北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (5): 913-918. doi: 10.19723/j.issn.1671-167X.2019.05.020
根分叉病变患牙经牙周非手术治疗后5年失牙状况及多因素分析
石姝雯1,孟洋2,焦剑1,李文静1,孟焕新1,△( ),栾庆先1,王万春2
),栾庆先1,王万春2
- 1. 北京大学口腔医学院·口腔医院,牙周科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
2. 青岛市口腔医院牙周科,山东青岛 266001
Tooth loss and multivariable analysis after 5-year non-surgical periodontal treatment on molars with furcation involvement
Shu-wen SHI1,Yang MENG2,Jian JIAO1,Wen-jing LI1,Huan-xin MENG1,△(),Qing-xian LUAN1,Wan-chun WANG2
- 1. Department of Periodontology, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
2. Department of Periodontology, Qingdao Stomatological Hospital, Qingdao 266001, Shandong, China
摘要:
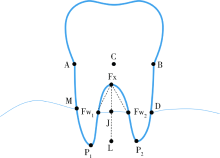
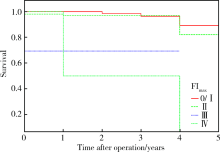
目的:观察根分叉病变患牙经牙周非手术治疗后5年的失牙状况及失牙的影响因素。方法:纳入79例就诊于北京大学口腔医院牙周科的慢性牙周炎患者,经牙周非手术治疗纵向观察5年。比较分析双侧下磨牙初诊及5年后随访时探诊深度(probing depth,PD)、出血指数(bleeding index,BI)、根分叉病变等级(furcation index,FI)、牙松动度等临床指标,并利用根尖片评价初诊时根分叉区牙槽骨吸收量,以了解根分叉病变患牙治疗前后临床指标的变化及失牙状况,并进一步分析影响失牙的主要因素。结果:(1)非手术治疗对伴有根分叉病变的慢性牙周炎患牙PD的改善是显著有效的,但根分叉病变的存在会影响其PD值的改善。(2)初始根分叉区PD值、松动度以及影像学根分叉区垂直骨丧失量和根分叉病变部位骨吸收区域面积与失牙成明显正相关(P<0.001),且FI=3、FI=4亦显著增加了失牙风险(P=0.017,P=0.007),而年龄(P=0.703)、性别(P=0.243)、吸烟史(P=0.895)等在本研究中与失牙无显著相关。(3)FI=3或FI=4的失牙风险显著高于FI为2及2以下的患牙,5年存活率不足50%。结论:根分叉病变患牙失牙风险与根分叉病变密切相关,根分叉病变严重、根分叉区水平及垂直骨丧失量多会显著增加失牙风险。
中图分类号:
- R781.42


| [1] | 孟焕新 . 临床牙周病学[M]. 2版. 北京: 北京大学医学出版社, 2014: 216-219. |
| [2] | 孟洋, 王万春, 栾庆先 . 根分叉病变发生、发展与治疗研究进展[J]. 中国实用口腔医学杂志, 2016,4(9):237-242. |
| [3] | Grover V, Malhotra R, Kapoor A , et al. Correlation of the interdental and the interradicular bone loss: A radiovisuographic analysis[J]. J Indian Soc Periodontol, 2014,18(4):482-487. |
| [4] | Dannewitz B, Krieger JK, Hüsing J , et al. Loss of molars in periodontally treated patients: A retrospective analysis five years or more after active periodontal treatment[J]. J Clin Periodontol, 2006,33(1):53-61. |
| [5] | Do Vale HF, Del Peloso Ribeiro E, Bittencourt S, et al. Radiographic characteristics of furcation involvements in mandibular molars as prognostic indicators of healing after nonsurgical periodontal therapy[J]. J Am Dent Assoc, 2009,140(4):434-440. |
| [6] | Mazza JE, Newman MG, Sims TN . Clinical and antimicrobial effect of stannous fluoride on periodontitis[J]. J Clin Periodontol, 1981,8(3):203-212. |
| [7] | Jiao J, Shi D, Cao ZQ , et al. Effectiveness of non-surgical periodontal therapy in a large Chinese population with chronic periodontitis[J]. J Clin Periodontol, 2017,44(1):42-50. |
| [8] | Hou GL, Hung CC, Tsai CC , et al. Topographic study of root trunk type on Chinese molars with Class Ⅲ furcation involvements: Molar type and furcation site[J]. Int J Periodontics Restorative Dent, 2005,25(2):173-179. |
| [9] | Bowers GM, Schallhorn RG, McClain PK, et al. Factors influen-cing the outcome of regenerative therapy in mandibular class Ⅱ furcations: Part Ⅰ[J]. J Periodontol, 2003,74(9):1255-1268. |
| [10] | James JR, Arun KV, Talwar A , et al. Mathematical analysis of furcation angle in extracted mandibular molars[J]. J Indian Soc Periodontol, 2013,17(1):68-71. |
| [11] | Faggion CM Jr, Petersilka G, Lange DE , et al. Prognostic model for tooth survival in patients treated for periodontitis[J]. J Clin Periodontol, 2007,34(3):226-231. |
| [12] | Checchi L, Montevecchi M, Gatto MR , et al. Retrospective study of tooth loss in 92 treated periodontal patients[J]. J Clin Perio-dontol, 2002,29(7):651-656. |
| [13] | Graetz C, Schützhold S, Plaumann A , et al. Prognostic factors for the loss of molars: An 18-years retrospective cohort study[J]. J Clin Periodontol, 2015,42(10):943-950. |
| [14] | Onabolu O, Donos N, Tu YK , et al. Periodontal progression based on radiographic records: An observational study in chronic and aggressive periodontitis[J]. J Dent, 2015,43(6):673-682. |
| [15] | 沈潇, 施捷, 徐莉 , 等. 伴错牙合畸形的侵袭性牙周炎患者牙周-正畸联合治疗的临床评价[J]. 北京大学学报(医学版), 2017,49(1):60-66. |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 王昕莹, 程雪原, 张孟钧, 李菲, 段晋瑜, 乔静. 浓缩生长因子联合引导性组织再生术治疗下颌磨牙根分叉病变的疗效[J]. 北京大学学报(医学版), 2026, 58(2): 372-379. |
| [4] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [7] | 包振英, 王雅杰. 炎症指标和细胞因子联合检测在慢性牙周炎中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 772-778. |
| [8] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [9] | 马丽娟, 腾雍辉, 王勇, 赵一姣, 张馨月, 秦庆钊, 尹东. 乳牙缺失数字化丝圈间隙保持器的三维有限元分析[J]. 北京大学学报(医学版), 2025, 57(2): 376-383. |
| [10] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [11] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [12] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [13] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [14] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [15] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
|
||
