北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (3): 586-590. doi: 10.19723/j.issn.1671-167X.2019.03.031
前交叉韧带生物力学止点重建的解剖学与有限元分析
张家豪,任爽,邵嘉艺,牛星跃,胡晓青,敖英芳△( )
)
- 北京大学第三医院运动医学研究所,北京市运动医学关节伤病重点实验室, 北京 100191
Anatomical and finite element analysis of anterior cruciate ligament reconstruction within biomechanical insertion
Jia-hao ZHANG,Shuang REN,Jia-yi SHAO,Xing-yue NIU,Xiao-qing HU,Ying-fang AO△()
- Beijing Key Laboratory of Sports Injuries, Beijing 100191, China
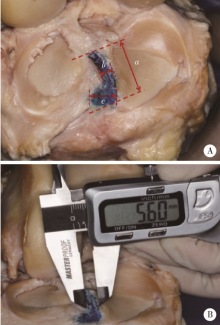
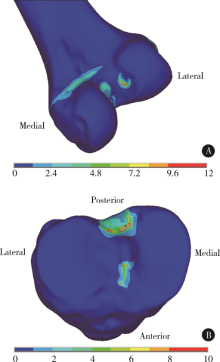
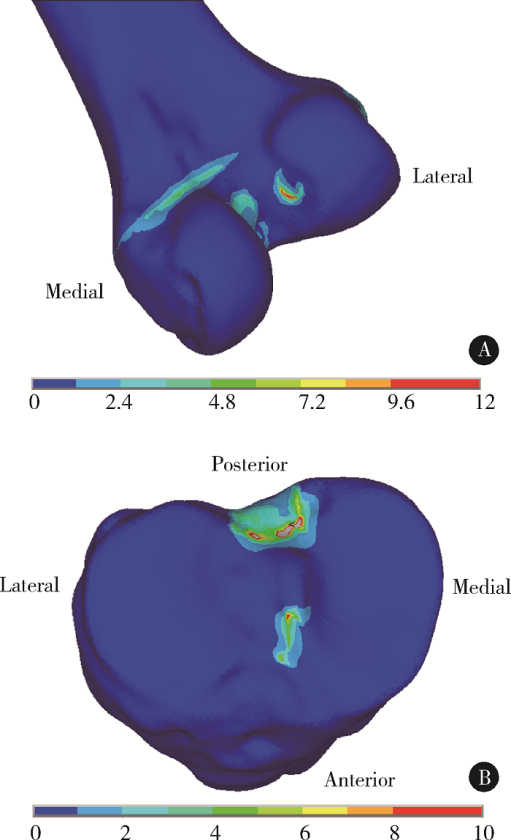
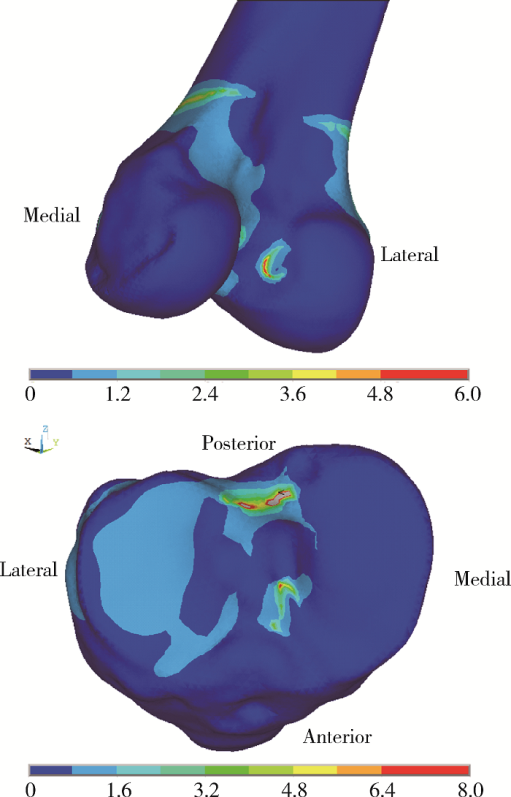
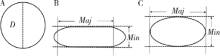
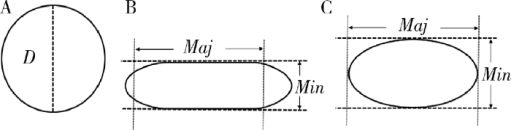
摘要: 目的 解剖研究大体观察膝关节前交叉韧带(anterior cruciate ligament, ACL)胫骨止点的形态,并利用有限元分析软件分析ACL的力学止点分布,为临床ACL重建提供新理念。方法 选取10例新鲜成人膝关节标本,男6例,女4例,采取标准髌旁内侧入路打开关节腔,暴露并解剖剔除ACL,观察并记录ACL胫骨止点形态,测量胫骨止点前后径和左右径。利用三维重建软件MIMICS及有限元分析软件ANSYS建立膝关节模型,模拟临床体格检查Lachman试验和pivot-shift试验,观察ACL在胫骨和股骨端止点的受力分布情况。结果 ACL胫骨致密止点大体观呈扁长的弧形,其前后径为(13.8±2.0) mm,体部左右径为(5.3±0.6) mm,前缘左右径为(11.5±1.2) mm。有限元分析显示,股骨端应力较高区域为住院医师嵴(residents’ ridge)附近一类椭圆形区域,胫骨端应力较高部分延内侧髁间嵴(medial intercondylar ridge)狭长分布,与解剖观察相符,从理论上验证了ACL止点的生物力学分布特点。结论 解剖研究及有限元分析均证实ACL胫骨止点为一扁长的弧形,理想的ACL重建技术应依据其生物力学特点进行重建, 基于解剖学研究和生物力学分析本课题组提出前交叉韧带生物力学止点重建理念,并建立手术模型。
中图分类号:
- R329.4


| [1] |
Kraeutler MJ, Wolsky RM, Vidal AF , et al. Anatomy and biomechanics of the native and reconstructed anterior cruciate ligament: surgical implications[J]. J Bone Joint Surg Am, 2017,99(5):438-445.
doi: 10.2106/JBJS.16.00754 |
| [2] | Lohmander LS, Englund PM, Dahl LL , et al. The long-term consequence of anterior cruciate ligament and meniscus injuries[J]. Am J Sports Med, 2017,35(10):1756-1769. |
| [3] |
Offerhaus C, Albers M, Nagai K , et al. Individualized anterior cruciate ligament graft matching: in vivo comparison of cross-sectional areas of hamstring, patellar, and quadriceps tendon grafts and ACL insertion area[J]. Am J Sports Med, 2018,46(11):2646-2652.
doi: 10.1177/0363546518786032 |
| [4] |
Siebold R, Schuhmacher P, Fernandez F , et al. Flat midsubstance of the anterior cruciate ligament with tibial “C”-shaped insertion site[J]. Knee Surg Sports Traumatol Arthrosc, 2015,23(11):3136-3142.
doi: 10.1007/s00167-014-3058-6 |
| [5] | Oka S, Schuhmacher P, Brehmer A , et al. Histological analysis of the tibial anterior cruciate ligament insertion[J]. Knee Surg Sports Traumatol Arthrosc, 2015,24(3):747-753. |
| [6] | 尤田, 张新涛, 张文涛 , 等. 中国成人前交叉韧带胫骨止点的解剖研究[J]. 中国修复重建外科杂志, 2015,29(6):730-733. |
| [7] |
Sasaki N, Ishibashi Y, Tsuda E , et al. The femoral insertion of the anterior cruciate ligament: discrepancy between macroscopic and histological observations[J]. Arthroscopy, 2012,28(8):1135-1146.
doi: 10.1016/j.arthro.2011.12.021 |
| [8] |
Tsukada H, Ishibashi Y, Tsuda E , et al. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints[J]. J Orthop Sci, 2008,13(2):122-129.
doi: 10.1007/s00776-007-1203-5 |
| [9] |
Noh JH, Yang BG, Roh YH , et al. Anterior cruciate ligament reconstruction using 4-strand hamstring autograft: conventional single-bundle technique versus oval-footprint technique[J]. Arthroscopy, 2011,27(11):1502-1510.
doi: 10.1016/j.arthro.2011.06.027 |
| [10] |
Shino K, Mae T, Nakamura N . Surgical technique: revision ACL reconstruction with a rectangular tunnel technique[J]. Clin Orthop Relat Res, 2012,470(3):843-852.
doi: 10.1007/s11999-011-1948-1 |
| [11] |
Petersen W, Forkel P, Achtnich A , et al. Technique of anatomical footprint reconstruction of the ACL with oval tunnels and medial portal aimers[J]. Arch Orthop Trauma Surg, 2013,133(6):827-833.
doi: 10.1007/s00402-013-1741-6 |
| [12] |
Nakase J, Toratani T, Kosaka M , et al. Technique of anatomical single bundle ACL reconstruction with rounded rectangle femoral dilator[J]. Knee, 2016,23(1):91-96.
doi: 10.1016/j.knee.2015.07.005 |
| [13] | 张家豪, 刘振龙, 胡晓青 , 等. 椭圆形骨道与圆形骨道重建膝关节前交叉韧带术后移植物成熟度对比研究[J]. 中国运动医学杂志, 2018,37(2):104-109. |
| [14] | 赵逢源, 史尉利, 张继英 , 等. 椭圆形骨道改良重建兔前交叉韧带动物模型的建立[J]. 中国运动医学杂志, 2017,36(4):300-305. |
| [15] |
Noyes FR . The function of the human anterior cruciate ligament and analysis of single- and double-bundle graft reconstructions[J]. Sports Health, 2009,1(1):66-75.
doi: 10.1177/1941738108326980 |
| [16] |
Vairis A, Stefanoudakis G, Petousis M , et al. Evaluation of an intact, an ACL-deficient, and a reconstructed human knee joint finite element model[J]. Comput Methods Biomech Biomed Engin, 2016,19(3):263-270.
doi: 10.1080/10255842.2015.1015526 |
| [17] |
LaPrade CM, Smith SD, Rasmussen MT , et al. Consequences of tibial tunnel reaming on the meniscal roots during cruciate ligament reconstruction in a cadaveric model, Part 1: The anterior cruciate ligament[J]. Am J Sports Med, 2015,43(1):200-206.
doi: 10.1177/0363546514554769 |
| [18] | 王健全, 敖英芳, 刘平 , 等. 前交叉韧带股骨止点临床解剖学研究[J]. 中国运动医学杂志, 2007,26(3):266-270. |
| [19] |
Tensho K, Shimodaira H, Aoki T , et al. Bony landmarks of the anterior cruciate ligament tibial footprint: a detailed analysis comparing 3-dimensional computed tomography images to visual and histological evaluations[J]. Am J Sports Med, 2014,42(6):1433-1440.
doi: 10.1177/0363546514528789 |
| [1] | 马丽娟, 腾雍辉, 王勇, 赵一姣, 张馨月, 秦庆钊, 尹东. 乳牙缺失数字化丝圈间隙保持器的三维有限元分析[J]. 北京大学学报(医学版), 2025, 57(2): 376-383. |
| [2] | 杨俊娟, 张蕾, 张龑. 妊娠合并脐尿管瘘1例[J]. 北京大学学报(医学版), 2025, 57(2): 393-395. |
| [3] | 胡轶博, 吕伟佳, 夏炜, 刘亦洪. 基于细胞生长与成骨分化的不同孔径生物支架流体力学有限元分析[J]. 北京大学学报(医学版), 2025, 57(1): 97-105. |
| [4] | 任爽, 时会娟, 梁子轩, 张思, 胡晓青, 黄红拾, 敖英芳. 前交叉韧带重建术后侧切动作的生物力学特征[J]. 北京大学学报(医学版), 2024, 56(5): 868-873. |
| [5] | 唐祖南,胡耒豪,陈震,于尧,章文博,彭歆. 增强现实技术在口腔颌面颈部解剖识别中的应用评价[J]. 北京大学学报(医学版), 2024, 56(3): 541-545. |
| [6] | 王江静,魏顺依,敖英芳,杨渝平. 前交叉韧带重建术后三种不同药物镇痛早期疗效的对比[J]. 北京大学学报(医学版), 2024, 56(2): 293-298. |
| [7] | 赵菡,卫彦,张学慧,杨小平,蔡晴,宁成云,徐明明,刘雯雯,黄颖,何颖,郭亚茹,江圣杰,白云洋,吴宇佳,郭雨思,郑晓娜,李文静,邓旭亮. 口腔硬组织修复材料仿生设计制备和临床转化[J]. 北京大学学报(医学版), 2024, 56(1): 4-8. |
| [8] | 张雯,刘筱菁,李自力,张益. 基于解剖标志的鼻翼基底缩窄缝合术对正颌患者术后鼻唇部形态的影响[J]. 北京大学学报(医学版), 2023, 55(4): 736-742. |
| [9] | 欧蒙恩,丁云,唐卫峰,周永胜. 基台边缘-牙冠的平台转移结构中粘接剂流动的三维有限元分析[J]. 北京大学学报(医学版), 2023, 55(3): 548-552. |
| [10] | 邱淑婷,弗朗斯,张晓,叶红强,刘云松. 口腔内窥镜在口腔解剖标志识别中的应用[J]. 北京大学学报(医学版), 2023, 55(1): 120-123. |
| [11] | 高梓翔,王勇,温奥楠,朱玉佳,秦庆钊,张昀,王晶,赵一姣. 基于三维下颌骨平均模型的颌骨标志点自动确定方法[J]. 北京大学学报(医学版), 2023, 55(1): 174-180. |
| [12] | 马珂楠,陈虎,沈妍汝,周永胜,王勇,孙玉春. 选择性激光熔化打印可摘局部义齿圆环形卡环固位力的有限元分析[J]. 北京大学学报(医学版), 2022, 54(1): 105-112. |
| [13] | 蒋艳芳,王健,王永健,刘佳,裴殷,刘晓鹏,敖英芳,马勇. 前交叉韧带翻修重建术后中长期临床疗效及影响因素[J]. 北京大学学报(医学版), 2021, 53(5): 857-863. |
| [14] | 任爽,时会娟,张家豪,刘振龙,邵嘉艺,朱敬先,胡晓青,黄红拾,敖英芳. 前交叉韧带重建术后移植物应力的有限元分析[J]. 北京大学学报(医学版), 2021, 53(5): 865-870. |
| [15] | 印钰,梅宇,王泽刚,宋首一,刘鹏飞,何鹏峰,武文杰,谢兴. 固定袢和可调节袢在粗骨道中的长度对股骨骨道增宽及膝关节功能的影响[J]. 北京大学学报(医学版), 2021, 53(5): 883-890. |
|
||
