63.8±8.7)岁;OPCABG病例451例,经倾向性评分匹配出85例作为对照组(OPCABG组),匹配后两组基线水平一致(P均>0.05)。MICS CABG 组平均搭桥(2.35±0.83)支/例,对照组平均(2.48±0.72)支/例(P=0.284),MICS CABG组无中转正中开胸者,两组均无中转体外循环手术。MICS CABG组与对照组相比,其术后主要不良心脑血管事件(major adverse cardiacand cerebrovascular events, MACCE)发生率[1.17%(1/85) vs. 3.52%(3/85)]、二次手术率[2.34%(2/85) vs. 3.52%(3/85)]、术后新发心房纤颤率[4.70%(4/85) vs. 3.52%(3/85)]及新发肾功能不全率[1.17%(1/85) vs. 0%(0/85)]差异无统计学意义(均P>0.05)。MICS CABG组手术时间较OPCABG组长[(282.8±55.8) min vs. (246.8±56.9) min, P<0.05],但术后呼吸机使用时间[(16.9±7.8) h vs. (29.6±15.9) h]、术后监护病房住院时间[(29.3±20.8) h vs. (51.5±48.3) h]及住院时间[(18.3±3.2) d vs. (25.7±4.2) d]均较短(均P<0.05)。术后冠脉造影检查,MICS CABG组总体桥血管通畅率(A+B级)为 96.5%。术后随访1年,两组患者MACCE累积发生率差异无统计学意义[1.18%(1/85) vs. 3.61%(3/83), P>0.05]。结论:经左胸前外侧小切口微创冠状动脉搭桥手术安全可行,近中期随访结果良好,MICS CABG出院更早,恢复更快。
中图分类号:
- R654



| [1] |
Yi G, Shine B, Rehman SM, et al. Effect of bilateral internal mammary artery grafts on long-term survival: a meta-analysis approach[J]. Circulation, 2014,130(7):539-545.
doi: 10.1161/CIRCULATIONAHA.113.004255 |
| [2] |
Ahn M, Park DW, Lee CW, et al. Comparison of stenting versus bypass surgery according to the completeness of revascularization in severe coronary artery disease: patient-level pooled analysis of the SYNTAX, PRECOMBAT, and BEST trials[J]. JACC Cardiovasc Interv, 2017,10(14):1415-1424.
doi: 10.1016/j.jcin.2017.04.037 pmid: 28728654 |
| [3] | 郑宝荣, 王联群, 刘建实, 等. 探讨Sino SCORE系统对非体外循环下冠状动脉旁路移植术风险评估的价值[J]. 中国循环杂志, 2013,28(5):375-378. |
| [4] |
Kikuchi K, Chen X, Mori M, et al. Perioperative outcomes of off-pump minimally invasive coronary artery bypass grafting with bilateral internal thoracic arteries under direct vision[J]. Interact Cardiovasc Thorac Surg, 2017,24(5):696-701.
doi: 10.1093/icvts/ivw431 pmid: 28329064 |
| [5] |
Nambiar P, Kumar S, Mittal CM, et al. Minimally invasive coronary artery bypass grafting with bilateral internal thoracic arteries: will this be the future[J]. J Thorac Cardiovasc Surg, 2017,155(1):190-197.
pmid: 29102209 |
| [6] | 张希涛, 高杰, 刘岩, 等. 腔镜获取大隐静脉在糖尿病患者心脏不停跳冠状动脉旁路移植术的应用[J]. 中华胸心血管外科杂志, 2016,32(3):159-161. |
| [7] |
Chan V, Lapierre H, Sohmer B, et al. Handsewn proximal anastomoses onto the ascending aorta through a small left thoracotomy during minimally invasive multivessel coronary artery bypass grafting: a stepwise approach to safety and reproducibility[J]. Semin Thorac Cardiov Surg, 2012,24(1):79-83.
doi: 10.1053/j.semtcvs.2011.12.010 |
| [8] | 杨威, 凌云鹏, 陈彧. 左胸前外侧小切口冠状动脉旁路移植术学习曲线[J]. 中国微创外科杂志, 2015,15(11):990-994. |
| [9] |
Dijk DV, Nierich AP, Jansen EWL, et al. Early outcome after off-pump vs. on-pump coronary bypass surgery results from a randomized study[J]. Circulation, 2001,104(15):1761-1766.
doi: 10.1161/hc4001.097036 pmid: 11591611 |
| [10] |
Kim YH, Oh HC, Choi JW, et al. No-touch saphenous vein harvesting may improve further the patency of saphenous vein com-posite grafts: early outcomes and 1-year angiographic results[J]. Ann Thorac Surg, 2017,103(5):1489-1497.
doi: 10.1016/j.athoracsur.2016.09.024 pmid: 27916241 |
| [11] | Kikuchi K, Une D, Suzuki K, et al. Off-pump minimally invasive coronary artery bypass grafting with a heart positioner: direct retraction for a better exposure[J]. Innovations, 2015,10(5):183-187. |
| [12] | Nambiar P, Mittal C. Minimally invasive coronary bypass using internal thoracic arteries via a left minithoracotomy: “the Nambiar Technique”[J]. Innovations, 2013,8(2):420-426. |
| [13] | 杨俊峰, 顾承雄, 韦华, 等. 非体外循环下双侧乳内动脉Y型桥的冠状动脉旁路移植术125例[J]. 中华外科杂志, 2006,44(22):1529-1531. |
| [14] | Glineur D, Etienne PY, Kuschner CE, et al. Bilateral internal mammary artery Y construct with multiple sequential grafting improves survival compared to bilateral internal mammary artery with additional vein grafts: 10-year experience at 2 different institutions[J]. Eur J Cardio-Thorac, 2017,51(2):368-375. |
| [15] |
Kikuchi K, Mori M. Less-invasive coronary artery bypass grafting international landscape and progress[J]. Curr Opin Cardiol, 2017,32(6):715-721.
doi: 10.1097/HCO.0000000000000461 pmid: 28858911 |
| [1] | 李斌, 梁寒. 机器人胃癌根治术:研究进展与实践挑战[J]. 北京大学学报(医学版), 2026, 58(2): 416-422. |
| [2] | 林国中,马长城,吴超,司雨. 经锁孔入路显微外科切除腰椎管肿瘤54例临床研究[J]. 北京大学学报(医学版), 2022, 54(2): 315-319. |
| [3] | 越雷,王月田,白纯碧,陈浩,付豪永,于峥嵘,李淳德,孙浩林. 内镜治疗中青年双节段腰椎间盘突出症患者的手术策略[J]. 北京大学学报(医学版), 2021, 53(4): 734-739. |
| [4] | 熊盛炜,王杰,朱伟杰,程嗣达,张雷,李学松,周利群. 二次肾盂成形术在复发性肾盂输尿管连接部梗阻中的研究进展[J]. 北京大学学报(医学版), 2020, 52(4): 794-798. |
| [5] | 易端,朱薇,孟秀丽,刘晓光,李水清,祝斌,贾东林. 慢性腰腿痛患者微创术前焦虑,抑郁状态及相关影响因素分析[J]. 北京大学学报(医学版), 2020, 52(2): 285-289. |
| [6] | 段登辉,王恩博,崔念晖,翟新利,刘宇,孟娟红,张伟,张益. 下颌阻生智齿拔除手术的可预期微创化[J]. 北京大学学报(医学版), 2020, 52(2): 395-403. |
| [7] | 丁光璞,程嗣达,方冬,杨昆霖,李学松,周辉霞,张骞,叶雄俊,周利群. 上尿路微创手术的技术改良[J]. 北京大学学报(医学版), 2019, 51(4): 610-614. |
| [8] | 熊盛炜,杨昆霖,丁光璞,郝瀚,李学松,周利群,郭应禄. 输尿管损伤外科修复治疗的研究进展[J]. 北京大学学报(医学版), 2019, 51(4): 783-789. |
| [9] | 刘冰川,杨钟玮,周方,姬洪全,张志山,郭琰,田耘. 肱骨近端骨折微创锁定钢板改良内固定的疗效分析[J]. 北京大学学报(医学版), 2019, 51(2): 277-282. |
| [10] | 张铃福,侯纯升,黄永辉,徐智,王立新,凌晓锋,王港,崔龙,修典荣. 胃空肠吻合术后胆总管结石腹腔镜手术取石和内镜取石的比较[J]. 北京大学学报(医学版), 2019, 51(2): 345-348. |
| [11] | 张鲁锋,凌云鹏, 杨航, 宫一辰, 宋之明, 万峰. 两种微创旁路移植手术治疗多支冠状动脉病变效果的对比[J]. 北京大学学报(医学版), 2017, 49(6): 1066-1070. |
| [12] | 徐杰,庄伟达,李新炜,俞国雨,林院,罗奋棋,肖毓华. 直接前入路和后外侧保留梨状肌入路全髋关节置换术的疗效对比[J]. 北京大学学报(医学版), 2017, 49(2): 214-220. |
| [13] | 张洪,马云青. 直接前入路人工全髋关节置换术[J]. 北京大学学报(医学版), 2017, 49(2): 185-187. |
| [14] | 赵丽萍, 詹雅琳, 胡文杰, 王浩杰, 危伊萍, 甄敏, 徐涛, 刘云松. 磨牙位点保存后进行种植修复及软组织增量的1例报告[J]. 北京大学学报(医学版), 2016, 48(6): 1090-1094. |
| [15] | 刘波,陈山林,朱瑾,王志新,杨辰,沈杰,田光磊. 腕关节镜辅助微创治疗月骨周围脱位[J]. 北京大学学报(医学版), 2016, 48(2): 234-236. |
|
||
