北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (3): 450-457. doi: 10.19723/j.issn.1671-167X.2022.03.009
基于马尔可夫模型的社区人群糖尿病筛查预防心血管病的效果评价
王佳敏1,刘秋萍1,张明露1,巩超1,刘舒丹1,陈暐烨1,沈鹏2,林鸿波2,高培1,3,*( ),唐迅1,*()
),唐迅1,*()
- 1. 北京大学公共卫生学院流行病与卫生统计学系, 北京 10019
2. 宁波市鄞州区疾病预防控制中心, 浙江宁波 3151011
3. 北京大学临床研究所真实世界证据评价中心, 北京 100191
Effectiveness of different screening strategies for type 2 diabete on preventing cardiovascular diseases in a community-based Chinese population using a decision-analytic Markov model
Jia-min WANG1,Qiu-ping LIU1,Ming-lu ZHANG1,Chao GONG1,Shu-dan LIU1,Wei-ye CHEN1,Peng SHEN2,Hong-bo LIN2,Pei GAO1,3,*(),Xun TANG1,*()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Yinzhou District Center for Disease Control and Prevention, Ningbo 315101, Zhejiang, China
3. Center for Real-World Evidence Evaluation, Clinical Research Institute, Peking University, Beijing 100191, China
摘要:
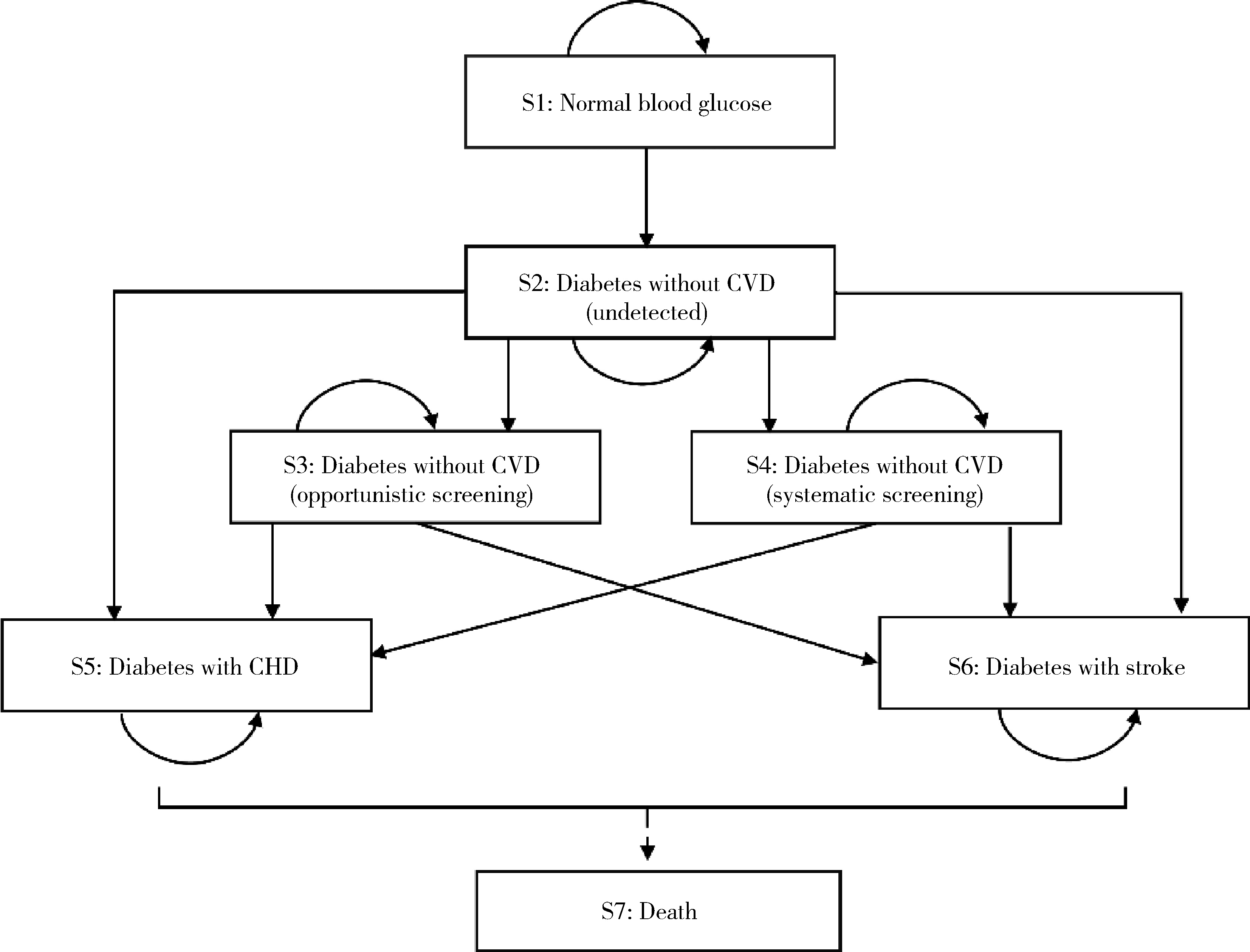
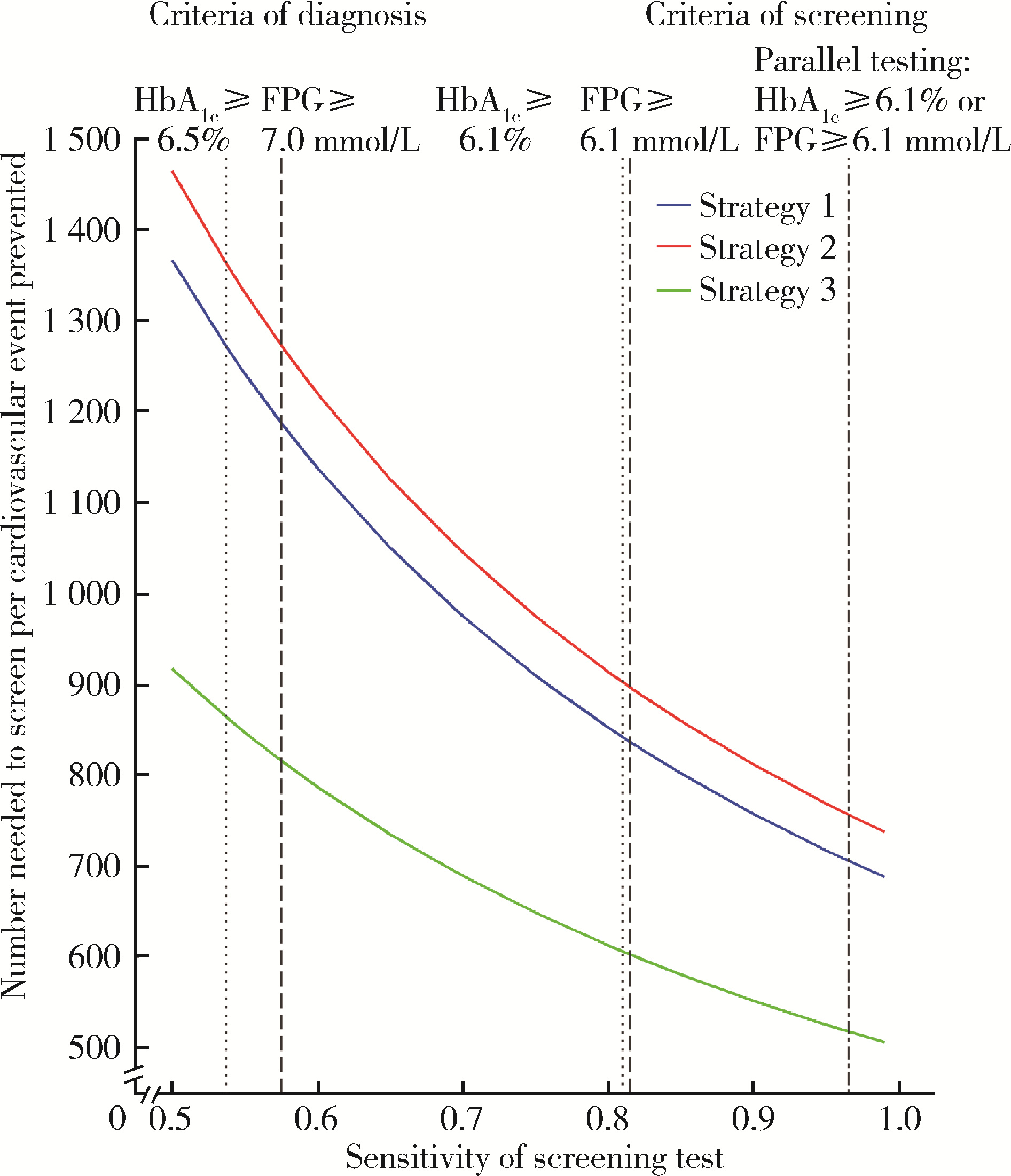
目的: 在中国鄞州电子健康档案研究(Chinese electronic health records research in Yinzhou, CHERRY)的队列人群中,评估国内外不同指南最新推荐的2型糖尿病筛查策略在我国发达地区人群中预防心血管病的效果。方法: 采用马尔可夫(Markov)模型模拟并比较的系统性筛查策略包括:(1) 根据《中国2型糖尿病防治指南(2020年版)》的推荐,在40~70岁人群中筛查(策略1);(2) 根据2022年美国糖尿病学会《糖尿病医学诊疗标准》的推荐,在35~70岁人群中筛查(策略2);(3)根据美国预防服务工作组2021年更新的《2型糖尿病的筛查建议声明》的推荐,在35~70岁且超重或肥胖(体重指数24 kg/m2及以上)的人群中进行筛查(策略3)。根据指南推荐,对筛查阳性(空腹血糖7.0 mmol/L及以上)的人群强化控制血糖以达到目标值(糖化血红蛋白控制在7.0%以下)。马尔可夫模型循环周期设为1年,研究期限设为10年,模拟10个周期,计算的结局指标包括心血管病事件发病数和全因死亡数等结局事件数,以及每预防一例心血管病事件或全因死亡需筛查人数等效果评价指标。马尔可夫模型的参数主要来源于CHERRY队列人群和公开发表的文献。采用单因素敏感性分析探讨筛查方法的灵敏度变化对结果的影响,采用概率敏感性分析探讨糖尿病发病率、筛查方法的灵敏度、强化干预措施的效应强度等参数的不确定性。结果: 研究纳入的289 245名基线无心血管病且未诊断糖尿病的35~70岁人群中,与机会性筛查相比,在40~70岁人群中进行系统性筛查的策略1可预防的心血管病发病数为222[95%不确定性区间(uncertainty interval, UI):180~264]例,在35~70岁人群中筛查的策略2为227(95%UI: 185~271)例,在35~70岁且超重或肥胖人群中筛查的策略3为131(95%UI: 98~164)例。每预防一例心血管病发病数的需筛查人数在策略1、2和3分别为1 184(95%UI: 994~1 456)人、1 274(95%UI: 1 067~1 564)人和814(95%UI: 649~1 091)人。策略2相比策略1每预防一例心血管病的需筛查人数增加90(95%UI: -197~381)人,但心血管病预防效果相似; 策略3相比策略2的需筛查人数减少460(95%UI: 185~724)人,筛查效率更高。单因素敏感性分析和概率敏感性分析的结果与主分析结果一致。结论: 在我国发达地区人群中,根据现有的最新指南开展糖尿病系统性筛查能够减少心血管病发病和全因死亡,但仅降低筛查起始年龄从40岁到35岁对预防心血管病效果的增益并不明显,如果降低筛查的起始年龄到35岁需要同时考虑超重或肥胖的危险因素以便提高筛查效率。
中图分类号:
- R181.3+8


| 1 |
Visseren FLJ , Mach F , Smulders YM , et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice[J]. Eur Heart J, 2021, 42 (34): 3227- 3337.
doi: 10.1093/eurheartj/ehab484 |
| 2 |
Liss D T , Uchida T , Wilkes CL , et al. General health checks in adult primary care: A review[J]. JAMA, 2021, 325 (22): 2294- 2306.
doi: 10.1001/jama.2021.6524 |
| 3 | 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志, 2021, 13 (4): 315- 409. |
| 4 | American Diabetes Association Professional Practice Committee . Classification and diagnosis of diabetes: Standards of medical care in diabetes: 2022[J]. Diabetes Care, 2021, 45 (Suppl 1): S17- S38. |
| 5 |
US Preventive Services Task Force . Screening for prediabetes and type 2 diabetes: US Preventive Services Task Force recommendation statement[J]. JAMA, 2021, 326 (8): 736- 743.
doi: 10.1001/jama.2021.12531 |
| 6 |
Wang L , Peng W , Zhao Z , et al. Prevalence and treatment of diabetes in China, 2013-2018[J]. JAMA, 2021, 326 (24): 2498- 2506.
doi: 10.1001/jama.2021.22208 |
| 7 |
Lin H , Tang X , Shen P , et al. Using big data to improve cardiovascular care and outcomes in China: A protocol for the Chinese electronic health records research in Yinzhou (CHERRY) study[J]. BMJ Open, 2018, 8 (2): e019698.
doi: 10.1136/bmjopen-2017-019698 |
| 8 |
Kaptoge S , Pennells L , De Bacquer D , et al. World Health Organization cardiovascular disease risk charts: Revised models to estimate risk in 21 global regions[J]. Lancet Global Health, 2019, 7 (10): e1332- e1345.
doi: 10.1016/S2214-109X(19)30318-3 |
| 9 |
Porta M , Curletto G , Cipullo D , et al. Estimating the delay between onset and diagnosis of type 2 diabetes from the time course of retinopathy prevalence[J]. Diabetes Care, 2014, 37 (6): 1668- 1674.
doi: 10.2337/dc13-2101 |
| 10 |
Gillies CL , Lambert PC , Abrams KR , et al. Different strategies for screening and prevention of type 2 diabetes in adults: cost effectiveness analysis[J]. BMJ, 2008, 336 (7654): 1180- 1185.
doi: 10.1136/bmj.39545.585289.25 |
| 11 |
Quan J , Li TK , Pang H , et al. Diabetes incidence and prevalence in Hong Kong, China during 2006-2014[J]. Diabetic Medicine, 2017, 34 (7): 902- 908.
doi: 10.1111/dme.13284 |
| 12 |
Bao Y , Ma X , Li H , et al. Glycated haemoglobin A1c for diagnosing diabetes in Chinese population: cross sectional epidemiological survey[J]. BMJ, 2010, 340, c2249.
doi: 10.1136/bmj.c2249 |
| 13 |
Stratton IM , Adler AI , Neil HA , et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study[J]. BMJ, 2000, 321 (7258): 405- 412.
doi: 10.1136/bmj.321.7258.405 |
| 14 |
Zhang Y , Sun J , Pang Z , et al. The impact of new screen-detected and previously known type 2 diabetes on health-related quality of life: A population-based study in Qingdao, China[J]. Qual Life Res, 2014, 23 (8): 2319- 2326.
doi: 10.1007/s11136-014-0674-z |
| 15 |
Zhang Y , Wu J , Chen Y , et al. EQ-5D-3L decrements by diabetes complications and comorbidities in China[J]. Diabetes Ther, 2020, 11 (4): 939- 950.
doi: 10.1007/s13300-020-00788-z |
| 16 |
Pan CW , Sun HP , Zhou HJ , et al. Valuing health-related quality of life in type 2 diabetes patients in China[J]. Med Decis Making, 2016, 36 (2): 234- 241.
doi: 10.1177/0272989X15606903 |
| 17 |
Feldman AL , Griffin SJ , Fharm E , et al. Screening for type 2 diabetes: Do screen-detected cases fare better[J]. Diabetologia, 2017, 60 (11): 2200- 2209.
doi: 10.1007/s00125-017-4402-4 |
| 18 |
Simmons RK , Echouffo-Tcheugui JB , Sharp SJ , et al. Screening for type 2 diabetes and population mortality over 10 years (ADDITION-Cambridge): A cluster-randomised controlled trial[J]. Lancet, 2012, 380 (9855): 1741- 1748.
doi: 10.1016/S0140-6736(12)61422-6 |
| 19 |
Kahn R , Alperin P , Eddy D , et al. Age at initiation and frequency of screening to detect type 2 diabetes: A cost-effectiveness analysis[J]. Lancet, 2010, 375 (9723): 1365- 1374.
doi: 10.1016/S0140-6736(09)62162-0 |
| 20 |
Chung S , Azar KMJ , Baek M , et al. Reconsidering the age thresholds for type Ⅱ diabetes screening in the U.S.[J]. Am J Prev Med, 2014, 47 (4): 375- 381.
doi: 10.1016/j.amepre.2014.05.012 |
| 21 |
Wang Y , Zhao L , Gao L , et al. Health policy and public health implications of obesity in China[J]. Lancet Diabetes Endocrinol, 2021, 9 (7): 446- 461.
doi: 10.1016/S2213-8587(21)00118-2 |
| 22 |
Hoerger TJ , Hicks KA , Sorensen SW , et al. Cost-effectiveness of screening for pre-diabetes among overweight and obese U.S. adults[J]. Diabetes Care, 2007, 30 (11): 2874- 2879.
doi: 10.2337/dc07-0885 |
| [1] | 杨明佳, 吴姜雪, 王静, 刘扬, 李忠民, 李静静, 李宏田, 周玉博, 刘建蒙. 2019—2024年以行政辖区小学生人群为基础的近视情况调查[J]. 北京大学学报(医学版), 2026, 58(3): 513-519. |
| [2] | 陆梦溪, 王炳翰, 康佳丽, 刘秋萍, 周逸帆, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 生物学年龄在社区人群队列中预测心血管病风险的应用[J]. 北京大学学报(医学版), 2026, 58(3): 543-550. |
| [3] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [4] | 袁思妍, 闵鹤葳, 陈平, 吴一波, 崔红霞, 张旭熙, 孙昕霙. 基于大五人格特质的2型糖尿病患者健康教育偏好[J]. 北京大学学报(医学版), 2026, 58(3): 600-605. |
| [5] | 闵鹤葳, 吴一波, 史宇晖, 李明子, 孙昕霙. 基于健康行动过程取向模型分析2型糖尿病患者膳食模式及血糖控制的影响因素[J]. 北京大学学报(医学版), 2025, 57(6): 1145-1152. |
| [6] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [7] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [8] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [9] | 陈子砚, 张晓悦, 顾亦梧, 常春. 2型糖尿病患者使用E-health管理疾病意愿与影响机制[J]. 北京大学学报(医学版), 2025, 57(3): 522-528. |
| [10] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [11] | 张培恒, 高莹, 吴红花, 张健, 张俊清. 暴发性1型糖尿病合并急性胰腺炎1例及文献回顾[J]. 北京大学学报(医学版), 2024, 56(5): 923-927. |
| [12] | 周恬静,刘秋萍,张明露,刘晓非,康佳丽,沈鹏,林鸿波,唐迅,高培. 基于马尔科夫模型的社区人群启动降压药物治疗预防心血管病的策略比较[J]. 北京大学学报(医学版), 2024, 56(3): 441-447. |
| [13] | 马雨佳,卢燃藜,周泽宸,李晓怡,闫泽玉,武轶群,陈大方. 基于两样本孟德尔随机化的失眠与2型糖尿病关联研究[J]. 北京大学学报(医学版), 2024, 56(1): 174-178. |
| [14] | 鲍雷,蔡夏夏,张明远,任磊磊. 维生素D3对2型糖尿病小鼠轻度认知障碍的改善作用及机制研究[J]. 北京大学学报(医学版), 2023, 55(4): 587-592. |
| [15] | 张晓悦,林雨欣,蒋莹,张蓝超,董芒艳,池海谊,董浩宇,马利军,李智婧,常春. 自我效能在2型糖尿病患者自我管理能力和自我管理行为间的中介效应[J]. 北京大学学报(医学版), 2023, 55(3): 450-455. |
|
||
