北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (6): 1128-1133. doi: 10.19723/j.issn.1671-167X.2022.06.012
不同分类标准对中国大动脉炎的诊断效能比较
曹瑞洁1,2,姚中强1,焦朋清2,崔立刚3,*( )
)
- 1. 北京大学第三医院风湿免疫科,北京 100191
2. 河北医科大学第四医院免疫风湿科,石家庄 050011
3. 北京大学第三医院超声医学科,北京 100191
Comparison of diagnostic efficacy of different classification criteria for Takayasu arteritis in Chinese patients
Rui-jie CAO1,2,Zhong-qiang YAO1,Peng-qing JIAO2,Li-gang CUI3,*()
- 1. Department of Rheumatology, Peking University Third Hospital, Beijing 100191, China
2. Department of Rheumato-logy, The Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China
3. Department of Ultrasound Medicine, Peking University Third Hospital, Beijing 100191, China
摘要:
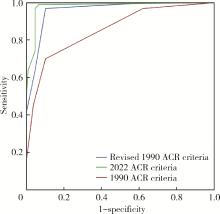
目的: 比较1990年和2022年美国风湿病学会(American College of Rheumatology,ACR)大动脉炎分类标准在中国人群中的诊断效能。方法: 回顾性分析2012年5月至2022年5月就诊于北京大学第三医院且病例资料完善的大动脉炎患者及动脉粥样硬化所致动脉狭窄或闭塞患者的临床资料和影像学检查。以2位风湿免疫科专科医师的诊断为金标准,比较以上两种分类标准的敏感性、特异性、阳性预测值、阴性预测值、准确度及受试者工作特征曲线(receiver operating characteristics,ROC)的曲线下面积(area under ROC curve,AUC)。此外,还尝试将新的影像学方法,如彩色多普勒超声(color Doppler ultrasound,CDUS)、计算机断层血管造影(computed tomography angiography,CTA)、磁共振血管造影(magnetic resonance angiography,MRA)和18F-氟脱氧葡萄糖(18F-fluorodeoxyglucose,18F-FDG)正电子发射断层扫描(positron emission tomography,PET)/计算机断层扫描显像(computed tomography,CT)加入1990年分类标准的影像学检查中,以了解影像学方法的改进对该分类标准诊断效能的影响,并比较大动脉炎和动脉粥样硬化患者影像学表现的差异。结果: 2022年ACR大动脉炎分类标准在灵敏度(91.75%)、阳性预测值(94.68%)、阴性预测值(92.79%)、准确度(93.66%)和AUC(0.979)方面均优于1990年ACR大动脉炎分类标准(45.36%、91.67%、66.24%、72.20%、0.855)。将CDUS、CTA、MRA和PET/CT纳入1990年ACR大动脉炎分类标准的影像学检查后,其灵敏度、阳性预测值、阴性预测值、准确度和AUC均有大幅提高,分别为63.92%、92.54%、74.64%、80.49%和0.959,但仍低于2022年ACR大动脉炎分类标准(P < 0.001)。大动脉炎组影像学表现为动脉狭窄者更多(P=0.030),动脉粥样硬化组动脉闭塞更多(P=0.021),动脉瘤形成或动脉夹层在两组间差异无统计学意义(P=0.171)。大动脉炎组受累血管数量≥3者更多(P=0.013),而动脉粥样硬化组单一血管受累者更多(P=0.011)。结论: 与1990年ACR大动脉炎分类标准相比,2022年的ACR分类标准诊断效能更高,可能更适合中国人群;纳入更多成像方式可以提高1990年ACR分类标准的诊断效能。
中图分类号:
- R593.2

| 1 |
Numano F , Okawara M , Inomata H , et al. Takayasu's arteritis[J]. Lancet, 2000, 356 (9234): 1023- 1025.
doi: 10.1016/S0140-6736(00)02701-X |
| 2 |
Vanoli M , Daina E , Salvarani C , et al. Takayasu's arteritis: A study of 104 Italian patients[J]. Arthritis Rheum, 2005, 53 (1): 100- 107.
doi: 10.1002/art.20922 |
| 3 |
David S , Mathieu V , Patrice C . Medium- and large-vessel vascu-litis[J]. Circulation, 2021, 143 (3): 267- 282.
doi: 10.1161/CIRCULATIONAHA.120.046657 |
| 4 |
Richards BL , March L , Gabriel SE . Epidemiology of large-vessel vasculidities[J]. Best Pract Res Clin Rheumatol, 2010, 24 (6): 871- 883.
doi: 10.1016/j.berh.2010.10.008 |
| 5 |
Cong XL , Dai SM , FENG X , et al. Takayasu's arteritis: Clinical features and outcomes of 125 patients in china[J]. Clin Rheumatol, 2010, 29 (9): 973- 981.
doi: 10.1007/s10067-010-1496-1 |
| 6 |
Kaymaz-Tahra S , Alibaz-Oner F , Direskeneli H . Assessment of damage in Takayasu's arteritis[J]. Semin Arthritis Rheum, 2020, 50 (4): 586- 591.
doi: 10.1016/j.semarthrit.2020.04.003 |
| 7 | 马斌, 牛林, 汪国生, 等. 80例大动脉炎临床资料回顾性分析[J]. 安徽医学, 2014, 35 (1): 71- 74. |
| 8 |
de Souza AW , de Carvalho JF . Diagnostic and classification criteria of Takayasu arteritis[J]. J Autoimmuny, 2014, 48/49, 79- 83.
doi: 10.1016/j.jaut.2014.01.012 |
| 9 |
Seeliger B , Sznajd J , Robson JC , et al. Are the 1990 American College of Rheumatology vasculitis classification criteria still valid?[J]. Rheumatology (Oxford), 2017, 56 (7): 1154- 1161.
doi: 10.1093/rheumatology/kex075 |
| 10 | Arend WP , Michel BA , Bloch DA , et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis[J]. Arthritis Rheum, 1990, 33 (8): 1129- 1134. |
| 11 |
Sugiyama K , Ijiri S , Tagawa S , et al. Takayasu disease on the centenary of its discovery[J]. Jpn J Ophthalmol, 2009, 53 (2): 81- 91.
doi: 10.1007/s10384-009-0650-2 |
| 12 |
Alibaz-Öner F , Aydın SZ , Direskeneli H . Recent advances in Takayasu's arteritis[J]. Eur J Rheumatol, 2015, 2 (1): 24- 30.
doi: 10.5152/eurjrheumatol.2015.0060 |
| 13 |
Kim ESH , Beckman J . Takayasu arteritis: Challenges in diagnosis and management[J]. Heart, 2018, 104 (7): 558- 565.
doi: 10.1136/heartjnl-2016-310848 |
| 14 |
Clifford AH , Cohen Tervaert JW . Cardiovascular events and the role of accelerated atherosclerosis in systemic vasculitis[J]. Atherosclerosis, 2021, 325, 8- 15.
doi: 10.1016/j.atherosclerosis.2021.03.032 |
| 15 |
Moriya J . Critical roles of inflammation in atherosclerosis[J]. J Cardiol, 2019, 73 (1): 22- 27.
doi: 10.1016/j.jjcc.2018.05.010 |
| 16 |
吴思凡, 马莉莉, 陈慧勇, 等. 不同诊断/分类标准对大动脉炎诊断的价值研究[J]. 中华风湿病学杂志, 2021, 25 (11): 727- 732.
doi: 10.3760/cma.j.cn141217-20200426-00175 |
| 17 | Sharma BK , Jain S , Suri S , et al. Diagnostic criteria for Takayasu arteritis[J]. Int J Cardiol, 1996, 54 (Suppl 2): S141- S147. |
| 18 |
Dejaco C , Ramiro S , Duftner C , et al. Eular recommendations for the use of imaging in large vessel vasculitis in clinical practice[J]. Ann Rheum Dis, 2018, 77 (5): 636- 643.
doi: 10.1136/annrheumdis-2017-212649 |
| 19 |
Sinha D , Mondal S , Nag A , et al. Development of a colour doppler ultrasound scoring system in patients of Takayasu's arteritis and its correlation with clinical activity score (ITAS 2010)[J]. Rheumatology (Oxford), 2013, 52 (12): 2196- 2202.
doi: 10.1093/rheumatology/ket289 |
| 20 |
Svensson C , Eriksson P , Zachrisson H . Vascular ultrasound for monitoring of inflammatory activity in Takayasu arteritis[J]. Clin Physiol Funct Imaging, 2020, 40 (1): 37- 45.
doi: 10.1111/cpf.12601 |
| 21 |
Oura K , Yamaguchi Oura M , Itabashi R , et al. Vascular imaging techniques to diagnose and monitor patients with Takayasu arteritis: A review of the literature[J]. Diagnostics (Basel), 2021, 11 (11): 1993.
doi: 10.3390/diagnostics11111993 |
| 22 |
Keser G , Aksu K , Direskeneli H . Takayasu arteritis: An update[J]. Turk J Med Sci, 2018, 48 (4): 681- 697.
doi: 10.3906/sag-1804-136 |
| [1] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [2] | 钟华, 李原, 徐丽玲, 白明欣, 苏茵. 18F-FDG PET/CT在风湿免疫病中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 853-859. |
| [3] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
| [4] | 靖婷,江华,李婷,申倩倩,叶兰,曾银丹,梁文欣,冯罡,司徒文佑,张玉梅. 中国西部5城市中老年人血清25羟基维生素D与握力的相关性[J]. 北京大学学报(医学版), 2024, 56(3): 448-455. |
| [5] | 王清波,傅虹桥. 中国卫生筹资转型的主要特征与历史沿革[J]. 北京大学学报(医学版), 2024, 56(3): 462-470. |
| [6] | 姚海红,杨帆,唐素玫,张霞,何菁,贾园. 系统性红斑狼疮及成人Still病合并巨噬细胞活化综合征的临床特点及诊断指标[J]. 北京大学学报(医学版), 2023, 55(6): 966-974. |
| [7] | 闫晓晋,刘云飞,马宁,党佳佳,张京舒,钟盼亮,胡佩瑾,宋逸,马军. 《中国儿童发展纲要(2011-2020年)》实施期间中小学生营养不良率变化及其政策效应分析[J]. 北京大学学报(医学版), 2023, 55(4): 593-599. |
| [8] | 王婷,李乔晟,刘皓冉,简伟研. 人格特征、城乡差异与抑郁症状变化的关系[J]. 北京大学学报(医学版), 2023, 55(3): 385-391. |
| [9] | 邓佳慧,黄筱琳,刘晓星,孙杰,陆林. 中国睡眠医学的过去、现在和未来[J]. 北京大学学报(医学版), 2023, 55(3): 567-封三. |
| [10] | 熊焰,李鑫,梁丽,李东,鄢丽敏,李雪迎,邸吉廷,李挺. 甲状腺粗针穿刺活检病理诊断的准确性评估[J]. 北京大学学报(医学版), 2023, 55(2): 234-242. |
| [11] | 哈雪梅,姚永正,孙莉华,辛春杨,熊焰. 实性肺胎盘样变形1例及文献复习[J]. 北京大学学报(医学版), 2023, 55(2): 357-361. |
| [12] | 宁博涵,张青霞,杨慧,董颖. 伴间质细胞增生、玻璃样变性及索状结构的子宫内膜样腺癌1例[J]. 北京大学学报(医学版), 2023, 55(2): 366-369. |
| [13] | 陈适,刘田. 重视系统性血管炎的早期识别和个体化治疗[J]. 北京大学学报(医学版), 2022, 54(6): 1065-1067. |
| [14] | 徐朝焰,林长艺,叶达梅,吴培埕,宋明辉,刘有添,邓琼,黄雪艳,范忠晓,游雪兰. 感染性关节炎诊断分析[J]. 北京大学学报(医学版), 2022, 54(6): 1234-1237. |
| [15] | 梁喆,范芳芳,张岩,秦献辉,李建平,霍勇. 中国高血压人群中H型高血压的比率和特征及与美国人群的比较[J]. 北京大学学报(医学版), 2022, 54(5): 1028-1037. |
|
||
