北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (1): 159-164. doi: 10.19723/j.issn.1671-167X.2019.01.027
脐动脉血气pH值对剖宫产新生儿住院期间并发症的预测价值
包菊1,刘佳2,曲元1,穆东亮1,△( )
)
- 1. 北京大学第一医院 麻醉科,北京 100034
2. 北京大学第一医院 手术室, 北京 100034
Predictive value of umbilical arterial cord pH on complications during hospitalization in neonates after cesarean section
Ju BAO1,Jia LIU2,Yuan QU1,Dong-liang MU1,△()
- 1. Department of Anesthesiology,Peking University First Hospital,Beijing 100034, China
2. Department of Operation Room,Peking University First Hospital,Beijing 100034, China
摘要:
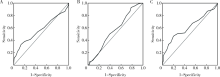
目的:分析脐动脉血气pH值对剖宫产新生儿住院期间并发症的预测价值。方法:本研究为回顾性队列研究,选择2017年1月1日至6月30日在北京大学第一医院剖宫产娩出并完成脐动脉血气分析的新生儿为研究对象,主要观察终点是新生儿住院期间并发症发生率。按照新生儿是否发生住院期间并发症将研究对象分为两组,比较两组间脐动脉血气pH值。收集母婴围产期的资料和新生儿住院期间并发症的资料,采用ROC曲线分析脐动脉血气pH对新生儿住院期间并发症的预测价值。结果:共纳入872例新生儿(择期541例、急诊331例),新生儿住院期间并发症的总体发生率为14.1%,其中发生率最高的3项分别为感染、吸入性肺炎及心肌损伤。无并发症组pH值平均为7.31,有并发症组pH值平均为7.29,组间比较差异有统计学意义(P<0.001)。本研究中pH≤7.20的总体比例为3.1%(27/872),其中无并发症组pH值≤7.20的比例为1.6%(12/749),有并发症组pH值≤7.20的比例为12.2%(15/123),组间比较差异有统计学意义(P<0.001)。多因素Logistic回归分析显示,早产(OR=8.224, 95%CI: 4.910~13.777, P<0.001)、妊娠期高血压(OR=1.886, 95%CI: 1.004~3.546, P=0.049)、宫内生长受限(OR=4.429, 95%CI: 1.280~15.330, P=0.019)、急诊剖宫产(OR=2.711, 95%CI: 1.682~4.369, P<0.001)、脐动脉血气pH值≤7.20(OR=7.420, 95%CI: 2.951~18.655, P<0.001)及5分钟Apgar评分小于10分(OR=11.849, 95%CI: 3.977~35.128, P<0.001)是新生儿发生住院期间并发症的危险因素。脐动脉血气pH值预测全部新生儿、择期新生儿及急诊新生儿住院并发症的ROC曲线下面积分别为0.570(95%CI: 0.508~0.633, P=0.012)、0.559(95%CI: 0.465~0.652, P=0.189)及0.617(95%CI: 0.538~0.697, P=0.002)。结论:脐动脉血气pH值≤7.2与剖宫产新生儿住院并发症发生率增加有相关性,但是ROC分析显示其预测价值较低。
中图分类号:
- R722.1

| [1] |
Yildiz EP, Tatli B, Ekici B , et al. Evaluation of etiologic and prognostic factors in neonatal convulsions[J]. Pediatr Neurol, 2012,47(3):186-192.
doi: 10.1016/j.pediatrneurol.2012.05.015 pmid: 22883283 |
| [2] |
Elmahdy H, El-Mashad AR, EI-Bathrawy H , et al. Human recombinant erythropoietin in asphyxia neonatorum: pilot trial[J]. Pediatrics, 2010,125(5):e1135-e1142.
doi: 10.1542/peds.2009-2268 pmid: 20385632 |
| [3] |
张燕妮, 牟红梅 . 新生儿窒息126例临床分析[J]. 中国妇幼健康研究, 2016,27(11):1370-1372.
doi: 10.3969/j.issn.1673-5293.2016.11.025 |
| [4] |
ACOG Committee on Obstetric Practice. ACOG Committee Opi-nion No. 348, November 2006: Umbilical cord blood gas and acid-base analysis[J]. Obstet Gynecol, 2006,108(5):1319-1322.
doi: 10.1097/00006250-200611000-00058 |
| [5] |
Whitelaw A, Thoresen M . Clinical trials of treatments after perinatal asphyxia[J]. Curr Opin Pediatr, 2002,14(6):664-668.
doi: 10.1097/00008480-200212000-00002 pmid: 12436031 |
| [6] |
Neilson JP . Umbilical cord blood gas analysis[J]. BMJ, 2010(340):c1720.
doi: 10.1016/S0889-8545(05)70107-8 pmid: 20466790 |
| [7] |
Ahmadpour-Kacho M, Asnafi N, Javadian M , et al. Correlation between umbilical cord pH and Apgar score in high-risk pregnancy[J]. Iran J Pediatr, 2010,20(4):401-406.
doi: 10.1007/s13312-010-0170-7 pmid: 23056738 |
| [8] |
White CR, Doherty DA, Henderson JJ , et al. Benefits of introducing universal umbilical cord blood gas and lactate analysis into an obstetric unit[J]. Aust N Z J Obstet Gynaecol, 2010,50(4):318-328.
doi: 10.1111/j.1479-828X.2010.01192.x pmid: 20716258 |
| [9] |
White CR, Doherty DA, Cannon JW , et al. Cost effectiveness of universal umbilical cord blood gas and lactate analysis in a tertiary level maternity unit[J]. J Perinat Med, 2016,44(5):573-584.
doi: 10.1515/jpm-2015-0398 pmid: 26966927 |
| [10] |
Wiklund I, Ahlberg M, Dahlström A , et al. Routine testing of umbilical cord blood after normal delivery should be discontinued[J]. Sex Reprod Healthc, 2014,5(4):165-166.
doi: 10.1016/j.srhc.2014.10.002 pmid: 25433824 |
| [11] |
Kutuk MS, Yikilmaz A, Ozgun MT , et al. Prenatal diagnosis and postnatal outcome of fetal intracranial hemorrhage[J]. Childs Nerv Syst, 2014,30(3):411-418.
doi: 10.1007/s00381-013-2243-0 pmid: 23907139 |
| [12] |
Caffrey Osvald E, Prentice P . NICE clinical guideline:antibiotics for the prevention and treatment of early-onset neonatal infection[J]. Arch Dis Child Educ Pract Ed, 2014,99(3):98-100.
doi: 10.1136/archdischild-2013-304629 pmid: 24334339 |
| [13] |
Mortier I, Blanc J, Tosello B , et al. Is gestational diabetes an independent risk factor of neonatal severe respiratory distress syndrome after 34 weeks of gestation? A prospective study[J]. Arch Gynecol Obstet, 2017,296(6):1071-1077.
doi: 10.1007/s00404-017-4505-7 pmid: 28948345 |
| [14] |
Eaton S . Necrotizing enterocolitis symposium:Epidemiology and early diagnosis[J]. J Pediatr Surg, 2017,52(2):223-225.
doi: 10.1016/j.jpedsurg.2016.11.013 pmid: 27914586 |
| [15] |
Sabol BA, Caughey AB . Acidemia in neonates with a 5-minute Apgar score of 7 or greater. What are the outcomes? [J]. Am J Obstet Gynecol, 2016, 215(4): 486. e1-e6.
doi: 10.1016/S0002-9378(16)30277-0 |
| [16] |
Malin GL, Morris RK, Khan KS . Strength of association between umbilical cord pH and perinatal and long-term outcomes:systema-tic review and meta-analysis[J]. BMJ, 2010(340):c1471.
doi: 10.1097/01.aoa.0000397115.97213.02 pmid: 20466789 |
| [17] |
Zanardo V, Dal Cengio V, Parotto M , et al. Elective caesarean delivery adversely affects preductal oxygen saturation during birth transition[J]. Arch Dis Child Fetal Neonatal Ed, 2016,101(4):F339-F343.
doi: 10.1136/archdischild-2015-308304 pmid: 26644392 |
| [18] |
Yeh P, Emary K, Impey L . The relationship between umbilical cord arterial pH and serious adverse neonatal outcome: analysis of 51 519 consecutive validated samples[J]. BJOG, 2012,119(7):824-831.
doi: 10.1111/j.1471-0528.2012.03335.x pmid: 22571747 |
| [19] |
Cahill AG, Mathur AM, Smyser CD , et al. Neurologic injury in acidemic term infants[J]. Am J Perinatol, 2017,34(7):668-675.
doi: 10.1055/s-0036-1597135 pmid: 27926973 |
| [20] |
Low JA, Lindsay BG, Derrick EJ . Threshold of metabolic acidosis associated with newborn complications[J]. Am J Obstet Gynecol, 1997,177(6):1391-1394.
doi: 10.1016/S0002-9378(97)70080-2 pmid: 9423740 |
| [21] |
中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2015)[J]. 中华产科急救电子杂志, 2015,4(4):206-213.
doi: 10.3760/cma.j.issn.0529-567x.2015.10.001 |
| [22] |
Allen MC, Cristofalo EA, Kim C . Outcomes of preterm infants:morbidity replaces mortality[J]. Clin Perinatol, 2011,38(3):441-454.
doi: 10.1016/j.clp.2011.06.011 pmid: 21890018 |
| [23] |
张春雨, 李蕊, 张大程 , 等. 脐血血气分析在早产儿窒息诊断中的价值及影响因素分析[J]. 中国妇幼保健, 2017,32(5):968-971.
doi: 10.7620/zgfybj.j.issn.1001-4411.2017.05.33 |
| [24] |
Low JA, Killen H, Derrick EJ . Antepartum fetal asphyxia in the preterm pregnancy[J]. Am J Obstet Gynecol, 2003,188(2):461-465.
doi: 10.1067/mob.2003.37 pmid: 12592256 |
| [25] |
Pallotto EK, Kilbride HW . Perinatal outcome and later implications of intrauterine growth restriction[J]. Clin Obstet Gynecol, 2006,46(2):257-269.
doi: 10.1097/00003081-200606000-00008 pmid: 16721105 |
| [26] |
Unterscheider J, O’Donoghue K, Daly S, , et al. Fetal growth restriction and the risk of perinatal mortality-case studies from the multicenter PORTO study[J]. BMC Pregnancy Childbirth, 2014(14):63.
doi: 10.1186/1471-2393-14-63 pmid: 3923738 |
| [27] |
Razaz N, Boyce WT, Brownell M , et al. Five-minute Apgar score as a marker for developmental vulnerability at 5 years of age[J]. Arch Dis Child Fetal Neonatal Ed, 2016,101(2):F114-F120.
doi: 10.1136/archdischild-2015-308458 |
| [28] |
Persson M, Razaz N, Tedroff K , et al. Five and 10 minute Apgar scores and risks of cerebral palsy and epilepsy:population based cohort study in Sweden[J]. BMJ, 2018(360):k207.
doi: 10.1136/bmj.k207 pmid: 29437691 |
| [29] |
徐娜, 马挺, 田肇隆 , 等. 剖宫产术中仰卧位低血压综合征对新生儿脐血血气分析的影响[J]. 首都医科大学学报, 2009,30(3):393-395.
doi: 10.3969/j.issn.1006-7795.2009.03.030 |
| [1] | 左蒙, 张文楼, 陈柏锜, 赵晨, 陈亚红, 何建辉, 郭新彪, 邓芙蓉. 环境温度个体暴露与慢性阻塞性肺疾病患者睡眠期间血氧饱和度的关联[J]. 北京大学学报(医学版), 2026, 58(3): 592-599. |
| [2] | 温倩颖, 张丽卿, 秦安霖, 李小峰. 无症状高尿酸血症患者小肠细菌过度生长及炎症细胞因子表达水平[J]. 北京大学学报(医学版), 2026, 58(2): 313-318. |
| [3] | FarinEbrahimi, 冯志强, FarazEbrahimi, 韩玮华, 于子杨, 贾宽宽, 安金刚. 上颌药物相关性颌骨坏死的不同分期手术治疗效果[J]. 北京大学学报(医学版), 2026, 58(1): 107-114. |
| [4] | 贾晓怡, 张炎, 汤卫红. 粪便钙卫蛋白检测在婴儿牛奶蛋白过敏性肠炎中的诊断价值[J]. 北京大学学报(医学版), 2025, 57(6): 1132-1135. |
| [5] | 董琪, 何菁, 贾园, 姚海红, 张霞. 模拟复发性多软骨炎的VEXAS综合征1例[J]. 北京大学学报(医学版), 2025, 57(6): 1180-1183. |
| [6] | 梁景原, 张霞, 姚海红. 误诊为系统性硬化症的POEMS综合征1例[J]. 北京大学学报(医学版), 2025, 57(6): 1184-1187. |
| [7] | 丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰. 利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1203-1207. |
| [8] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [9] | 黄俊捷, 刘肇瑞, 张婷婷, 黄悦勤. 中国精神卫生调查的跨世纪历程[J]. 北京大学学报(医学版), 2025, 57(5): 868-874. |
| [10] | 杨树涵, 李奕昕, 崔浩亮, 王佑新, 吴玉莹, 王明月, 杨依凡, 恩卡尔·努尔, 杨磊, 王辉. 代谢相关脂肪性肝病及其心脏代谢风险指标异常与不良妊娠结局的相关性[J]. 北京大学学报(医学版), 2025, 57(3): 487-495. |
| [11] | 张烁, 兰勇兵, 孙点剑一, 裴培, 杜怀东, 陈君石, 陈铮鸣, 吕筠, 李立明, 余灿清, (代表中国慢性病前瞻性研究项目协作组). 慢性阻塞性肺疾病患者体力活动与死亡风险的前瞻性关联[J]. 北京大学学报(医学版), 2025, 57(3): 537-544. |
| [12] | 阿娜尔古丽·阿不都肉什提, 宋迎豪, 闫晓晋, 高永康, 刘波, 胡刚. 1990—2021年中国及全球增龄性听力损失的疾病负担与未来趋势预测[J]. 北京大学学报(医学版), 2025, 57(3): 545-553. |
| [13] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
| [14] | 朱玉静, 王磊, 吕成银, 谈文峰, 张缪佳. 抗EJ抗体阳性抗合成酶综合征相关间质性肺疾病复发的临床特征分析[J]. 北京大学学报(医学版), 2024, 56(6): 980-986. |
| [15] | 翟佳羽, 赵金霞, 安卓, 刘蕊. 低疾病活动度的中轴型脊柱关节炎患者残留症状评估及其相关因素分析[J]. 北京大学学报(医学版), 2024, 56(6): 987-993. |
|
||
