北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (6): 1088-1093. doi: 10.19723/j.issn.1671-167X.2021.06.014
88例重叠肌炎的临床及免疫学特征
肖云抒1,朱冯赟智2,罗澜2,邢晓燕2,李玉慧2,△( ),张学武2,沈丹华1
),张学武2,沈丹华1
- 1.北京大学人民医院病理科,北京 100044
2.北京大学人民医院风湿免疫科,北京 100044
Clinical and immunological characteristics of 88 cases of overlap myositis
XIAO Yun-shu1,ZHU Feng-yun-zhi2,LUO Lan2,XING Xiao-yan2,LI Yu-hui2,△(),ZHANG Xue-wu2,SHEN Dan-hua1
- 1. Department of Pathology, Peking University People’s Hospital, Beijing 100044, China
2. Department of Rheumatology and Immunology, Peking University People’s Hospital, Beijing 100044, China
摘要:
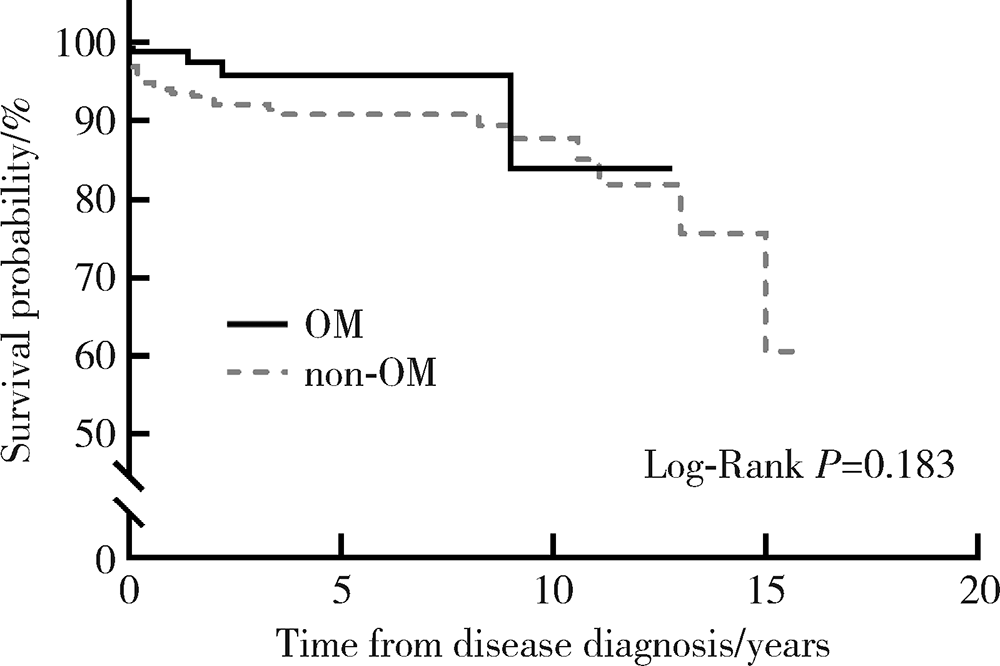
目的:探讨重叠肌炎 (overlap myositis, OM) 患者的临床及免疫学特征。方法:对2004年1月至2020年8月于北京大学人民医院住院的特发性炎性肌病 (idiopathic inflammatory myopathies,IIMs) 患者资料进行回顾性分析,包括人口学特征、临床症状、实验室指标、免疫学指标(抗核抗体、类风湿因子、肌炎相关性抗体、肌炎特异性抗体)、生存情况,并比较OM和其他炎性肌病患者的临床和实验室特点及预后差别。结果:共纳入368例IIMs患者,其中OM患者占23.9% (88/368)。OM患者女性占85.2% (75/88),中位病程13.5个月,结缔组织病(connective tissue disease, CTD)合并皮肌炎(dermatomyositis, DM)、多肌炎(polymyositis, PM)、免疫介导坏死性肌病(immune-mediated necrotizing myopathy, IMNM)、抗合成酶综合征(anti-synthetase syndrome, ASS)分别为 60.2%、3.4%、2.3%、 34.1%。OM患者和非OM患者相比,女性比例高(85.2% vs. 72.1%, P=0.016),病程长[13.5(4.5, 48.0)月 vs. 4.0(2.0,12.0)月,P<0.001)]。在临床特点方面,OM患者比非OM患者V型疹(25.0% vs. 44.6%, P=0.001)、甲周红斑(8.0% vs. 19.6%, P=0.013)发生率低,雷诺现象(14.8% vs. 1.8%, P<0.001)、间质性肺炎(88.6% vs. 72.1%, P=0.001)、肺动脉高压(22.7% vs. 7.5%, P<0.001)、心脏受累(18.2% vs. 9.3%, P=0.033)发生率高。在免疫学特点方面,天门冬氨酸氨基转移酶升高比例低(31.8% vs. 45.0%, P=0.035), C反应蛋白升高比例高(58.0% vs. 44.6%, P=0.037),抗核抗体(85.1% vs. 63.4%, P=0.001)、类风湿因子(40.2% vs. 17.8%, P<0.001)、抗Ro-52抗体(71.6% vs. 56.1%,P=0.038)阳性率高。OM患者和非OM患者的预后无明显差异。结论:OM出现脏器受累多见,易合并肺动脉高压、心脏损害。
中图分类号:
- R593.26

| [1] |
Lilleker JB, Vencovsky J, Wang G, et al. The EuroMyositis registry: an international collaborative tool to facilitate myositis research[J]. Ann Rheum Dis, 2018, 77(1):30-39.
doi: 10.1136/annrheumdis-2017-211868 pmid: 28855174 |
| [2] |
Aguila LA, Lopes MR, Pretti FZ, et al. Clinical and laboratory features of overlap syndromes of idiopathic inflammatory myopathies associated with systemic lupus erythematosus, systemic sclerosis, or rheumatoid arthritis[J]. Clin Rheumatol, 2014, 33(8):1093-1098.
doi: 10.1007/s10067-014-2730-z |
| [3] |
Nuño-Nuño L, Joven BE, Carreira PE, et al. Overlap myositis, a distinct entity beyond primary inflammatory myositis: a retrospective analysis of a large cohort from the REMICAM registry[J]. Int J Rheum Dis, 2019, 22(8):1393-1401.
doi: 10.1111/1756-185X.13559 pmid: 30968571 |
| [4] |
Lundberg IE, Tjärnlund A, Bottai M, et al. EULAR/ACR Classification Criteria for Adult and Juvenile Idiopathic Inflammatory Myopathies and their Major Subgroups[J]. Arthritis Rheumatol, 2017, 69(12):2271-2282.
doi: 10.1002/art.40320 |
| [5] | Dalakas MC. Polymyositis, dermatomyositis and inclusion-body myositis[J]. N Engl J Med, 1991, 325(21):1487-1498. |
| [6] |
van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism Collaborative Initiative[J]. Arthritis Rheum, 2013, 65(11):2737-2747.
doi: 10.1002/art.38098 |
| [7] |
Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism Collaborative Initiative[J]. Arthritis Rheum, 2010, 62(9):2569-2581.
doi: 10.1002/art.27584 |
| [8] |
VitaliC, Bombardiefi S, Josson R, et al. Classification criteria for Sjögren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group[J]. Ann Rheum Dis, 2002, 61(6):554-558.
pmid: 12006334 |
| [9] |
Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus[J]. Arthritis Rheumatol, 2019, 71(9):1400-1412.
doi: 10.1002/art.40930 |
| [10] |
Solomon J, Swigris JJ, Brown KK. Myositis-related interstitial lung disease and antisynthetase syndrome[J]. J Bras Pneumol, 2011, 37(1):100-109.
doi: S1806-37132011000100015 pmid: 21390438 |
| [11] |
Chinniah KJ, Mody GM. The spectrum of idiopathic inflammatory myopathies in South Africa[J]. Clinical rheumatology, 2020, 40(4):1437-1446.
doi: 10.1007/s10067-020-05048-w |
| [12] |
Troyanov Y, Targoff IN, Tremblay JL, et al. Novel classification of idiopathic inflammatory myopathies based on overlap syndrome features and autoantibodies: analysis of 100 French Canadian patients[J]. Medicine (Baltimore), 2005, 84(4):231-249.
doi: 10.1097/01.md.0000173991.74008.b0 |
| [13] |
Cobo-Ibáñez T, López-Longo FJ, Joven B, et al. Long-term pulmonary outcomes and mortality in idiopathic inflammatory myopathies associated with interstitial lung disease[J]. Clinical Rheumatology, 2019, 38(3):803-815.
doi: 10.1007/s10067-018-4353-2 pmid: 30392161 |
| [14] |
Zhang L, Wu G, Gao D, et al. Factors associated with interstitial lung disease in patients with polymyositis and dermatomyositis: a systematic review and meta-analysis[J]. PLoS One, 2016, 11(5):e0155381.
doi: 10.1371/journal.pone.0155381 |
| [15] |
Keser G, Capar I, Aksu K, et al. Pulmonary hypertension in rheumatoid arthritis[J]. Scand J Rheumatol, 2004, 33(4):244-245.
pmid: 15370720 |
| [16] | Kobak S, Kalkan S, Bahadır Kirilmaz, et al. Pulmonary arterial hypertension in patients with primary Sjögren’s syndrome[J]. Autoimmune diseases, 2014, 2014:710401. |
| [17] |
Sanges S, Yelnik CM, Sitbon O, et al. Pulmonary arterial hypertension in idiopathic inflammatory myopathies: data from the French pulmonary hypertension registry and review of the literature[J]. Medicine (Baltimore), 2016, 95(39):e4911.
doi: 10.1097/MD.0000000000004911 |
| [18] |
Barba T, Mainbourg S, Nasser M, et al. Lung diseases in inflammatory myopathies[J]. Semin Respir Crit Care Med, 2019, 40(2):255-270.
doi: 10.1055/s-0039-1685187 |
| [19] |
Condliffe R, Howard L. Connective tissue disease-associated pulmonary arterial hypertension[J]. F1000Prime Reports, 2015, 7:6.
doi: 10.12703/P7-06 pmid: 25705389 |
| [20] |
Aithala R, Alex AG, Danda D. Pulmonary hypertension in connective tissue diseases: an update[J]. Int J Rheum Dis, 2017, 20(1):5-24.
doi: 10.1111/1756-185X.13001 pmid: 28205373 |
| [21] |
Albrecht K, Huscher D, Callhoff J, et al. Trends in idiopathic inflammatory myopathies: cross-sectional data from the German National Database[J]. Rheumatol Int, 2020, 40(10):1639-1647.
doi: 10.1007/s00296-020-04634-0 pmid: 32594219 |
| [22] |
Ruiz-Cano MJ, Escribano P, Alonso R, et al. Comparison of baseline characteristics and survival between patients with idiopathic and connective tissue disease-related pulmonary arterial hypertension[J]. J Heart Lung Transplant, 2009, 28(6):621-627.
doi: 10.1016/j.healun.2009.02.016 |
| [23] |
Jayakumar D, Zhang R, Wasserman A, et al. Cardiac manifestations in idiopathic inflammatory myopathies: an overview[J]. Cardiol Rev, 2019, 27(3):131-137.
doi: 10.1097/CRD.0000000000000241 pmid: 30585794 |
| [24] |
Gupta R, Wayangankar SA, Targoff IN, et al. Clinical cardiac involvement in idiopathic inflammatory myopathies: a systematic review[J]. Int J Cardiol, 2011, 148(3):261-270.
doi: 10.1016/j.ijcard.2010.08.013 |
| [25] |
Danieli MG, Gambini S, Pettinari L, et al. Impact of treatment on survival in polymyositis and dermatomyositis. A single-centre long-term follow-up study[J]. Autoimmun Rev, 2014, 13(10):1048-1054.
doi: 10.1016/j.autrev.2014.08.023 |
| [26] | Lundberg IE. The heart in dermatomyositis and polymyositis[J]. Rheumatology (Oxford), 2006, 45(Suppl 4):18-21. |
| [27] |
Lu Z, Guo-Chun W, Li M, et al. Cardiac involvement in adult polymyositis or dermatomyositis: a systematic review[J]. Clin Cardiol, 2012, 35(11):685-691.
doi: 10.1002/clc.v35.11 |
| [28] |
Iaccarino L, Gatto M, Bettio S, et al. Overlap connective tissue disease syndromes[J]. Autoimmun Rev, 2013, 12(3):363-373.
doi: 10.1016/j.autrev.2012.06.004 pmid: 22743033 |
| [29] |
Betteridge Z, Tansley S, Shaddick G, et al. Frequency, mutual exclusivity and clinical associations of myositis autoantibodies in a combined European cohort of idiopathic inflammatory myopathy patients[J]. J Autoimmun, 2019, 101:48-55.
doi: S0896-8411(19)30100-3 pmid: 30992170 |
| [30] |
Rigolet A, Musset L, Dubourg O, et al. Inflammatory myopathies with anti-Ku antibodies: a prognosis dependent on associated lung disease[J]. Medicine (Baltimore), 2012, 91(2):95-102.
doi: 10.1097/MD.0b013e31824d9cec |
| [31] |
Maundrell A, Proudman S, Limaye V. Prevalence of other connective tissue diseases in idiopathic inflammatory myopathies[J]. Rheumatol Int, 2019, 39(10):1777-1781.
doi: 10.1007/s00296-019-04411-8 pmid: 31385080 |
| [32] |
Ng KP, Ramos F, Sultan SM, et al. Concomitant diseases in a cohort of patients with idiopathic myositis during long-term follow-up[J]. Clin Rheumatol, 2009, 28(8):947-953.
doi: 10.1007/s10067-009-1181-4 pmid: 19387765 |
| [33] |
Torres C, Belmonte R, Carmona L, et al. Survival, mortality and causes of death in inflammatory myopathies[J]. Autoimmunity, 2006, 39(3):205-215.
doi: 10.1080/08916930600622603 |
| [34] |
Amaral Silva M, Cogollo E, Isenberg DA. Why do patients with myositis die? A retrospective analysis of a single-centre cohort[J]. Clin Exp Rheumatol, 2016, 34(5):820-826.
pmid: 27494511 |
| [1] | 初吉燕, 李萍, 田竞, 付笛语, 郭琳, 孙蕊, 李亚娣. 黑色素瘤缺乏因子2介导的细胞焦亡通路在特发性炎性肌病患者外周血单个核细胞中的表达[J]. 北京大学学报(医学版), 2026, 58(1): 175-183. |
| [2] | 练益瑞, 刘静璇, 赵亮, 赵静, 臧思田, 李玉慧. 抗PM/Scl抗体相关风湿性疾病谱及其在特发性炎性肌病中的免疫学特征[J]. 北京大学学报(医学版), 2025, 57(6): 1018-1023. |
| [3] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
| [4] | 赖展鸿,李嘉辰,贠泽霖,张永刚,张昊,邢晓燕,邵苗,金月波,王乃迪,李依敏,李玉慧,栗占国. 特发性炎性肌病完全临床应答相关因素的单中心真实世界研究[J]. 北京大学学报(医学版), 2024, 56(2): 284-292. |
| [5] | 孟彦宏,陈怡帆,周培茹. CENP-B抗体阳性的原发性干燥综合征患者的临床和免疫学特征[J]. 北京大学学报(医学版), 2023, 55(6): 1088-1096. |
| [6] | 张璐,陈澄,翁梅婷,郑爱萍,苏美玲,王庆文,蔡月明. 狼疮肾炎患者肾小管间质损伤的自身抗体特征[J]. 北京大学学报(医学版), 2022, 54(6): 1094-1098. |
| [7] | 张琳崎,赵静,王红彦,王宗沂,李英妮,汤稷旸,李思莹,曲进锋,赵明威. 抗ENO1抗体与狼疮性视网膜病变的相关性[J]. 北京大学学报(医学版), 2022, 54(6): 1099-1105. |
| [8] | 罗澜,邢晓燕,肖云抒,陈珂彦,朱冯赟智,张学武,李玉慧. 抗合成酶综合征合并心脏受累患者的临床及免疫学特征[J]. 北京大学学报(医学版), 2021, 53(6): 1078-1082. |
| [9] | 赵静,孙峰,李云,赵晓珍,徐丹,李英妮,李玉慧,孙晓麟. 抗α-1C微管蛋白抗体在系统性硬化症中的表达及临床意义[J]. 北京大学学报(医学版), 2020, 52(6): 1009-1013. |
| [10] | 郑艺明,郝洪军,刘怡琳,郭晶,赵亚雯,张巍,袁云. Ro52抗体与其他肌炎抗体共阳性的相关性研究[J]. 北京大学学报(医学版), 2020, 52(6): 1088-1092. |
| [11] | 朱冯赟智,邢晓燕,汤晓菲,李依敏,邵苗,张学武,李玉慧,孙晓麟,何菁. 肌炎合并血栓栓塞患者的临床及免疫学特征[J]. 北京大学学报(医学版), 2020, 52(6): 995-1000. |
| [12] | 李英妮,相晓红,赵静,李云,孙峰,王红彦,贾汝琳,胡凡磊. 抗类瓜氨酸化抗体在系统性红斑狼疮中的意义[J]. 北京大学学报(医学版), 2019, 51(6): 1019-1024. |
| [13] | 卢昕,张立宁. 肌活检在特发性炎性肌病诊断和临床分型中的价值[J]. 北京大学学报(医学版), 2018, 50(6): 949-951. |
| [14] | 王永福,刘媛. 自身抗体在肿瘤及感染性疾病发生、发展中的作用[J]. 北京大学学报(医学版), 2018, 50(6): 952-955. |
| [15] | 郭晓玥,邵珲,赵扬玉. 系统性红斑狼疮患者孕期并发肺动脉高压1例[J]. 北京大学学报(医学版), 2018, 50(5): 928-931. |
|
||
