

特发性炎性肌病(idiopathic inflammatory myo-pathies,IIM)是一组以横纹肌和皮肤慢性炎症为特征的异质性疾病[1],包括皮肌炎、抗合成酶综合征(anti-synthetase antibody syndrome,ASS)、免疫介导坏死性肌病(immune-mediated necrotizing myopathy,IMNM)、包涵体肌炎和多肌炎[2]。IIM发病机制尚不完全清楚,患者机体对自身抗原的异常反应是发病的主要原因之一[3-4]。在血清学方面,抗组氨酰tRNA合成酶(histidyl tRNA synthetase, Jo-1)抗体是ASS最常见的抗体,能在约30%的ASS患者体内测出[5]。既往文献表明,不仅IIM患者抗Jo-1抗体阳性,很多其他结缔组织病(connective tissue disease,CTD)及非CTD患者的血清中也可以检测到该抗体,如类风湿关节炎、系统性红斑狼疮等[6-10],但多为个案报道或针对单一疾病的报道,目前缺乏归纳抗Jo-1抗体疾病谱的系统性大样本研究。
1 资料与方法
1.1 一般资料
纳入2016—2022年于北京大学人民医院检测肌炎谱的患者中所有抗Jo-1抗体阳性患者,记录患者起病的基本信息[起病年龄、性别,初次就诊时血常规、肌酸激酶(creatine kinase,CK)、乳酸脱氢酶(lactate dehydrogenase,LDH)、α-羟丁酸脱羧酶(α-hydroxybutyric dehydrogenase,α-HBD)等]、临床诊断、临床表现以及多种炎症指标、免疫学指标。IIM的诊断符合美国风湿病学会及欧洲抗风湿病学联盟分类标准[15];ASS的诊断符合Solomon标准[16],即抗合成酶抗体阳性同时合并任意2种主要指标或1种主要指标及2种次要指标[主要指标:①排除其他原因的间质性肺病,②符合Bohan和Peter标准的皮肌炎或多肌炎;次要指标:①关节炎,②雷诺现象(Raynaud phenomenon),③技工手];IMNM的诊断符合国际共识[17]。此外,本研究同时纳入45例同期于北京大学人民医院诊断为抗Jo-1抗体阴性的ASS患者[抗异亮氨酰tRNA合成酶(isoleucyl tRNA synthetase,OJ)抗体、抗甘氨酰tRNA合成酶(glycyl tRNA synthetase,EJ)抗体、抗苏氨酰tRNA合成酶(threonyl tRNA synthetase,PL-7)抗体或抗丙氨酸tRNA合成酶(alanine tRNA synthetase,PL-12)抗体阳性]作为对照,对照组ASS患者符合Solomon标准[16]。
在免疫学指标方面,检测了肌炎相关抗体(myositis associated antibodies,MAAs)和肌炎特异性抗体(myositis specific antibodies,MSAs),包括抗核小体重塑-去乙酰化酶复合物组成成分(component of the nucleosome remodeling-deacetylase complex,Mi-2)、抗转录中介因子1γ(transcriptional intermediary factor 1γ,TIF-1γ)、小泛素样修饰激活酶(small ubiquitin like modifier activating enzyme,SAE)、黑色素瘤分化相关基因5(melanoma differentiation associated gene 5,MDA5)、核基质蛋白2(nuclear matrix protein 2,NXP2)、信号识别颗粒(signal recognition particle,SRP)、Ro-52、Ku、PM-Scl、抗PL-7、抗PL-12、抗EJ、抗OJ抗体和抗核抗体(anti-nuclear antibody,ANA)。
在其他实验室检查方面,我们定义C反应蛋白(C-reaction protein,CRP)>10 mg/L为CRP升高,男性红细胞沉降率(erythrocyte sedimentation rate,ESR)>15 mm/h、女性ESR>20 mm/h为ESR升高,CK>165 U/L为CK升高,LDH>245 U/L为LDH升高,α-HBD>182 U/L为α-HBD升高。
1.2 检测方法
抗Jo-1抗体的检测应用免疫印迹法,带有天然Jo-1(利用亲和层析法从小牛和兔胸腺中纯化)的试纸孵育后,用EUROLineScan软件进行判读,+、++、+++分别表示抗体滴度的低、中、高。
1.3 统计学处理
本研究采用SPSS 23.0进行统计学分析。符合正态分布的计量资料用均数±标准差表示,采用t检验进行统计分析;不符合正态分布的计量资料用中位数(25%分位数,75%分位数)表示,采用Wil-coxon秩和检验进行统计分析;分类变量用例数(百分数)表述,使用卡方检验及Fisher’s精确概率检验进行统计分析。在分析临床特征与抗Jo-1抗体滴度相关性时使用Spearman秩相关分析,P < 0.05为差异有统计学意义。
2 结果
2.1 抗Jo-1抗体阳性患者疾病谱
研究纳入165例抗Jo-1抗体阳性患者,包括120例女性和45例男性,平均年龄(48.04±14.24)岁;其中CTD共133例(80.6%),分为IIM及除外IIM的CTD患者:(1)IIM共95例(57.6%),其中ASS 84例(50.9%)、IMNM 7例(4.2%)、皮肌炎4例(2.5%);(2)除外IIM的CTD共38例(23.0%),其中类风湿关节炎11例(6.7%)、未分化结缔组织病5例(3.0%)、具有自身免疫特征的间质性肺炎5例(3.0%)、未分化关节炎4例(2.5%)、干燥综合征3例(1.8%)、系统性红斑狼疮3例(1.8%)、系统性血管炎3例(1.8%)、系统性硬化症2例(1.2%)、抗磷脂综合征1例(0.6%)、风湿性多肌痛1例(0.6%)。此外,未诊断CTD的患者包括恶性肿瘤3例(1.8%,样本中患恶性肿瘤患者共6例,另外3例合并CTD)、感染性疾病4例(2.4%,支原体感染1例、EB病毒感染1例、乙型肝炎1例及未明确病原体感染1例)、骨关节炎2例、免疫性血小板减少性紫癜2例及脊柱关节炎、痛风、多系统萎缩、神经性皮炎、周围神经病和溃疡性结肠炎各1例。有15例(9.1%)患者未明确临床诊断(图 1)。
图1
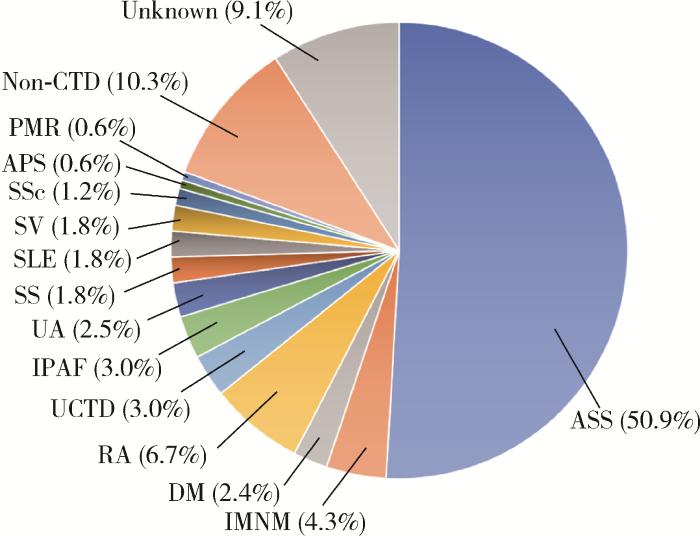
图1
抗Jo-1抗体阳性患者疾病分布
Figure 1
Disease distribution in patients with positive anti-Jo-1 antibody
ASS, anti-synthetase syndrome; IMNM, immune-mediated necrotizing myositis; DM, dermatomyositis; RA, rheumatoid arthritis; UCTD, undifferentiated connective tissue disease; IPAF, interstitial pneumonia with autoimmune features; UA, undifferentiated arthritis; SS, Sjögren's syndrome; SLE, systemic lupus erythematosus; SV, systemic vasculitis; SSc, systemic sclerosis; APS, antiphospholipid syndrome; PMR, polymyalgia rheumatica; Non-CTD, non-connective tissue disease.
2.2 抗Jo-1抗体阳性和阴性ASS患者比较
本研究纳入的抗Jo-1抗体阳性及阴性的ASS患者分别为84例和45例,后者包括抗PL-7抗体阳性15例、抗PL-12抗体阳性14例、抗EJ抗体阳性15例、抗OJ抗体阳性3例。将抗Jo-1抗体阳性及阴性的ASS患者进行比较发现,抗Jo-1抗体阳性的ASS患者的起病年龄更低(49.9岁vs. 55.0岁,P=0.026),更多表现为关节炎(60.7% vs. 33.3%,P=0.002)和肌痛(47.1% vs. 22.2%,P=0.004),抗Jo-1抗体阴性的ASS患者ESR升高的比例显著高于阳性患者(50.0% vs. 71.1%,P=0.010,表 1)。
表1 抗Jo-1抗体阳性与阴性ASS患者临床特征及实验室数据对比
Table 1
| Items | Anti-Jo-1 (+) (n=84) | Anti-Jo-1 (-) (n=45) | t/Z/χ2 | P |
| Clinical features | ||||
| Age of onset/years | 49.9±12.8 | 55.0±11.9 | 2.247 | 0.026 |
| Female | 64 (76.2) | 33 (73.3) | 0.128 | 0.720 |
| ILD | 72 (85.7) | 43 (95.6) | 2.933 | 0.087 |
| Arthritis | 51 (60.7) | 15 (33.3) | 8.792 | 0.003 |
| Myalgia | 40 (47.1) | 10 (22.2) | 7.962 | 0.005 |
| Myasthenia | 45 (53.6) | 21 (46.7) | 0.559 | 0.455 |
| Dysphagia | 5 (6.0) | 6 (13.3) | 2.047 | 0.153 |
| Mechanic hands | 45 (53.6) | 23 (51.1) | 0.071 | 0.790 |
| Gottron sign | 68 (81.0) | 39 (86.7) | 0.676 | 0.411 |
| Raynaud phenomenon | 11 (13.1) | 8 (17.8) | 0.842 | 0.474 |
| Neurologic abnormality | 4 (4.8) | 0 | 0.297a | |
| Malignancy | 2 (2.4) | 1 (2.2) | >0.999a | |
| Laboratory data | ||||
| ANA+ | 44 (52.4) | 29 (64.4) | 1.736 | 0.188 |
| Anti-Ro-52 (+) | 63 (75.0) | 36 (80.0) | 0.410 | 0.522 |
| Anti-PM-Scl 75/100 (+) | 5 (6.0) | 0 | 0.156a | |
| Anti-Mi-2 (+) | 2 (2.4) | 1 (2.2) | >0.999a | |
| Anti-SAE (+) | 1 (1.2) | 0 | >0.999a | |
| Anti-MDA5 (+) | 1 (1.2) | 0 | >0.999a | |
| Anti-NXP2 (+) | 0 | 0 | ||
| Anti-TIF-1γ (+) | 0 | 1 (2.2) | 0.349a | |
| Anti-SRP (+) | 1 (1.2) | 0 | >0.999a | |
| ESR/(mm/h) | 20.0 (8.0, 44.0) | 32.0 (16.0, 58.0) | -2.067 | 0.039 |
| Elevated ESR | 42 (50.0) | 32 (71.1) | 5.340 | 0.021 |
| CRP/(mg/L) | 4.3 (0.6, 27.0) | 13.2 (1.5, 27.0) | -1.648 | 0.099 |
| Elevated CRP | 51 (60.7) | 24 (53.3) | 0.656 | 0.418 |
| CK/(U/L) | 230.0 (93.0, 1 059.0) | 131.0 (69.0, 413.0) | -1.733 | 0.083 |
| Elevated CK | 46 (54.8) | 19 (42.2) | 1.843 | 0.175 |
Data are expressed as n(%), $\bar x \pm s$ or median (0.25 quantile, 0.75 quantile). a, analyzed by Fisher’s exact test. Elevated ESR: male>15 mm/h, female>20 mm/h; Elevated CRP: CRP>10.0 mg/L; Elevated CK: CK>165 U/L. Anti-Jo-1, anti-histidyl tRNA synthetase antibody; ASS, anti-synthetase syndrome; ILD, interstitial lung disease; ANA, antinuclear antibodies; Mi-2, component of the nucleosome remodeling-deacetylase complex; SAE, small ubiquitin like modifier activating enzyme; MDA5, melanoma differentiation associated gene 5; NXP2, nuclear matrix protein 2; TIF-1γ, transcriptional intermediary factor 1γ; SRP, signal recognition particle. SRP, signal recognition particle; ESR, erythrocyte sedimentation rate; CRP, C-reaction protein; CK, creatine kinase.
2.3 抗Jo-1抗体滴度与临床特点
依据抗Jo-1抗体滴度+、++、+++将患者分为低、中、高三组,其中低滴度组15例(25.0%),中等滴度组15例(38.5%),高滴度组54例(81.8%),图 2展示了抗Jo-1抗体不同滴度组的疾病分布。将抗Jo-1抗体滴度与ASS患者临床特点进行Spearman秩相关分析发现,在临床表现方面,关节炎、技工手、雷诺现象、Gottron征的发生率均随抗体滴度的升高而升高(P < 0.05);在实验室检查方面,随着抗Jo-1抗体滴度升高,患者CK和α-HBD升高的发生率增加(P<0.05,表 2),抗Jo-1抗体滴度低、中、高组的CK值依次为67.0(40.0,284.0) U/L、186.0(83.0,494.0) U/L和414.0(121.0,1 288.5) U/L,α-HBD值依次为247.5(144.3,287.0) U/L、234.0(159.0,293.0) U/L和275(201.5,367.0) U/L。
图2
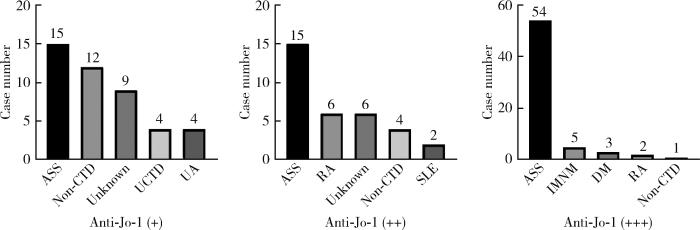
图2
抗Jo-1抗体滴度与疾病分布(前五种)
Figure 2
The top five diseases with high, median and low anti-Jo-1 antibody titer
Abbreviations as in
表2 抗Jo-1抗体滴度与ASS患者临床特征及实验室数据的相关性分析
Table 2
| Items | Anti-Jo-1 (+) (n=15) | Anti-Jo-1 (++) (n=15) | Anti-Jo-1 (+++)(n=54) | r | P |
| Clinical features | |||||
| Fever | 5 (33.3) | 4 (26.7) | 9 (16.7) | -0.163 | 0.140 |
| ILD | 12 (80.0) | 13 (86.7) | 47 (87.0) | 0.062 | 0.576 |
| Arthritis | 4 (26.7) | 7 (46.7) | 40 (74.1) | 0.385 | < 0.001 |
| Myalgia | 6 (40.0) | 11 (73.3) | 24 (44.4) | -0.071 | 0.521 |
| Myasthenia | 6 (40.0) | 8 (53.3) | 32 (59.3) | 0.136 | 0.218 |
| Dysphagia | 0 | 0 | 5 (9.3) | 0.183 | 0.096 |
| Mechanic hands | 4 (26.7) | 8 (53.3) | 33 (61.1) | 0.233 | 0.033 |
| Raynaud phenomenon | 0 | 1 (2.6) | 10 (15.2) | 0.223 | 0.041 |
| Gottron sign | 9 (60.0) | 12 (80.0) | 47 (87.3) | 0.236 | 0.031 |
| Malignancy | 1 (6.7) | 0 | 1 (1.9) | -0.074 | 0.504 |
| Neurologic abnormality | 1 (6.7) | 0 | 3 (5.6) | 0.028 | 0.797 |
| Laboratory data | |||||
| Elevated WBC | 7 (46.7) | 10 (66.7) | 38 (70.4) | 0.162 | 0.141 |
| Decreased lymphocyte | 8 (53.3) | 9 (60.0) | 31 (57.4) | 0.016 | 0.887 |
| Elevated neutrophil | 10 (66.7) | 11 (73.3) | 38 (70.4) | 0.013 | 0.905 |
| Elevated ESR | 7 (46.7) | 4 (26.7) | 31 (57.4) | 0.159 | 0.151 |
| Elevated CRP | 7 (46.7) | 1 (6.7) | 24 (44.4) | 0.087 | 0.445 |
| Decreased albumin | 13 (86.7) | 10 (66.7) | 40 (74.1) | -0.058 | 0.600 |
| Elevated CK | 4 (26.7) | 8 (53.3) | 34 (63.0) | 0.263 | 0.016 |
| Elevated LDH | 13 (86.7) | 10 (66.7) | 43 (79.6) | 0.002 | 0.958 |
| Elevated α-HBD | 10 (66.7) | 9 (60.0) | 47 (87.0) | 0.255 | 0.021 |
Data are expressed as n(%). Elevated WBC: WBC>9.50×109/L; Decreased lymphocyte: Lymphocyte < 1.10×109/L; Elevated neutrophil: Neutrophil>6.3×109/L; Decreased albumin: Albumin < 40 g/L; Elevated LDH: LDH>245 U/L; Elevated α-HBD: α-HBD >182 U/L; WBC, white blood cell; LDH, lactate dehydrogenase; α-HBD, α-hydroxybutyric dehydrogenase. Other abbreviations and explanations as in
2.4 单一抗Jo-1抗体阳性与抗Jo-1抗体合并其他MAAs/MSAs阳性ASS患者对比
将抗Jo-1抗体阳性ASS患者分为单一抗Jo-1抗体阳性组(20例)和抗Jo-1抗体合并其他MAAs/MSAs阳性组(64例),两组比较发现,单一抗Jo-1抗体阳性组表现出肌痛(25.0% vs. 56.3%,P=0.015)、肌无力(35.0% vs. 61.0%,P=0.042)的比例显著低于抗Jo-1抗体合并其他MAAs/MSAs阳性组,其他临床表现及实验室指标两组间差异无统计学意义(表 3)。
表3 单一抗Jo-1抗体与抗Jo-1抗体合并其他MAAs/MSAs阳性ASS患者临床特征及实验室数据对比
Table 3
| Items | Isolated anti-Jo-1 (+) (n=20) | Coexistence of anti-Jo-1 (+) and MAAs/MSAs (+) (n=64) | t/Z/χ2 | P |
| Clinical features | ||||
| Age of onset/years | 45.60±10.15 | 49.94±13.60 | -0.102 | 0.919 |
| Female | 15 (75.0) | 49 (76.6) | < 0.001 | >0.999 |
| Fever | 5 (25.0) | 13 (20.3) | 0.018 | 0.894 |
| Myalgia | 5 (25.0) | 36 (56.3) | 5.956 | 0.015 |
| Myasthenia | 7 (35.0) | 39 (61.0) | 4.138 | 0.042 |
| Dysphagia | 0 | 5 (7.8) | 0.332a | |
| Gottron sign | 15 (75.0) | 53 (82.8) | 0.203 | 0.652 |
| Raynaud phenomenon | 2 (10.0) | 9 (14.1) | 0.008 | 0.928 |
| ILD | 17 (85.0) | 55 (85.9) | < 0.001 | >0.999 |
| Mechanic hands | 9 (45.0) | 36 (56.3) | 0.775 | 0.379 |
| Arthritis | 11 (55.0) | 40 (62.5) | 0.359 | 0.549 |
| Neurologic abnormality | 1 (5.0) | 3 (4.7) | >0.999a | |
| Malignancy | 1 (5.0) | 1 (1.6) | 0.422a | |
| Laboratory data | ||||
| ESR/(mm/h) | 15.5 (7.5, 31.5) | 22.0 (8.0, 56.0) | -1.076 | 0.282 |
| Elevated ESR | 9 (45.0) | 33 (51.6) | 0.331 | 0.565 |
| CRP/(mg/L) | 7.1 (0.5, 12.4) | 4.3 (0.6, 32.2) | -0.952 | 0.341 |
| Elevated CRP | 8 (40.0) | 24 (37.5) | 0.046 | 0.836 |
| CK/(U/L) | 155.0 (80.0, 756.0) | 237.0 (100.0, 1153.0) | -0.799 | 0.425 |
| Elevated CK | 10 (50.0) | 36 (56.3) | 0.313 | 0.576 |
Data are expressed as n(%), $\bar x \pm s$ or median (0.25 quantile, 0.75 quantile). a, analyzed by Fisher’s exact test. MAAs, myositis associated antibodies; MSAs, myositis specific antibodies. Other abbreviations and explanations as in
此外,在95例IIM患者中,抗Jo-1抗体与其他三种MAAs同时存在的情况见图 3,其中单一抗Jo-1抗体阳性者占13.7%,抗Jo-1抗体同时合并Ro-52抗体和ANA阳性患者最多见,占总体的42.1%。
图3
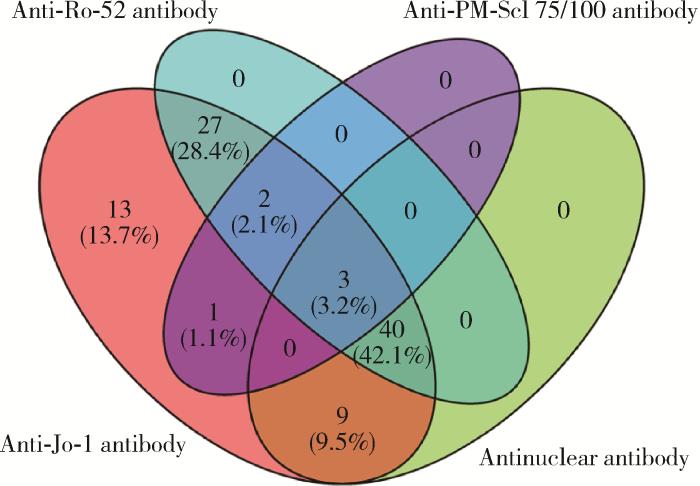
图3
IIM患者中抗Jo-1抗体与抗Ro-52抗体、抗PM-Scl 75/100抗体及抗核抗体合并存在情况
Figure 3
Condition of anti-Jo-1 antibody with anti-Ro-52, anti-PM-Scl 75/100 and ANA in IIM patients
The red part represents the anti-Jo-1 antibody-positive samples, the blue part represents the anti-Ro-52 antibody-positive samples, the purple part represents the anti-PM-Scl 75/100 antibody-positive samples, the green part represents the antinuclear antibody-positive samples, and the overlap part represents the patients with two or more positive antibodies at the same time.
3 讨论
抗Jo-1抗体是肌炎特异性抗体之一,本研究结果显示抗Jo-1抗体阳性患者的疾病多样,有57.6%的患者最终诊断为IIM,50.9%诊断为ASS,除外IIM的CTD患者占23.6%。在除外IIM的CTD中,类风湿关节炎是最多的诊断,以往研究显示,ASS在疾病早期往往不会表现出经典的关节炎、肌炎、ILD三联征,可只表现出关节症状,导致部分ASS在早期被诊断为类风湿关节炎,也有部分病例最终被认为是ASS与类风湿关节炎重叠[7],因此,这部分诊断为非肌炎CTD的患者需继续随访观察。本研究有31例患者未被诊断为CTD,Mielnik等[18]的研究表明,部分IIM患者在表现出肌炎相关症状前可以检测到抗Jo-1抗体阳性,因此本研究中部分未被诊断为CTD的患者可能是IIM早期,最终可能分化进展为肌炎。与以往研究[19]相比,本研究诊断IIM的比例较低,推测在未诊断为IIM的患者中有部分未表现出典型症状者可能被遗漏掉,需密切随访观察。
在ASS患者的亚组分析中,抗Jo-1阳性的ASS患者发病年龄更早,更多表现为肌痛和关节炎,而ESR升高的发生率更低。在抗Jo-1抗体阴性的ASS亚组中,其他抗合成酶抗体(抗EJ、OJ、PL-7、PL-12抗体)的阳性率相应更高,Ge等[20]的研究提示,抗OJ抗体阳性ASS患者ESR高于抗Jo-1抗体阳性ASS患者,这与本研究抗Jo-1阳性ASS患者ESR升高比例低于阴性组的结果相一致。既往研究表明,抗Jo-1抗体阳性与技工手、ILD、肌炎、关节炎、雷诺现象等症状有关[21],在Aggarwal等[19]的研究结果中,抗Jo-1抗体阴性ASS患者组与阳性组相比起病年龄更晚,常无典型肌炎表现,更多表现出ILD、肺动脉高压等肺部受累表现,而肺部受累患者普遍预后差、死亡率高。本研究结果在起病年龄和肌肉受累方面与既往结果类似,与抗Jo-1抗体阳性ASS患者相比,抗Jo-1抗体阴性ASS患者的ILD比例更高,但未发现统计学意义,尚需加大样本量进一步探究。
本组84例抗Jo-1抗体阳性的ASS患者中,随着抗Jo-1抗体滴度的升高,关节炎、技工手、Gottron征、雷诺现象更加多见,且CK及α-HBD异常的比例升高。Liu等[22]的研究表明,抗Jo-1抗体阳性患者多存在白细胞、ESR、CRP、CK、LDH等指标水平的升高,Zhao等[23]的研究提示,血清抗Jo-1抗体水平与疾病活动度相关,本研究发现大量结缔组织受累表现和肌肉损害相关指标与抗Jo-1抗体的抗体滴度相关,表明抗Jo-1抗体可能介导机体某些炎症反应及肌肉组织损伤,后续研究可以就抗Jo-1抗体水平能否作为预测患者疾病活动和预后的指标进行探究。本研究发现随着抗Jo-1抗体滴度升高,诊断为ASS的比例也随之升高,由前可知随着抗Jo-1抗体的升高,Gottron征、技工手、关节炎及肌炎相关指标升高的发生率更高,因此,我们认为高滴度的抗Jo-1抗体可能对ASS更有诊断价值。
恶性肿瘤是IIM较为常见的合并症,以往研究表明,抗合成酶抗体是IIM合并恶性肿瘤的保护因素[27],这与本研究的结果相一致,但本研究中仅2例ASS患者合并肿瘤,其临床指导意义较小,抗Jo-1抗体与恶性肿瘤的关系以及作用机制尚需更深入地探究。
本研究存在一定的局限性:首先,本研究为单中心横断面回顾性研究,有待扩大样本进行随访;其次,本研究所用检测抗Jo-1抗体的方法为免疫印记法,为非定量检测,期待其他检测方法应用于临床以进一步验证。
综上所述,抗Jo-1抗体阳性患者疾病谱广,以ASS为主;抗Jo-1抗体阳性ASS患者相较于阴性患者起病更早,更易累及肌肉和关节,抗Jo-1抗体阴性ASS患者更易出现ESR升高;随着抗Jo-1抗体滴度升高,ASS患者累及结缔组织的临床表现和肌肉损伤指标异常情况发生率升高,总体疾病活动度更高,病情更加严重;抗Jo-1抗体可与MAAs/MSAs同时存在,在合并其他肌炎抗体阳性时,ASS患者更多表现出肌痛、肌无力,疾病表现更重。
参考文献
Classification of idiopathic inflammatory myopathies: Pathology perspectives
[J].DOI:10.1097/WCO.0000000000000740 [本文引用: 1]
Anti-Jo 1 autoantibodies, from clinic to the bench
[J].DOI:10.1002/rai2.12035 [本文引用: 1]
Clinical usefulness of autoantibodies in idiopathic inflammatory myositis
[J].
The immune response and the pathogenesis of idiopathic inflammatory myositis: A critical review
[J].DOI:10.1007/s12016-016-8527-x [本文引用: 1]
Clinical features of anti-synthetase syndrome associated interstitial lung disease: A retrospective cohort in China
[J].DOI:10.1186/s12890-021-01399-5 [本文引用: 1]
Rare autoantibodies to cellular antigens in systemic lupus erythematosus
[J].DOI:10.1177/0961203314524850 [本文引用: 1]
Anti-Jo-1 syndrome often misdiagnosed as rheumatoid arthritis (for many years): A single-center experience
[J].DOI:10.1097/RHU.0000000000001234 [本文引用: 1]
Etanercept-induced anti-Jo-1-antibody-positive polymyositis in a patient with rheumatoid arthritis: A case report and review of the literature
[J].
Cytokines in relation to autoantibodies before onset of symptoms for systemic lupus erythematosus
[J].
不同抗氨酰tRNA合成酶抗体阳性的抗合成酶综合征60例临床和影像学相关特征分析
[J].
Serum-circulating His-tRNA synthetase inhibits organ-targeted immune responses
[J].DOI:10.1038/s41423-019-0331-0 [本文引用: 1]
Jo-1 antibodies from myositis induce complement-dependent cytotoxicity and TREM-1 upregulation in muscle endothelial cells
[J].DOI:10.1212/NXI.0000000000200116 [本文引用: 1]
Clinical spectrum time course in anti Jo-1 positive antisynthetase syndrome: Results from an international retrospective multicenter study
[J].DOI:10.1097/MD.0000000000001144 [本文引用: 1]
Clinical spectrum of anti-Jo-1-associated disease
[J].DOI:10.1097/BOR.0000000000000434 [本文引用: 1]
2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups
[J].DOI:10.1136/annrheumdis-2017-211468 [本文引用: 1]
Myositis-related interstitial lung disease and antisynthetase syndrome
[J].DOI:10.1590/S1806-37132011000100015 [本文引用: 2]
224th ENMC international workshop: Clinico-sero-pathological classification of immune-mediated necrotizing myopathies Zandvoort, The Netherlands, 14-16 October 2016
[J].DOI:10.1016/j.nmd.2017.09.016 [本文引用: 1]
Clinical features and prognosis of patients with idiopathic inflammatory myo-pathies and anti-Jo-1 antibodies
[J].DOI:10.1080/08916930600623767 [本文引用: 1]
Patients with non-Jo-1 anti-tRNA-synthetase autoantibodies have worse survival than Jo-1 positive patients
[J].DOI:10.1136/annrheumdis-2012-201800 [本文引用: 2]
Clinical characteristics of anti-isoleucyl-tRNA synthetase antibody associated syndrome and comparison with different patient cohorts
[J].DOI:10.55563/clinexprheumatol/v2rbd0 [本文引用: 1]
A comprehensive overview on myositis-specific antibodies: New and old biomarkers in idiopathic inflammatory myopathy
[J].DOI:10.1007/s12016-015-8510-y [本文引用: 1]
Increased serum matrix metalloproteinase-9 levels are associated with anti-Jo1 but not anti-MDA5 in myositis patients
[J].DOI:10.14336/AD.2018.1120 [本文引用: 1]
Myositis-specific autoantibodies in adults with idiopathic inflammatory myopathy: Correlations with diagnosis and disease activity
[J].DOI:10.1007/s10067-020-05273-3 [本文引用: 1]
Enhanced formation and impaired degradation of neutrophil extracellular traps in dermatomyositis and polymyositis: A potential contributor to interstitial lung disease complications
[J].DOI:10.1111/cei.12319 [本文引用: 1]
Serum levels of B-cell activating factor of the TNF family (BAFF) correlate with anti-Jo-1 autoantibodies levels and disease activity in patients with anti-Jo-1positive polymyositis and dermatomyositis
[J].DOI:10.1186/s13075-018-1650-8 [本文引用: 1]
Critical requirement for professional APCs in eliciting T cell responses to novel fragments of histidyl-tRNA synthetase (Jo-1) in Jo-1 antibody-positive polymyositis
[J].DOI:10.4049/jimmunol.169.12.7127 [本文引用: 1]
A systematic review and meta-analysis to inform cancer screening guidelines in idiopathic inflammatory myopathies
[J].DOI:10.1093/rheumatology/keab166 [本文引用: 1]
Short-term and long-term outcome of anti-Jo1-positive patients with anti-Ro52 antibody
[J].DOI:10.1016/j.semarthrit.2011.09.008 [本文引用: 1]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}