Journal of Peking University (Health Sciences) ›› 2020, Vol. 52 ›› Issue (4): 667-671. doi: 10.19723/j.issn.1671-167X.2020.04.013
Previous Articles Next Articles
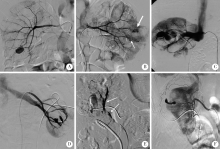
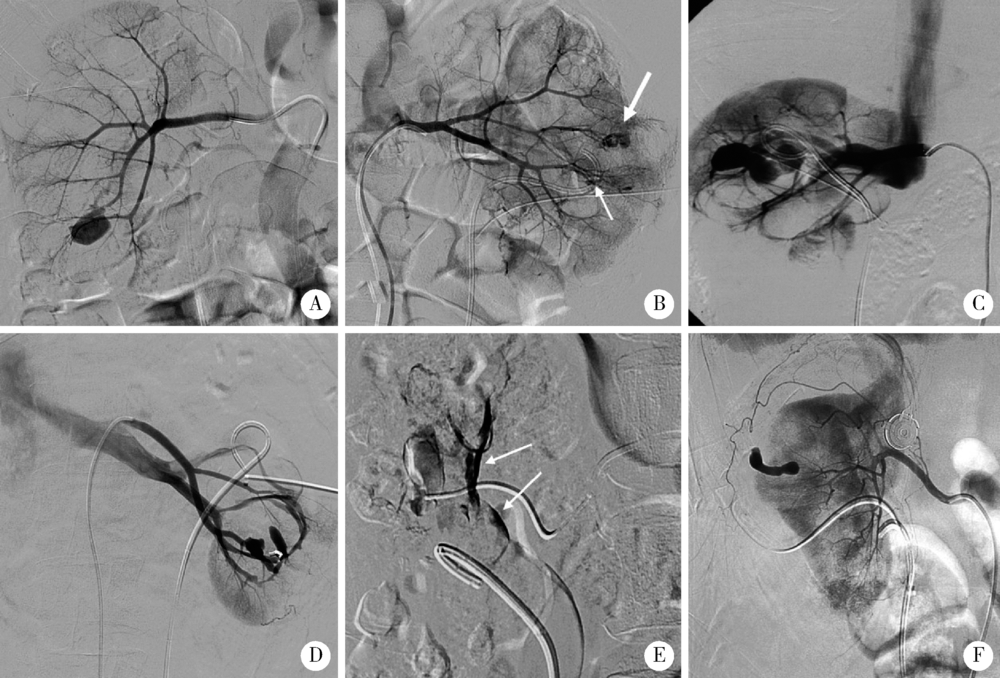
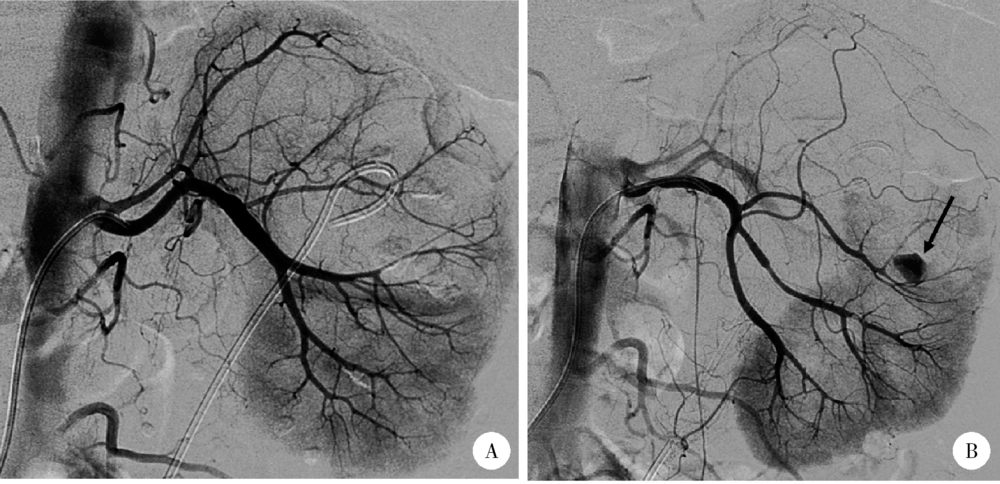
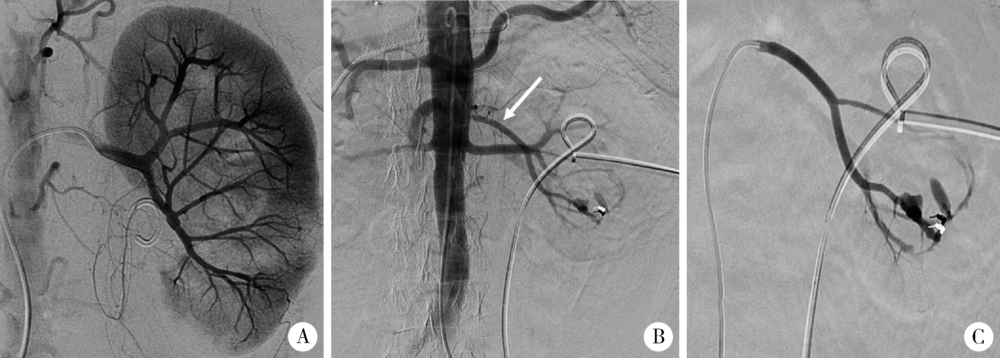
Interventional treatment of hemorrhage after percutaneous nephrolithotomy
Jian GAO1,△( ),Li-bao HU1,Chen CHEN1,Xin ZHI1,Tao XU2,△()
),Li-bao HU1,Chen CHEN1,Xin ZHI1,Tao XU2,△()
- 1. Department of Radiology, Peking University People’s Hospital, Beijing 100044, China
2. Department of Urology, Peking University People’s Hospital, Beijing 100044, China
CLC Number:
- R814.47





| [1] | Un S, Cakir V, Kara C, et al. Risk factors for hemorrhage requiring embolization after percutaneous nephrolithotomy[J]. Can Urol Assoc J, 2015,9(9/10):594-598. |
| [2] | El Tayeb MM, Knoedler JJ, Krambeck AE, et al. Vascular complications after percutaneous nephrolithotomy: 10 years of expe-rience[J]. Urology, 2015,85(4):777-781. |
| [3] | El-Nahas AR, Shokeir AA, Mohsen T, et al. Functional and morphological effects of postpercutaneous nephrolithotomy superselective renal angiographic embolization[J]. Urology, 2008,71(3):408-412. |
| [4] | Kervancioglu S, Gelebek Yilmaz F, Erturhan S. Endovascular management of vascular complications after percutaneous nephrolithotomy[J]. Vasa, 2014,43(6):459-464. |
| [5] | Li L, Zhang Y, Chen Y, et al. A multicentre retrospective study of transcatheter angiographic embolization in the treatment of delayed haemorrhage after percutaneous nephrolithotomy[J]. Eur Radiol, 2015,25(4):1140-1147. |
| [6] | Wang HL, Xu CY, Wang HH, et al. Emergency transcatheter arterial embolization for acute renal hemorrhage[J]. Medicine, 2015,94(42):e1667. |
| [7] | Choi MJ, Kim PH, Shin JH, et al. Angiographic management of percutaneous renal procedure-related bleeding: A single-center experience[J]. Int J Urol, 2019,26(3):406-412. |
| [8] |
El-Nahas AR, Shokeir AA, El-Assmy AM, et al. Postpercuta-neous nephrolithotomy extensive hemorrhage: A study of risk factors[J]. J Urol, 2007,177(2):576-579.
pmid: 17222636 |
| [9] | 任医民, 伍筱梅, 温宇, 等. 经皮肾镜取石术后肾出血栓塞失败的原因分析[J]. 中华医学杂志, 2017,97(1):22-25. |
| [10] |
He ZH, Lei HQ, Lu XB, et al. Analysis of repeated renal arte-riography after percutaneous nephrolithotomy[J]. Urolithiasis, 2017,45(5):495-499.
pmid: 27837249 |
| [11] | Ding XB, Guan JJ, Tian JY, et al. Subcostal artery bleeding after percutaneous nephrolithotomy: A case report and literature review[J]. J Int Med Res, 2018,46(10):4350-4353. |
| [12] | Seetharama MK, Ananthashayana VH, Shivanand G, et al. Interventional radiology in the management of visceral artery pseudo-aneurysms: A review of techniques and embolic materials[J]. Korean J Radiol, 2016,17(3):351-363. |
| [13] | Ganpule AP, Shah DH, Desai MR. Postpercutaneous nephrolithotomy bleeding: Aetiology and management[J]. Curr Opin Urol, 2014,24(2):189-194. |
| [14] | 熊六林, 黄晓波, 叶雄俊, 等. 经皮肾镜术后肾脏严重出血特点及选择性介入栓塞的时机选择(附13例报告)[J]. 北京大学学报(医学版), 2010,42(4):465-468. |
| [1] | Xiaolin WANG, Shaoyi GUO, Dazhao CHEN, Xijie WEN, Yong HUA, Liang ZHANG, Qin ZHANG. A follow-up study on total hip arthroplasty in patients with systemic lupus erythematosus combined with osteonecrosis of femoral head [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1081-1088. |
| [2] | Chao ZUO, Guoli WANG, Kunlin YANG, Xinyan CHE, Yisen MENG, Kai ZHANG. Comparison of efficacy and safety of transurethral thulium fiber laser enucleation of prostate in patients with different prostate volumes [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 711-716. |
| [3] | Zhao ZHAO, Weiyu ZHANG, Wenbo YANG, Yongjie ZHANG, Xiaopeng ZHANG, Huiying ZHAO, Gang ZHOU, Qiang WANG. Kidney transplantation in low-age, low-weight children: A report of two cases [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 803-807. |
| [4] | Wanyin HOU,Jie DONG. Acquired cystic kidney hemorrhage in peritoneal dialysis patients: A report of three cases [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 546-550. |
| [5] | Kewei CHEN,Shaohui DENG,Zhuo LIU,Hongxian ZHANG,Lulin MA,Shudong ZHANG. Discussion on the surgical timing of rupture and hemorrhage of renal angiomyolipoma [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 326-331. |
| [6] | Min FENG,Zhe CHEN,Yong-jing CHENG. A case of duodenal ulcer as prominent manifestation of IgG4-related disease [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1125-1129. |
| [7] | Dong LAN,Zhuo LIU,Yu-xuan LI,Guo-liang WANG,Xiao-jun TIAN,Lu-lin MA,Shu-dong ZHANG,Hong-xian ZHANG. Risk factors for massive hemorrhage after radical nephrectomy and removal of venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 825-832. |
| [8] | Su-huan XU,Bei-bei WANG,Qiu-ying PANG,Li-jun ZHONG,Yan-ming DING,Yan-bo HUANG,Xin-yan CHE. Effect of equal temperature bladder irrigation in patients with transurethral resection of prostate: A meta-analysis [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 676-683. |
| [9] | Yun-peng CUI,Xue-dong SHI,Jia LIU,Chuan MI,Bing WANG,Yuan-xing PAN,Yun-fei LIN. Percutaneous pedicle screw fixation combined expandable tubular retractor in the treatment of spinal metastases [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 530-536. |
| [10] | Hui LI,Yang-xu GAO,Shu-lei WANG,Hong-xin YAO. Surgical complications of totally implantable venous access port in children with malignant tumors [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1167-1171. |
| [11] | YUAN Chang-wei,WANG Ying-jin,ZHANG Shu-jie,SHEN Sheng-li,DUAN Hong-zhou. Clinical outcomes following microsurgery and endovascular embolization in the management of spinal dural arteriovenous fistula: A meta-analysis study [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 304-314. |
| [12] | LI Wei-hao,LI Wei,ZHANG Xue-min,LI Qing-le,JIAO Yang,ZHANG Tao,JIANG Jing-jun,ZHANG Xiao-ming. Comparison of the outcomes between open and hybrid approaches in the treatment of thoracoabdominal aortic aneurysms repair [J]. Journal of Peking University (Health Sciences), 2022, 54(1): 177-181. |
| [13] | DAI Xiang,ZUO Mei-ni,ZHANG Xiao-peng,HU Hao,XU Tao. Comparison of long-term outcomes in different managements of diverticular neck in percutaneous nephrolithotomy for diverticular calculi [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 704-709. |
| [14] | ZHANG Lei,LI Guo-liang,DANG Zong-hui, ,A yong,WU Ling-jie,LIU Li-jun. Analysis of bleeding risk in percutaneous renal biopsy in Tibet [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 298-301. |
| [15] | Wen-min DONG,Ming-rui WANG,Hao HU,Qi WANG,Ke-xin XU,Tao XU. Initial clinical experience and follow-up outcomes of treatment for ureteroileal anastomotic stricture with Allium coated metal ureteral stent [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 637-641. |
|
||