北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (3): 541-547. doi: 10.19723/j.issn.1671-167X.2022.03.021
儿童坏死性肺炎临床特征及危险因素分析
钱婧1,魏友加1,程毅菁2,张奕1,彭博1,朱春梅1,*( )
)
- 1. 首都儿科研究所附属儿童医院呼吸内科,国家临床重点专科,北京 100020
2. 首都儿科研究所大数据中心,北京 100020
Analysis of clinical features and risk factors of necrotizing pneumonia in children
Jing QIAN1,You-jia WEI1,Yi-jing CHENG2,Yi ZHANG1,Bo PENG1,Chun-mei ZHU1,*()
- 1. Department of Respiratory Medicine, Children's Hospital Affiliated to Capital Institute of Pediatrics, National Key Clinical Specialty, Beijing 100020, China
2. Big Data Center of Capital Institute of Pediatrics, Beijing 100020, China
摘要:
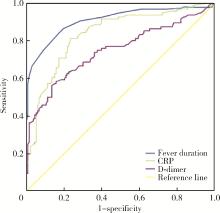
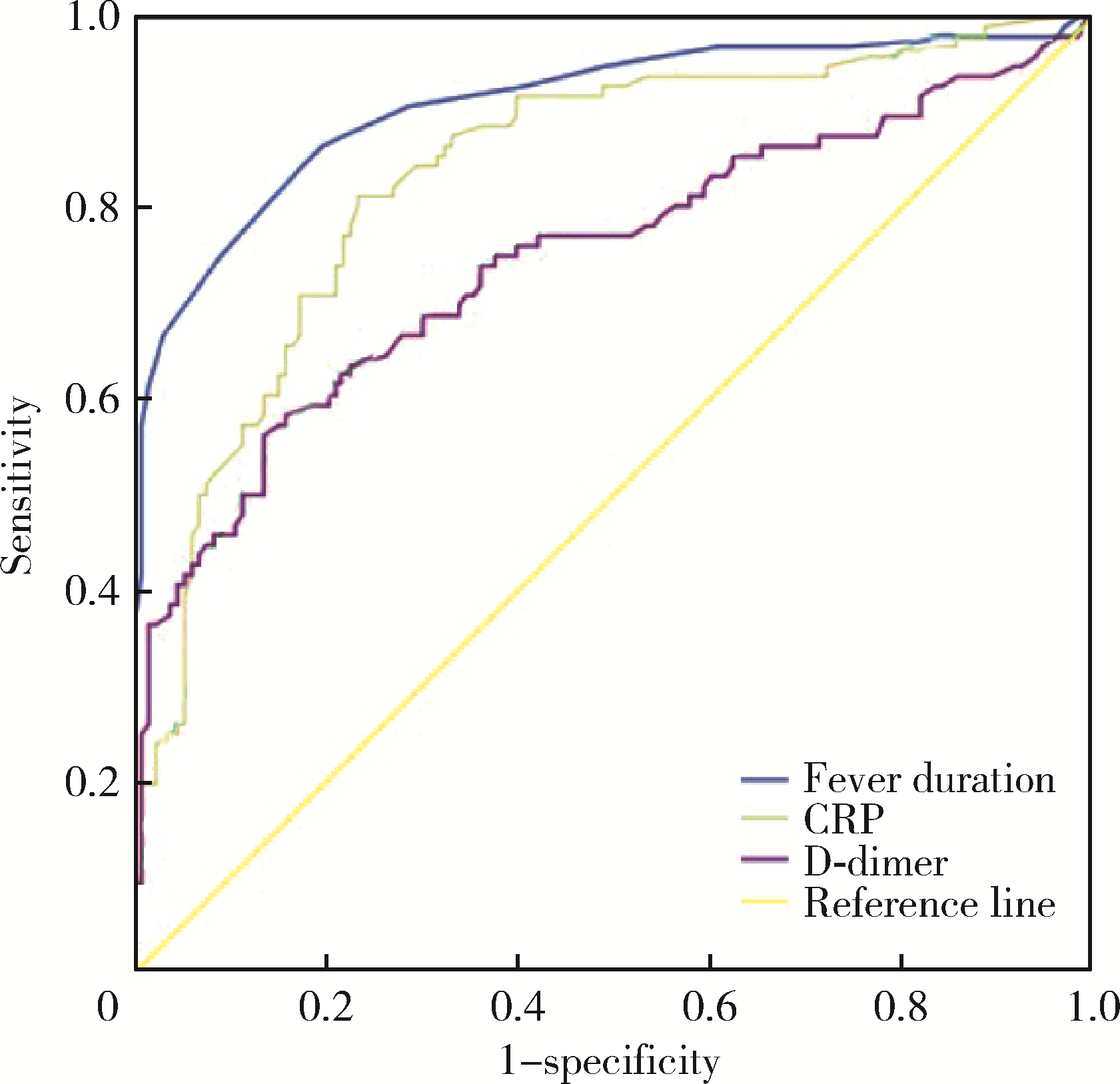
目的: 探讨儿童坏死性肺炎的临床特点及危险因素。方法: 回顾性分析2016年1月至2020年1月在首都儿科研究所附属儿童医院呼吸科住院的218例重症肺炎患儿的病例资料,根据是否发生肺坏死将患儿分为坏死性肺炎(necrotizing pneumonia, NP)组(96例)和非坏死性肺炎(non-necrotizing pneumonia, NNP)组(122例),比较两组临床特征(营养不良、热程、住院时间、影像学表现、治疗及转归随访情况)、实验室检查[白细胞、中性粒细胞比例、血小板计数(platelet,PLT)、C-反应蛋白(C-reactive protein,CRP)、降钙素原(procalcitonin,PCT)、D-二聚体(D-dimer)、乳酸脱氢酶(lactate dehydrogenase,LDH)]和支气管镜下表现的差异,对坏死性肺炎相关临床危险因素进行Logistic回归分析,进一步通过受试者工作特征(receiver operating characteristic, ROC)曲线确定各指标最大诊断价值的临界值。结果: 两组患儿在年龄、性别、病原学分类、支气管镜下表现的差异无统计学意义(P>0.05),NP组患儿的影像学吸收时间长于NNP组(P < 0.05)。两组患儿营养不良、热程、住院时间、白细胞计数、中性粒细胞比例、CRP、PCT、D-dimer等指标的差异有统计学意义(P < 0.05)。6岁以下患儿的影像学吸收时间短于6岁以上者,病程10 d内进行支气管肺泡灌洗治疗的患儿影像学吸收时间短于病程10 d以上者,混合感染组的影像学吸收时间明显长于单一病原感染组。对两组病例进行Logistic回归分析发现,热程、住院时间、CRP、PCT、D-dimer是继发肺坏死的危险因素(分别为P < 0.001、P < 0.001、P < 0.001、P=0.013、P=0.001)。绘制热程、CRP、PCT、D-dimer的ROC曲线,发现当热程>11.5 d、CRP>48.35 mg/L、D-dimer>4.25 mg/L时,对于预测肺坏死的发生有一定诊断价值[ROC曲线下面积(area under ROC curve, AUC)分别为0.909、0.836、0.747,P均 < 0.001]。结论: 儿童坏死性肺炎的热程、住院时间长,混合病原感染的影像学吸收时间明显长于单一病原感染;与6岁以上组患儿及病程>10 d组患儿相比,6岁以下以及病程10 d内的患儿行电子支气管镜肺泡灌洗的疗效更具优势;炎症指标CRP、PCT、D-dimer明显升高,热程、CRP、PCT、D-dimer是重症肺炎继发肺坏死的危险因素,热程>11.5 d、CRP>48.35 mg/L、D-dimer>4.25 mg/L对诊断坏死性肺炎有较高预测价值。
中图分类号:
- R725.6
| 1 |
Masters IB , Isles AF , Grimwood K . Necrotizing pneumonia: An emerging problem in children?[J]. Pneumonia (Nathan), 2017, 9, 11.
doi: 10.1186/s41479-017-0035-0 |
| 2 | Krenke K , Sanocki M , Urbankowska E , et al. Necrotizing pneumonia and its complications in children[J]. Adv Exp Med Biol, 2015, 857, 9- 17. |
| 3 |
Krutikov M , Rahman A , Tiberi S . Necrotizing pneumonia (aetiology, clinical features and management)[J]. Curr Opin Pulm Med, 2019, 25 (3): 225- 232.
doi: 10.1097/MCP.0000000000000571 |
| 4 | 戴菱蔓. 儿童坏死性肺炎的研究进展[J]. 国际儿科学杂志, 2021, 48 (3): 163- 167. |
| 5 |
Wang RS , Wang SY , Hsieh KS , et al. Necrotizing pneumonitis caused by Mycoplasma pneumoniae in pediatric patients: Report of five cases and review of literature[J]. Pediatr Infect Dis J, 2004, 23 (6): 564- 567.
doi: 10.1097/01.inf.0000130074.56368.4b |
| 6 | 宾松涛, 胡晓琴, 王继, 等. 儿童肺炎支原体坏死性肺炎30例临床分析[J]. 疑难病杂志, 2021, 20 (2): 144- 147. |
| 7 | 刘杰. 儿童坏死性肺炎临床特点分析[D]. 天津: 天津医科大学, 2020. |
| 8 |
杨男, 尚云晓. 儿童肺炎链球菌感染致坏死性肺炎的临床特点及预测指标研究[J]. 中华实用儿科临床杂志, 2020, 35 (8): 573- 577.
doi: 10.3760/cma.j.cn101070-20191015-00990 |
| 9 | 张园园, 戴菱蔓, 周云连, 等. 儿童细菌性坏死性肺炎与肺炎支原体坏死性肺炎临床特征及预后比较[J]. 中华儿科杂志, 2019, 57 (8): 625- 630. |
| 10 | 张天骄, 刘盈盈, 裴亮. 儿童肺炎支原体肺炎并发坏死性肺炎的临床预测因素[J]. 中国医科大学学报, 2022, 51 (1): 79- 82. |
| 11 |
杨男, 陈宁, 尚云晓. 儿童坏死性肺炎49例临床分析[J]. 中华实用儿科临床杂志, 2017, 32 (4): 280- 283.
doi: 10.3760/cma.j.issn.2095-428X.2017.04.010 |
| 12 | 刘帅帅, 马静, 张忠晓, 等. 增强CT对儿童坏死性肺炎的诊断价值[J]. 中华实用儿科临床杂志, 2021, 36 (4): 267- 270. |
| 13 | 曾洪武, 黄文献, 陈杰华, 等. 儿童坏死性肺炎的临床特点及胸部HRCT特征[J]. 放射学实践, 2018, 33 (7): 758- 761. |
| 14 | 杜雪平, 郭燕军. 儿童坏死性肺炎的临床特点及胸部CT特征[J]. 影像研究与医学应用, 2020, 4 (10): 68- 69. |
| 15 | Wang X , Zhong LJ , Chen ZM , et a1 . Necrotizing pneumonia caused by refractory Mycoplasma pneumonia pneumonia in children[J]. World J Pediatr, 2018, 14 (4): 344- 349. |
| 16 | 王敏敏. 儿童坏死性肺炎诊治进展[J]. 国际儿科学杂志, 2021, 48 (8): 529- 533. |
| 17 | 席少婷, 蔡栩栩. 儿童难治性肺炎支原体肺炎诊治进展[J]. 国际儿科学杂志, 2020, 47 (6): 384- 388. |
| 18 | Takigawa Y , Fujiwara K , Saito T , et al. Rapidly progressive multiple cavity formation in necrotizing pneumonia caused by community-acquired methicillin-resistant Staphylococcus aureus positive for the Panton-Valentine leucocidin gene[J]. Intern Med, 2019, 58 (5): 685- 691. |
| 19 | 王晓丽, 郑兴厂, 管栋, 等. 胸部CT及可弯曲支气管镜在坏死性肺炎的应用价值[J]. 中国小儿急救医学, 2020, 27 (11): 830- 833. |
| 20 | 陈鲁闽, 王程毅, 宋朝敏, 等. 重症肺炎患儿凝血指标与危重症评分的相关性分析[J]. 中国小儿急救医学, 2013, 20 (4): 380- 382. |
| 21 | Graw-Panzer KD , Verma S , Rao S , et al. Venous thrombosis and pulmonary embolism in a child with pneumonia due to Mycoplasma pneumoniae[J]. J Natl Med Assoc, 2009, 101 (9): 956- 958. |
| 22 | 刘金荣, 徐保平, 李惠民, 等. 肺炎链球菌坏死性肺炎20例诊治分析[J]. 中华儿科杂志, 2012, 50 (6): 431- 434. |
| 23 | 贺艺璇, 张春峰, 吴润晖, 等. D-二聚体在肺炎支原体肺炎患儿病情及预后判断中的应用[J]. 中华实用儿科临床杂志, 2019, 34 (22): 1702- 1706. |
| 24 | 刘帅帅, 马静, 张忠晓, 等. 儿童肺炎支原体坏死性肺炎的早期预测指标[J]. 中华实用儿科临床杂志, 2021, 36 (8): 601- 604. |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [3] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [4] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [5] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [6] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [7] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [8] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [9] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [10] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [11] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [12] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [13] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [14] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [15] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
|
||
