北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (2): 403-407. doi: 10.19723/j.issn.1671-167X.2025.02.030
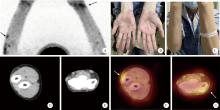
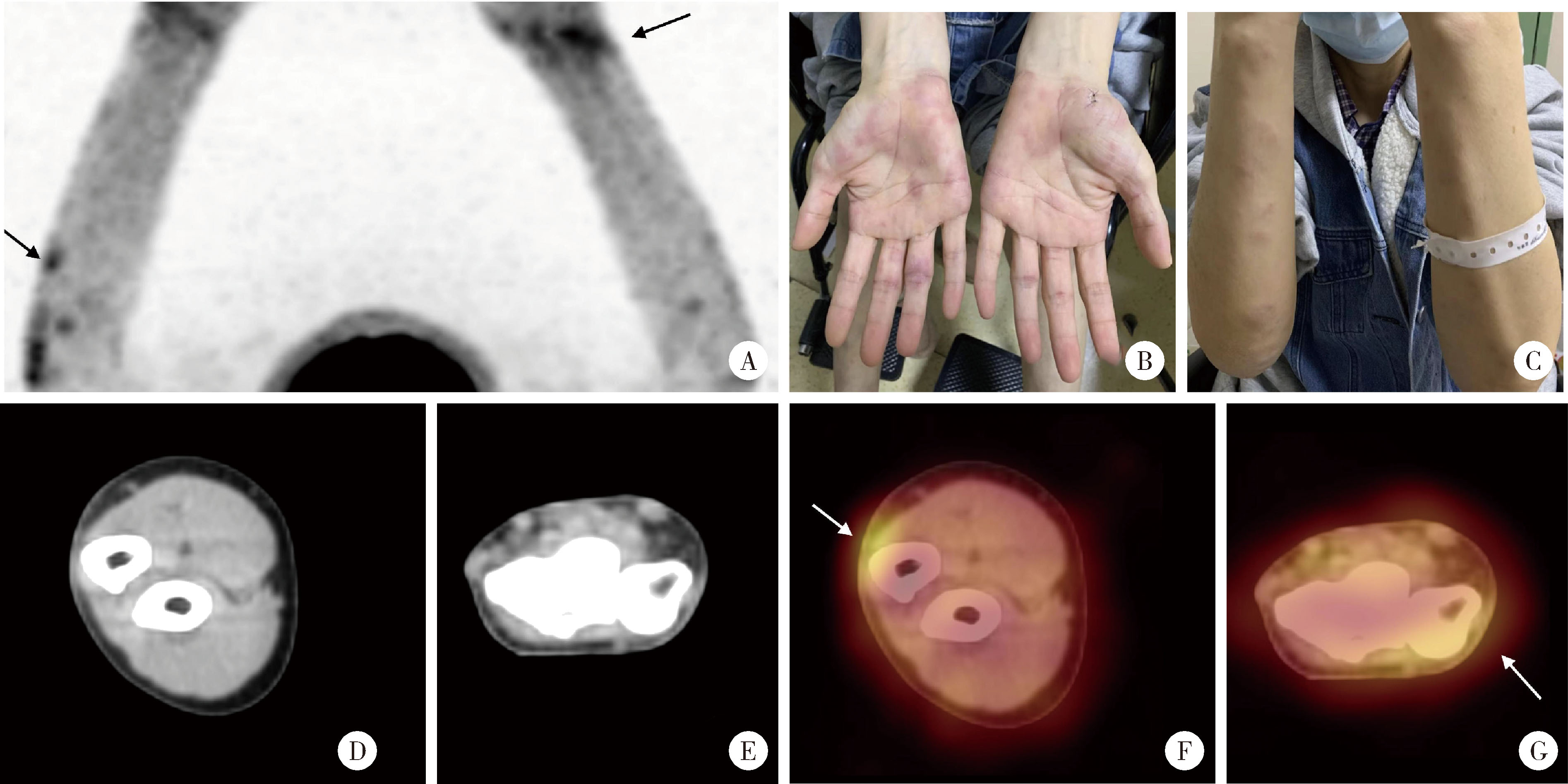
经典型Sweet综合征 18F-FDG PET/CT多脏器异常显像1例
陈钊, 邱永康, 康磊△( )
)
- 北京大学第一医院核医学科,北京 100034
Classical Sweet syndrome with multiple organ lesions by 18F-FDG PET/CT: A case report
Zhao CHEN, Yongkang QIU, Lei KANG△()
- Department of Nuclear Medicine, Peking University First Hospital, Beijing 100034, China
中图分类号:
- R814.42

| 1 |
Raza S , Shahzad RS , Patel AA , et al. Insight into Sweet's syndrome and associated-malignancy: A review of the current literature[J]. Int J Oncol, 2013, 42 (5): 1516- 1522.
doi: 10.3892/ijo.2013.1874 |
| 2 | Ytting H , Vind I , Bang D , et al. Sweet's syndrome: An extra-intestinal manifestation in inflammatory bowel disease[J]. Digestion, 2005, 72 (2/3): 195- 200. |
| 3 |
Von D . Sweet's syndrome (acute febrile neutrophilic dermatosis)[J]. J Am Acad Dermatol, 1994, 31 (4): 535- 536.
doi: 10.1016/S0190-9622(94)70215-2 |
| 4 | Cohen PR . Sweet's syndrome: A comprehensive review of an acute febrile neutrophilic dermatosis[J]. Orphanet J Rare Dis, 2007, 34 (1): 1750- 1772. |
| 5 |
Neoh CY , Tan A , Ng SK . Sweet's syndrome: A spectrum of unusual clinical presentations and associations[J]. Br J Dermatol, 2007, 156 (3): 480- 485.
doi: 10.1111/j.1365-2133.2006.07677.x |
| 6 |
Hou TY , Chang DM , Gao HW , et al. Sweet's syndrome as an initial presentation in systemic lupus erythematosus: A case report and review of the literature[J]. Lupus, 2005, 14 (5): 399- 402.
doi: 10.1191/0961203305lu2083cr |
| 7 |
Schadt CR , Callen JP . Management of neutrophilic dermatoses[J]. Dermatol Ther, 2012, 25 (2): 158- 172.
doi: 10.1111/j.1529-8019.2012.01488.x |
| 8 |
Aydemir H , Oztoprak N , Celebi G , et al. Pulmonary and central nervous system involvement in Sweet's syndrome: A very rare case report[J]. Intern Med, 2008, 47 (16): 1481- 1484.
doi: 10.2169/internalmedicine.47.1115 |
| 9 | Ravaglia C , Poletti G , Gurioli C , et al. Sweet's syndrome asso-ciated with myelogenous leukemia and pulmonary involvement[J]. Monaldi Arch Chest Dis, 2011, 75 (2): 149- 150. |
| 10 |
Marie I , Boyer A , Heron F , et al. Focal aseptic osteitis under-lying neutrophilic dermatosis[J]. Br J Dermatol, 1998, 139 (4): 744- 745.
doi: 10.1046/j.1365-2133.1998.02482.x |
| 11 |
Li B , Ma Z , Xu X , et al. Multi-organ involvement of Sweet's syndrome: A case report and literature review[J]. Intern Med, 2015, 54 (3): 339- 343.
doi: 10.2169/internalmedicine.54.2755 |
| 12 |
Evans AV , Sabroe RA , Setterfield J , et al. Erythema elevatum diutinum/Sweet's syndrome overlap with gastrointestinal and oral involvement[J]. Br J Dermatol, 1999, 141 (4): 766- 767.
doi: 10.1046/j.1365-2133.1999.03140.x |
| 13 |
Notani K , Kobayashi S , Kondoh K , et al. A case of Sweet's syndrome (acute febrile neutrophilic dermatosis) with palatal ulceration[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2000, 89 (4): 477- 479.
doi: 10.1016/S1079-2104(00)70128-4 |
| 14 |
Rosen MJ , Dhawan A , Saeed SA . Inflammatory bowel disease in children and adolescents[J]. Jama Pediatr, 2015, 169 (11): 1053- 1060.
doi: 10.1001/jamapediatrics.2015.1982 |
| 15 | Beckers C , Ribbens C , Andre B , et al. Assessment of disease activity in rheumatoid arthritis with 18F-FDG PET[J]. J Nucl Med, 2004, 45 (6): 956- 964. |
| 16 |
Gontier E , Fourme E , Wartski M , et al. High and typical 18F-FDG bowel uptake in patients treated with metformin[J]. Eur J Nucl Med Mol Imaging, 2008, 35 (1): 95- 99.
doi: 10.1007/s00259-007-0563-6 |
| 17 | Nielsen I , Donati D , Strumia R , et al. Sweet's syndrome and malignancy: Report of the first case associated with adenocarcinoma of the lung[J]. Lung Cancer, 1993, 10 (1/2): 95- 99. |
| 18 |
Cohen PR , Kurzrock R . Sweet's syndrome and malignancy[J]. Am J Med, 1987, 82 (6): 1220- 1226.
doi: 10.1016/0002-9343(87)90229-4 |
| 19 | Liu D , Seiter K , Mathews T , et al. Sweet's syndrome with CML cell infiltration of the skin in a patient with chronic-phase CML while taking imatinib mesylate[J]. Leuk Res, 2004, 28 (Suppl 1): S61- S63. |
| 20 |
White JM , Mufti GJ , Salisbury JR , et al. Cutaneous manifestations of granulocyte colony-stimulating factor[J]. Clin Exp Dermatol, 2006, 31 (2): 206- 207.
doi: 10.1111/j.1365-2230.2005.01996.x |
| 21 |
Titulaer MJ , Soffietti R , Dalmau J , et al. Screening for tumours in paraneoplastic syndromes: Report of an EFNS task force[J]. Eur J Neurol, 2011, 18 (1): 19- e3.
doi: 10.1111/j.1468-1331.2010.03220.x |
| [1] | 马豆豆, 马晓彩, 常天静, 王丽芳, 丁艳, 石连杰. 临床表现似系统性红斑狼疮的大B细胞淋巴瘤骨髓受累1例[J]. 北京大学学报(医学版), 2026, 58(3): 666-669. |
| [2] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [3] | 王月, 梁宇红. 繁茂型牙骨质-骨结构不良1例[J]. 北京大学学报(医学版), 2026, 58(1): 220-224. |
| [4] | 池彦廷, 蒋鸿杰, 陈艳, 徐志秀, 李斌斌. 直接免疫荧光在口腔黏膜寻常型天疱疮诊断中的价值: 基于多指标联合分析的回顾性研究[J]. 北京大学学报(医学版), 2026, 58(1): 68-73. |
| [5] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [6] | 肖晓笛, 夏有辰, 柳剑英, 付鹏. 左侧胸锁乳突肌间血管内乳头状内皮增生1例[J]. 北京大学学报(医学版), 2025, 57(5): 1002-1004. |
| [7] | 孙翔宇, 袁超, 周芯竹, 刁婧, 郑树国. 唾液微生态在口腔及全身疾病早期防治中的应用[J]. 北京大学学报(医学版), 2025, 57(5): 859-863. |
| [8] | 方媛媛, 徐帆, 雷杰, 张昊, 张文宇, 孙宇, 吴宏新, 傅开元, 毛伟玉. 基于颞下颌关节紊乱病诊断标准的临床自动诊断系统的建立及验证[J]. 北京大学学报(医学版), 2025, 57(1): 192-201. |
| [9] | 车佳璐, 刘子臣, 李琨, 张晨, 车南颖. 全自动EasyNAT核酸快速检测系统检测石蜡包埋组织诊断结核病的临床价值[J]. 北京大学学报(医学版), 2024, 56(6): 1047-1051. |
| [10] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [11] | 钟华, 李原, 徐丽玲, 白明欣, 苏茵. 18F-FDG PET/CT在风湿免疫病中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 853-859. |
| [12] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
| [13] | 姚海红,杨帆,唐素玫,张霞,何菁,贾园. 系统性红斑狼疮及成人Still病合并巨噬细胞活化综合征的临床特点及诊断指标[J]. 北京大学学报(医学版), 2023, 55(6): 966-974. |
| [14] | 熊焰,李鑫,梁丽,李东,鄢丽敏,李雪迎,邸吉廷,李挺. 甲状腺粗针穿刺活检病理诊断的准确性评估[J]. 北京大学学报(医学版), 2023, 55(2): 234-242. |
| [15] | 哈雪梅,姚永正,孙莉华,辛春杨,熊焰. 实性肺胎盘样变形1例及文献复习[J]. 北京大学学报(医学版), 2023, 55(2): 357-361. |
|
||
